Your Questions
Your Questions
Q: Dr. Eppley, I’m planning on getting a bbl as well and I was wondering if that had to be before or after rib removal. Thank you.
A: It makes the most sense to do it after the BBL surgery. See what you get out of the BBL surgery first before deciding whether rib removal is necessary.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a consult for hip augmentation by fat injection and was told I would need to gain weight for the surgery. Do you think I will have enough fat to do the procedure? Can the back between and around the shoulder blades be used for harvest? Is the use of postoperative compression helpful for making the fat survive better?
A: In answer to your questions:
1) Despite having gained weight the reality is that the amount of fat available for the hips is not going to ‘significant”. (but better than not gaining the weight) The term ‘skinny BBL’ is just a nice way of saying you really don’t have enough fat to do the surgery but we will do it anyway…just don’t expect much of a result. When you factor in the important concept of ‘halving’ when it comes to fat transfer the reality of the potential result becomes more apparent. (50% of what is harvested is removed for concentration, that amount is then split in half for each hip injection, and if one is lucky 50% or half will survive. (in the hips it will be less) Mathematically use 1,000cc of aspirate harvest (you will be very lucky to get that amount) and then cut it half for concentration (500cc), divide in half for each hip injection (250ccs) and then at best 50% will survive. (125cc)
2) The harvest sites are the abdomen and flanks. The back (shoulder blades) are not viable harvest sites.
3) No one knows how to make fat survive the best. Every doctor thinks they do. But the reality is that fat injection grafting is modern day alchemy. The biology of fat grafting by injection remains poorly understood in terms of what makes some fat cells survive and why others don’t. Thus postoperative compression vs non-compression is a perception not an established scientific method.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,If I would decide for testicle removal, do I have to inject only Testosterone till end of my life?
Or is there anything else that needs to be injected?
One more question: is the size 5.5 cm or 6 cm in the human shape?
(I saw some doctors use dog shape silicon testicles – I would like human shape).
A: Hormone management in the face of testicle removals is not my area of expertise. You would be well served to consult a Urologist to get accurate answers as to what the hormonal implications are with testicle removals and whether that is a wise medical decision.
All testicle implants that I have ever designed or used are in the human ratio of 0.7 width to length ratio. I have never heard of using ‘dog-shaped’ testicle implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Dr. Eppley is a very knowledgeable surgeon and I know he has a blog where he answers questions. I have a important question for dr. Eppley regarding revision rhinoplasty. I had a diced rib cartilage glue graft placed (dorsal onlay graft), however it looks way too big on my nose and is also wide. Is there a technique to remove this graft completely so that I can my original underlying bridge bone back?
A:That can be done. Such rib grafts heal by fibrous union so they can be safely dissected out for reduction or removal.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
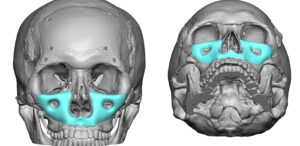 Q: Dr. Eppley, I had a LeFort I osteotomy to fix a recessed maxilla but it made the area above it recessed. Because of this, I’m interested in an extended custom midface implant for a LeFort III type augmentation, like the one in the picture attached, that I took from your blog (minus the area that the LeFort I fixed, obviously). If, down the road, I want an implant to augment my cheek-archs (like the one in the attached picture, that I also took from your blog), would it be possible to put them on top of the part that already has some of the extended custom midface implant? I know that it is possible to make a single implant for both areas, but I haven’t decided if I want to augment my cheek-archs. Thanks in advance.
Q: Dr. Eppley, I had a LeFort I osteotomy to fix a recessed maxilla but it made the area above it recessed. Because of this, I’m interested in an extended custom midface implant for a LeFort III type augmentation, like the one in the picture attached, that I took from your blog (minus the area that the LeFort I fixed, obviously). If, down the road, I want an implant to augment my cheek-archs (like the one in the attached picture, that I also took from your blog), would it be possible to put them on top of the part that already has some of the extended custom midface implant? I know that it is possible to make a single implant for both areas, but I haven’t decided if I want to augment my cheek-archs. Thanks in advance.
