Your Questions
Your Questions
Q: Dr. Eppley, Hello. I saw on your web site a procedure you’ve had success treating angular chelitis. It involves the corner of the mouth. Is that the only area that’s focused on? In other words would it be necessary to raise the upper lip too? I’m trying to find the least invasive, yet effective, treatment.
A: The success in surgically curing angular cheilitis is to remove all chronically infected mucosa and skin. How that may affect the shape of the corner of the mouth depends on the infected/resected area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am soon going to undergo maxillomandibular advancement. I currently have an optimal amount of tooth show. In the post-op simulation, my philtrum lengthens a bit. I suspect this is due to the advancement vector being a little downward relative to my natural head position (which is about 6.5 degrees downward from the frankfurt plane). I am not yet certain this will look bad, but I have always had a strong dislike for long as well as convex philtrums. I am wondering:
1. Is it possible to shorten the philtrum without increasing tooth show? I find mixed answers when it comes to this.
2. Is it possible to turn a concave philtrum convex again, also without altering tooth show?
Depending on the effect of my maxillomandibular advancement on the philtrum, I may be interested in one or both of these.
I look forward to hearing your response.
A: In my experience 1) No and 2) No.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi. If I had cheek bone reduction and too much of the bone was cut off. Is it possible to get cheekbone implants? I’ve lost so much volume so my face is saggy and I have extra skin. My smile changed as well
A: The typical subtotal or total cheekbone reduction reversal is to use implants to build the cheekbones back out. This is best done with a custom implant design to control the amount of augmentation and to address any bony asymmetries which now may exist.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a consultation for possibly a lower eyelid pinch procedure. I am 32 years old and am experiencing extra skin that Botox is only making worse. My smile pull is a rather large area from cheek to brow.
A: No form of a lower lid blepharoplasty is going to help get rid of wrinkles thaf primarily appear in animation. (smling) Surgery treats static problems not dynamic ones. While you have a small amount of redundant lower eyelid skin (with scleral show) its removal is not going to make much a difference in the wrinklers while smiling. Those wrinkles appear because of the push of the cheek tissues upward.
While there may be some modest benefit to a lower eyelid pinch bleph and TCA lid peel, it is important to realize what that procedure does and does not achieve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve recently seen a question online asked by a user in regards to a midface shortening surgery using the lefort practice. You responded that such a surgery would not help since this would just burry the teeth if there were no abnormally long gums to begin with.
Now to my question. Would a lefort 1 for example make sense if the outside skin or soft tissue could be removed from the above the lip, for example cut a bit of an area from above the lip then sow it back to the upper lip, or would a bullhorn liplift be enough to reduce the soft tissue for it to look normal?
i understand that im not a professional but i think if only about 0,5cms of bone are removed it would be manageable, no?
A: While you can shorten the upper lip that will do nothing for the rest of the midface. In short there is nothing thaf can be done to shorten the long external midface. A LeFort I impaction reduces excessive gum show of the upper teeth but will not change the long external soft tissue midface.
Changing facial dimensions involves more variables than a diagrammatic exercise on a skeletal model. The effects on the external soft tissues do not correlate on a linear basis to what is done on the bone…and in the case of the midface bone shortening these is virtually no effect at all.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello! I saw a thread before regarding a question about having dents in the forehead.I have several dents in the forehead. The first one is quite big and is located in the middle. Its like a U: in the middle of the forehead. Then I have one more in the middle that is like a bullet hole and one on the left side which makes the whole forehead uneven. What can be done here to make it look more normal
A:You have two forehead treatment options, fat injections and a custom thin forehead implant to smooth the whole forehead out. Each one has its advantages and disadvantages.
FAT = autologous, minimally invasive but unpredictable survival and persistence
IMPLANT = permanent, smoothest result but it is an implant that has to be surgically placed
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I saw that you’re doing mouth widening surgery and I have some question about it. Actually I’ve not so wide mouth, and that’s bothering me in many ways. Does mouth widening increases opening of the mouth? I can open my mouth 4cm would be nice to open more than 5cm. I’ve not so small face and my lips doesn’t fit my face too, have juicy lips but small mouth.
A: Mouth widening surgery is an aesthetic procedure that lengths the width of the mouth. It will have no functional improvements in how far the mouth opens…which is controlled primarily by lower jaw motion not that of the lips.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a genioplasty, jaw shaving and facelift done 5 years ago. I was hoping to have revision work done to make the chin a little smaller to match the jawline and have the chin ptsosis corrected and the skin under the neck tightened.
A:While I don’t know what your chin bone looks like the anatomic reality is that the thickness of the overlying soft tissues is the limiting factor in any further chin reduction. This is evident with the presence of the existing chin ptosis. (too much soft tissue for the amount of bone that now exists). While submental chin ptosis correction may be effective I wouldn’t count on the chin getting much smaller.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 34 year old male and previously a few years back underwent forehead contouring surgery and fat grafting to the parasagittal areas of the skull (simultaneously) to correct a minor u treated case of craniosynostosis from childhood.