A:In answer to your midface augmentation questions:
1) If you have had a successful LeFort I osteotomy you may only need to augment the rest of the midface that lies above it. (see diagram)
2) An arch onlay implant could be laid over the midface implant secondarily.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in an upper vy lip advancement for both volume and elevation, but do not know if I am a good candidate. Also, would like to talk about the technique in general since so few docs do it — even though it seems like a great surgery. Curious as to risks and outcomes.
 A:You are not a good candidate for V-Y upper lip enhancement as you have a long upper lip. The V-Y procedure adds volume but can not elevate the lip or decrease the distance between the nose and the upper lip. With a good Cupid’s bow shape the more appropriate procedure for your upper lip enhancement is a subnasal lip lift combined with lateral vermilion advancements.
A:You are not a good candidate for V-Y upper lip enhancement as you have a long upper lip. The V-Y procedure adds volume but can not elevate the lip or decrease the distance between the nose and the upper lip. With a good Cupid’s bow shape the more appropriate procedure for your upper lip enhancement is a subnasal lip lift combined with lateral vermilion advancements.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,There are numerous places where I have seen you state that safe skull reduction cannot enter the diploic space, but in the case of this patient it appears you reduced his skull all the way down to the inner table – why is the diploic space the standard stopping point, and why was that rule able to be ignored in this instance?
A: What I always say is that skull reductions are taken down to the diploic space. You only find the diploic space by entering it. The diploic space is very thin so entering it usually means you are virtually through it. That is a good stopping point as the inner cranial table is now what is left…leaving some layer of bone over the underlying dura mater covering of the brain.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope you wouldn’t mind giving me some advice/thoughts. In 2022 I had bilateral gonial angle reduction and a bit of excess bone from middle of chin shaved off. Very happy with gonial angle reduction but the improvement in my front view wasn’t what I was hoping for.
Consulted a surgeon this year and underwent chin reduction – he cut 5mm off the chin point and narrowed it. Unfortunately, I’m very regretful of this, feeling like I needed that extra length to balance my face and feel chin looks too short and round. It is early after surgery and I still have some submental swelling. Aware I need to let things settle physically and mentally, however I have a few queries.
1. When would be a good time to have a repeat CBCT post surgery? ‘m keen to see what exact changes where made and where on the mandible and what can be done to restore my chin as closely to what it previously was.
2. Would a vertical lengthening genioplasty be an option? My original surgeon offered dermal filler.
3. What are your thoughts on custom made chin implants to restore the original shape and length of the chin? Would these be made using exact measurement differences of the bone from the pre and post surgery CT scans? I am 30 years old and healthy, would I likely need a repeat procedure in future if i was to get an implant?
Psychologically, I feel I prefer the permanent aspect of the genioplasty and the fact it is ‘replacing’ what I’ve taken off – bone. Appreciate I can’t turn back time and struggling with regret.
4. I am concerned, although have recovered well, about future intraoral incisions and effect on the mentalis muscle. Can a vertical lengthening genioplasty be done submentally?
I have included some photos. Many thanks for reading, and thank you for the information you share on your website, it has been by far my most helpful and informative source recently.
A: In answer to your questions:
1) Anytime is OK to get a 3D CT scan of your chin/lower jaw. The bone shape is not going to change with more healing time.
2) The only autologous approach to improvement would be a vertical lengthening genioplasty. I do not know how the previous reduction was done but the 3D scan will make that clear.
3) A custom chin implant is the non-autologous option as long as one can accept an implant to do it. Such implants are permanent., Unless you had a pre-reduction 3D CT scan that can be matched to the postop 3D CT scan there would be no way to know exactly how to do the ‘perfect’ restoration froma dimensionally standpoint. This applies to a vertical lengthening genioplasty as well.
4) The vertical lengthening bony genioplasty can not be done from a submental approach, only a custom chin implant can.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope this email finds you well. I am writing to inquire about the possibility of midface shortening surgery using the lefort principle, followed by a subnasal lip lift. I am aware that midface shortening surgery is a complex and unconventional procedure, and I understand the risks it carries.
I have been contemplating midface shortening surgery for roughly 5 years. While I understand that this procedure is not as common as some others, I am genuinely interested in exploring the possibilities it may offer in achieving a more balanced facial appearance, although I don’t bring the needed characteristics like a gummy smile etc. I am simply displeased with the aesthetic of my midface.
I am committed to making an informed decision about the surgery and would greatly appreciate the opportunity to schedule an online consultation with you. I want to emphasize that I am approaching this decision with realistic expectations and a strong commitment to my well-being. My primary objective is to be satisfied with the appearance of my face. If you would be open to discussing the possibility of midface shortening surgery with me, I would be grateful for the opportunity to meet online with you at your earliest convenience.
Thank you for taking the time to consider my inquiry.
A: Doing a LeFort I impaction is NOT going to shorten the external midface. That is a procedure that works only to decrease excessive tooth and gum show. And in the patient who has a normal tooth to lip relationship it will bury the upper front teeth under the upper lip creating an aged appearance.The only procedure that has any effect on vertical midface shortening is the subansal lip lift whose effect is limited to altering the distance between base of the nose and the upper lip.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a prominent supraorbital bone and I want to do supraorbital bone ( eyebrow bone shaving) Is it possible to shave or peel the excessive supraorbital bone by minimal invasive technique (endoscopic technique) because the problem that I have a baldness on the both sides of the head and I don’t want to have a long visible scar on my forehead. And is it possible to remove the excessive eyebrow bone by making an incision on the upper eyelid ( transpalpebral technique) in order to avoid the long visible scar the resulted from the conventional open method for the forehead rasping. Thanks
A: Your question about the access for any form of brow bone reduction is a good one and that is always the challenge in male brow bone reductions. Whether it is burring or bone flap setback the endoscopic and transpalpebral approaches will not work. There is no good instrumentation through the endoscope to make any significant brow bone reduction possible and the upper eyelid incision provides limited access to the brow bones because of the supraorbital nerves which are impossible to work around without permanent injury to them. Thus in many men the choices become a mid-forehead incision, which can work well if a horizontal wrinkle line is present, and a frontal hairline incision if the frontal hairline is not too far back.
I would agree that the typical coronal scalp incision is not an acceptable scar tradeoff for most men.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my son had a poorly performed otoplasty which resulted in excessive pinning of the middle third of both ears. We have been researching the cadaver cartilage bracing reverse otoplasty procedure and are curious what the recovery for that procedure would look like. How many months would the ears need to be protected during sleep? How have your other patients protected their postoperative ears during sleep? Any information is appreciated.
A:I have never done any special ‘protective’ maneuvers after a subtotal reversal otoplasty including any postoperative dressing…although to date these have all been in adults.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have lost a lot of weight but i need more hips and but, and BBL is not possible. What can de doctor suggest for me with visible results.
A: In thin patients like yourself, particularly after weight loss, buttock implants are possible but not hip implants as you don’t have enough tissue to support them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had scoliosis surgery 2.5 years ago and it was successful but still have a bit of a curve. My question is, do I qualify for the rib removal surgery? I have uneven waistline due to the curvature of the spine that I’d like to correct.
A: Having prior scoliosis surgery does not preclude one from having rib removal surgery later. From your inquiry it appears the goal would be to improve the waistline asymmetry which shows more fullness on the right side. This would indicate that only the right side needs to be done which could be approached from your midline spine surgery scar.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What would you say is the biggest change that went from when I was 16 to me right now at 23 ? Is it soft tissue (skin, fat pads) or bone changes ? I feel like my midface looks especially sunken now compare to before. I’d like to look like I did before (and ideally better) but I don’t know how. I’ll try to state my issues as clearly as possible:
-I believe that my midface looks sunken in from the front especially (and I’m talking about the lateral orbitals, infra/zygomatic region and paranasal area). I’m not sure if this is just in my head but if it’s not would I benefit from some type of lefort 3 surgery ?
-I feel like I have a long-ish midface (nose) or oversized nose and mouth relative to my midface. I’m not sure if this is an optical illusion.
-My jaw and chin seem recessed as well
Would you agree with my statements ? I would very much appreciate your insights, thank you kindly
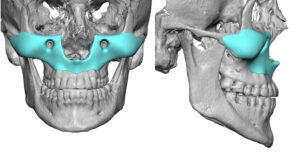 A: Since I don’t have any reference pictures from age 16 I can’t speak to a change. All I can speak to is that now your midface is flat. (lacks horizontal projecion from the orbital rims down)
A: Since I don’t have any reference pictures from age 16 I can’t speak to a change. All I can speak to is that now your midface is flat. (lacks horizontal projecion from the orbital rims down)
While you may be seeking a Lefort III effect that is not going to come from an osteotomy unless you have a significant Class III malocculsion…which you don’t. Thus any midface augmentation is going to need to be done by a custom midface mask implant. (see attached implant design example)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m very interested in infraorbital-malar implants, as well as potentially paranasal implants to improve my deficient midface after I have a LeFort I osteotomy and BSSO that’is scheduled later this year. So I’m writing this as I have two questions for you! First one is how long after should I wait to have a consultation about these implants due to residual swelling and the bones healing etc. In terms of getting the actual implant i’ve seen online that waiting 6 months after is enough although I will ask my surgeon specifically on that. But what I mean is to have the initial consult and get the process started in deciding on the implants and design? My second question is how the process in determining the appropriate sizing of the implants to get my desired result works? As having mild midface hypoplasia I believe I’d need larger implants but don’t really understand how the planning goes for it. Like I know what I would want my end result to look like and would be able to create that look in a picture with a sort of filter, but seeing pics of scans of the implant on my skull and measurements etc. is quite confusing to me on what it would actually look like on my face. I would hate for it to be too big, or too small and have to revise, which is why I’m curious how you go about that.
Thank you very much and hope to hear back soon!
A:In answer to your custom midface implant questions:
- You need to begin the process at any time since the implant design process takes 3 to 4 months and getting a surgery date may taken even longer.
- The implant design process requires a lot of learned experience to understand what shape and measurements on an implant design mean to an external facial change. This is a translation that no patient can really make with any accuracy…although some try. (and often fail with their chosen measurements) This is why patients should largely leave those design decisions up to me. Implant designing is not an exact science and is more of an art form.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I have for some time now been set on getting a chin implant. However, as the deadline for doing so is coming closer, I doubt whether I should opt for a custom implant or choose a standard chin implant. As you can see in the pictures attached I lack both vertical and horizontal length.The only option for a standard chin implant that can add vertical height, is the VLC-implant, designed by you.
I lack more than 12mm in horizontal length, which is why I would need to opt for the large VLC-implant. Though I am scared that this implant might be too big for me as it would also widen my chin area?
There are no surgeons in Denmark specialising in custom chin implants. I would, therefore, like to know whether I would be best off with a custom implant that gives me the same projection of a large VLC-implant without widening the chin so much or whether I could benefit aesthetically from the standard large VLC-implant.
A: When you have a combined vertical and horizontal chin augmentation with specific dimensional needs that are 12mm horizontal and some vertical lengthening (maybe 3mms) the choices are not between a standard and a custom implant. Rather the choices ae between a custom implant and a sliding genioplasty. Such dimensional changes can not be well achieved by the use of any standard chin implant. Quite frankly these dimensional changes are really at the outer limits of even a custom chin implant given the tightness of the overlying soft tissue chin pad.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I just came back from the dentist and have some periodontal disease (with no bone loss) due to having smoked when younger but have now quit. I was hoping to get jaw implants however I’m wondering if this could be an issue and could it increase the progression of gum disease? I have good oral hygiene habits now however I have some concerns about this.
Also I was wondering if the implant would be visible on dental x-rays and so if a dentist could make assessments about it in the future in case something started going wrong
A: A jaw implant will not cause worsening of any pre-existng periodontal disease nor interfere with any ongoing or future periodontal treatments.
The jaw implant itself is not visible on any standard dental x-rays although its fixation screws would be on a panorex x-ray. The jaw implant is only visible on 2D or 3D CT scans.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in temporal artery ligations. You seem to be the surgeon that comes up repeatedly for this procedure online so I am very interested in learning more.
– is this a common procedure for you? Do people routinely fly in for this?
– what are we looking at as far as scarring? Hairline vs forehead?
– sort of a strange question, may not be relevant but wanted to flag it – once litigated is there any potential that they could rupture, break etc.? I ask because I practice MMA and routinely get choked.
A: In answer to your temporal artery ligation questions:
1) While this is a common procedure in my practice, it is done by only a handful of surgeons around the world.
2) The small ligation sites heal inconspicuously. No one has ever requested or had a scar revision for any ligation site in over 100 patients treated (over 700 ligation sites)
3) Each site is double ligated so getting loose is not a concern. How that relates to MMA fighting and being choked out I can not say since I have never has such a patient before. But it does not seem like a problem given the multi-level ligations done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I previously got a lower jaw surgery as well as a sliding genioplasty for a total of 14mm of movement. I still have a weak chin, so wondering if Dr. Eppley would recommend a second genioplasty? For this second genioplasty, is it possible to do an additional say, 10mm? My initial genioplasty was 4mm. I am curious if there are risks with the second genioplasty, such as a limited amount of forward projection that can be done.
A: If the initial sliding genioplasty was only 4mms you should be able to have a second one for an additional 10mm movement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to know, is it possible to reduce the posterior zygomatic arch by 8 mm through a combination of an osteotomy and burring? Thank you!
A: Maybe. But it would require a 3D CT scan with measurements of the posterior arch and its temporal attachments to know for sure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have come to realize that my primary goal is to address the physical length of the area between my eyes and nose. I am dissatisfied with the elongated appearance of this specific region of my face, as it affects the overall balance and harmony of my facial features.
While exploring potential solutions, I have considered a rhinoplasty to achieve nose shortening. However, I am apprehensive that this may lead to an elongated distance between the bottom of my nose and the top of my lips (pilthrum). This outcome could potentially be corrected with a lip lift procedure, as you previously mentioned.
However, I have concerns about the physical position of my mouth after a lip lift, since the position of my mouth will appear too low, which prevents from the desired face shortening aesthetic I hope to achieve.
To provide you with a clearer understanding of my desired outcome, I will be including a visual representation portraying the practice itself. However, I want to emphasize that these pictures are overdramatized and intended to highlight the desired changes only. They do not represent my exact expectations. Additionally, I would greatly appreciate your expertise in exploring any other possibilities/ procedures that could effectively address the length of the area between my eyes and nose, while ensuring facial harmony.
Thank you for your time and consideration.
A: If I understand what you have described and illustrated you are trying to achieve a middle third of the face shortening…which is essentially impossible. This is a common question/goal of many patients but unlike the forehead (upper face) and the chin/jaw (lower face) can not be achieved because the soft tissue can never reduced no matter what happens to the underlying bone. (e.g., a Lefort impaction reduced tooth/gum show but the outside soft tissue does not change. Thus thus leaves only a shortneing rhinoplasty (tip rotation) and/or a lip lift as the only procedures that can alter the perception of the vertical length of the midface.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a cis woman and I have a very wide torso, my ribcage is very large, I would like to know if there is a way to remove ribs 11, 10, 9 and shave the ribs above without interfering with the subcostal nerve.
A: There are two surgical methods of torso narrowing via rib removal, the lateral approach and the vertical midline back approach.
In the lateral incisional approach ribs 10 and 11 can be removed as well as maybe part of 9. (depending on the location of the pleura) But at least rib 9 can be shaved down. Higher level ribs can be shaved down but the lateral incision needed to do so gets longer.
In the vertical midline back approach, which is used in weight loss patients or those who have loose back skin a vertical elliptical excision of back skin is done (which pulls the sides of the torso in considerably) and ribs 10 and 11 removed.
In either approach removal of the lateral border of the latissimus dorsi muscle is done which is another essential element of torso narrowing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my face is asymmetrical, the right side of my face is lower than the left and my right eye is lower than my left eye. I’m uncomfortable with this situation.I went to 3 plastic surgeons in my country and they said there is no solution .I found you after my research.Is there a solution for this situation?
A: You have a right facial asymmetry where the entire right face is lower than that of the left. This is the most apparent in the eye area because it is the most visually seen and the easiest to detect facial feature asymmetry. All affected facial areas can be improved, it is just a question of how much effort one wants to put into it. I ask all patients with facial asymmetry to make a priority list of facial features they want to improve from most important to least important.
Assuming that the eye asymmetry, known as vertical orbital dystopia (VOD), is at the top of the priorlty list, the combination of infraorbital rim-floor augmentation (to raise up the eye) with eyelid adjustments around it is how it is treated.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve had two past skull implantation surgeries with you in the past few years. I would like to find out if a third implant is possible and set up a virtual consultation. I hope to hear from you soon. Thank you.
A: Good to hear from you. It has been two years since your 2nd skull implant. Your last skull implant, placed in 2021, was 260ccs. That is a very large skull implant for the back of the head. The question is not whether a larger skull implant can be placed but how much bigger can it accommodate. The amount of implant size increase with each subsequent implant replacement becomes less. I think the last volume increase (implant 1 to 2) was a 100% change. That would be far less incremental change this time. (implant 2 to 3, 25% increase)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have been looking for information about this operation for a very long time, but there is so little of it on the Internet. As a result, I made a correction of the ribs, my ribs were broken and I wore a corset for 3 months, 24/7. The first 2 weeks it was very tight, and later I wore it in these conditions so that they would take the desired position. Do you know about this operation? But this is not the result that I would like, there was a strong rollback. As soon as I took off the corset, I really liked it, but the result did not last, and I had such a painful rehabilitation, I took strong painkillers for a month and hardly walked because of back pain and tension with a corset. tell me, after the removal of the ribs, what kind of rehabilitation? How long will I need to stay in the clinic and in the city? Will I be able to fly in 2-3 weeks on a regular flight or will I need to buy business class tickets? Please tell me more about this operation, narrow waist is my dream.
A: You are referring to the ‘rib fracture’ technique which often does not work well in the long term. While I am familiar with that technique it is not what I use. My technique is a RIB REMOVAL method in which the outer halfs of ribs 11 and 12 as well as part of 10 PLUS latissimus dorsi muscle removal is done for a more effective and sustained result.
Pain rehabilitation is NOT part of the rib removal recovery in my experience. The recovery you have described for the rib fracture method is not what my patients report with the rib removal method. You should be able to return home in 3 to 5 days after the surgery.
To learn extensive details about rib removal surgery go to www.exploreplasticsurgery.com and place the words RIB REMOVAL in the search box on the homepage. Every article I have written on this subject will be listed there.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is there a visual of some kind I could see to understand how the implants “wrap around” the bone? Do they fold around the bone or actually wrap around, like rope?
Are they permanent? Can the surgery be done under local anesthesia? What are the risks involved?
Thanks so much.
 A: Clavicle augmentation would be done by a sleeve concept where the tubular implant fits around the clavicle over its mid-shaft portion before it turns into the sternal and acromial heads. (see attached) Think of a tube that is opened up along its length and this is wrapped around a smaller tube. (clavicle) This would be done through a small 2.5cm incision in the supraclavicular fossa. Implants would be designed off of a female clavicle model. The slit on one side of the implant allows for size adjustment. Such implant augmentations are permanent (meaning they last forever) but also easily reversible. I would not do the surgery under local, this procedure requires an anesthesia.
A: Clavicle augmentation would be done by a sleeve concept where the tubular implant fits around the clavicle over its mid-shaft portion before it turns into the sternal and acromial heads. (see attached) Think of a tube that is opened up along its length and this is wrapped around a smaller tube. (clavicle) This would be done through a small 2.5cm incision in the supraclavicular fossa. Implants would be designed off of a female clavicle model. The slit on one side of the implant allows for size adjustment. Such implant augmentations are permanent (meaning they last forever) but also easily reversible. I would not do the surgery under local, this procedure requires an anesthesia.
The risks of surgery would be like any other implant surgery…small scars, infection, transitional edging, too big/too small size.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What is the projection angle of iliac crest in reference to the spine? Would you say 45 degrees? The reason for my question is that I am trying to understand how much the iliac implant will add lateral prominence and height to the pelvic bones. Will the implant narrow the gap between the iliac crest and rib cage?
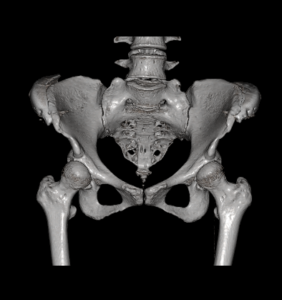 A: 45 degrees would be accurate assessment of the angulation of iliac crest implants on the bone.(see attached 3D CT scan) At a 45 degree angulation it would be fair to say that it would reduce the vertical distance between the new crest position and the 12th rib.
A: 45 degrees would be accurate assessment of the angulation of iliac crest implants on the bone.(see attached 3D CT scan) At a 45 degree angulation it would be fair to say that it would reduce the vertical distance between the new crest position and the 12th rib.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I considered getting custom silicone jawline implant but in the end I got the medpor implants in my home country. I got RZ mandibular angle 11mm, and RZ extended square chin implant (5mm) The op took place 7 mounths ago. The implants were fixated with titanium screws. Choose of the implants was meant do get so caled “wraparound” or “matrix” effect.
The operation went succesful exept one thing – propably due to the natural assymetry of the lower part of my face, or wrong placement done by the surgeon – I endend up with crooked chin, more specific, the left side of my lower face is somehow more portruded than the right side, it’s seems too rounded, which causes the left jaw implant look so out of place, so unnatural, like a result or swelling, while the right side creates a natural looking straight line. As I said I don’t know the exact cause of this result, the implant either shifted or it’s the left wing of an Implant, which causes too much projection, but I pressume the reason behind this is the lack of implant customization before inserting it, and it made my face look even more assymetrical than before. I’m writing this because you have had many experiences with medpor implant removal, and I wanted to ask a few questions about possible correction:
1) Can a medpor implant be safely trimmed through the intraoral/skin incision or does it have to be removed, trimmed and inserted again? Is it a saw or scalpel to be used to shave it down?
2) – If my case requires implant removal/replacement – Because of long size of the chin implant wings, my chin implant lays partially over mandibular implants, as the wings reach the jaw angles. Are these three implants became commecected due to the tissue ingrowth? And If they did, could future chin implant correction or removal be dangerous to jaw angle implants?
3) After one side of an implant is shaved down, weather 2 or 3mm, or completely, could it somehow cause the middle and right side to shift, due to lack of balance?
4) If chirurgical intervention were too risky, could it be treated with HA dermal fillers to achieve facial symmetry?
Best regards and thank you in advance for your answers
A: When using standard implants to create a total jawline augmentation effect the question is not whether there will be asymmetry, as there always will be, but how significant will it be and how will it needed to be treated.
In answer to your questions:
1) Medpor implants will need to be removed, modified and reinserted.
2) The jaw angle implant can be removed despite the wing of the chin implant overlying it.
3) No.
4) Injectable fillers can always be used to help with the asymmetry of any paired set of facial implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to add bone to the orbital rim, with something like hydroxyapatite? I’m talking about the upper orbital rim, rather than something like infraorbital rim implants.
A: Hydroxapatite, a synthetic ceramic material and not bone, can certainly be added to the brow bones or superior orbital rims…but it would require a full coronal scalp incision to do so. This is why brow bone implants, which can be done through a small scalp incision using an endoscopic technique, is usually preferred.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 24 year old male with a vertical lengthening chin implant (size medium). Unfortunately, I have visible ridges from the implant and I still desire more vertical augmentation. I had a few questions about genioplasty and scheduling surgery.
1. Does Eppley still perform vertical lengthening genioplasty of 10-14mms?
2. Does Eppley prefer to use iliac crest or cadaver bone for vertical lengthening genioplasty? How much do these grafting options tend to add on to cost?
3. Can the chin be widened during genioplasty? Not changing the shape of the chin, but widening the natural chin.
A: In answer to your vertical chin lengthening questions:
- I have done vertical chin lengthening osteotomies up to 20mms.
- While one’s own one can be used as the interpositional graft most patients opt for the cadaveric corticocancellous block graft.
- While chin widening osteotomies can be done, doing so at the same time as a significant vertical lengthening procedure is not recommended. This create unstable bone segments that are hard to fixate.
Dr. Barry Eppley
World-Renowned Plastic Surgeon