On the right sight of my skull in the parasagittal area, some of the fat grafts either did not take and/or were not distributed evenly because there is a slight concave area which is somewhat noticeable when my hair is cut very short. I previously had an injection of bellafil to correct that spot and I was supposed to go back for more but then ended up relocating to here in the bay area. I would like to correct the rest of that spot if possible.
You can’t see it in a picture really but I attached a photo circling in red the outline of where the concavity is.
I was wondering what options there could be to smooth the concavity and fill the “indented” area. I know there’s fat grafting, spot cranioplasty with bon cement, fillers etc, many of which you offer. I’m wondering what would be effective and also cost efficient?
A: An implant augmentation of some form is going to produce the reliable and sustained effect. A custom skull implant would produce the most effective result. ePTFE sheeting would provide the most cost efficient approach although the aesthetic outcome may not be quite as good as a custom skull implant..
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Thank you for confirming the suspicion. I see now that it was positioned as a standard chin implant rather than how a VLC implant is designed to be placed. Since the implant is positioned incorrectly, how much vertical height (if any) do you think it is giving me currently? The edit looks much better than what I have now. I am most interested in improving my frontal view the most; I was wondering if you could send an edit of the frontal view photo (if it is not too much trouble). I want a look that is similar to the lower thirds of the reference photos that you and I reviewed. One of my main fears is that I won’t be able to achieve the vertical length of those photos without an 8mm+ movement. Ideally, I’d prefer an implant over genioplasty because of the invasiveness, but I’d like your opinion on the most appropriate procedure knowing what we know now.
I have a few questions:
1) How much vertical movement do you think that I would need to achievethe height in the goal photos?
2) What is the maximum vertical and horizontal projections of a custom vertical lengthening chin implant?
3) How much more vertical length can I get from a custom chin implant in comparison to the VLC standard that I have in?
4) Taking my goal photo references into account, which procedure(s)would you recommend most to achieve my goals? My options are: modifying the existing VLC implant, vertical lengthening genioplasty w/ standard chin implant overlay, and a custom chin implant with an extended wing design.
A: In answer to your vertical chin lengthening questions:
1) Probably 5 to 7mms vertical
2) The tissue tolerances of the soft tissue chin pad for any implant augmentation is the number 12mms. (any amount of horizontal and vertical changes when added together)
3) It doesn’t matter whether it is custom or a standard chin implant you can not usually exceed the 12mm number)
4) Based on the information I know I would choose the custom extended chin implant. Then you control all variables including how it blends into the jawline behind the chin.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to enquire about a cosmetic ‘lip commisuroplasty’ to make the mouth less wide. I plan to get cosmetic surgeries to make my overall face smaller, but when I edit my face my wide mouth looks awkward. I’m not a fan of large lips and don’t want my mouth to stand out. I hope to make my mouth 2-3mm thinner if possible. How does this surgery work? Where and how large is the scar? Thanks in advance.
A:You are referring to a mouth narrowing procedure as opposed to a lip reduction procedure. This is done by a V-Y corner movement technique. This is the opposite of the Y-V mouth widening technique. Normally I am not in favor of mouth narrowing surgery because the scar trail left behind by the corner moving inward. (the straight line of the Y-closure) But for a 2 to 3mm change such a scar line may be more acceptable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in having cheekbone reduction surgery. Approximately 1.5 years ago, I had the procedure performed by another surgeon. The results weren’t what I wanted. He didn’t remove enough bone. So I am thinking of having a revision done but with you. If at all possible, that is. I’m not sure if a revision can be done for this type of surgery. I keep reading conflicting information online. At any rate, how would you approach such a procedure? Would I need extensive bone work done again via osteotomy? Or can the bones near the temple be shaved down for a simpler/safer approach? Also, what will the risks be?
I’ve attached pre-op and post-op photos, including a recent photograph of myself and a model whose cheekbones are what I hope to achieve. Hopefully, they help you in determining my options. Have a nice day, doctor. Thank you.
A:Thank you for your inquiry sending your pictures and 3D CT scans. I would agree that the only way to get closer to your result is further cheekbone reduction. Since there is no effective cheek shaving procedure that leaves the type of cheekbone reduction osteotomies you had done the first time. Since I don’t know how much inward movement was done we have to look at the scans to make that determination and see if more can be achieved. The views that will provide that information are either the top or basal (submental) views. This allows one to see how much inward movement was done. Those are the key views that are not in the 3D images that you have sent.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I had brow bone reduction surgery done 3 years ago. I love the results since my bone was very prominent and unattractive although I have been feeling my forehead area is less masculine now and wanted to see if it was possible to contour with slight augmentation. Please let me know if this is possible! I am a 31 year old male.
A: Secondary brow bone augmentation can always be done after a brow bone reduction. The only question is what material to use to do so which is yet to be determined.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am contacting you about clavicle widening surgery – I have very narrow clavicles that feel tight and cause my shoulders to roll forward. I’m wondering if there’s potential for therapeutic benefit to clavicle lengthening surgery in addition to aesthetic improvements. Also wondering how much lengthening is achievable, long term effects on shoulder health and exercises, cost, and wether you have more before/after photos to share from previous patients.
A:I am not very enthusiastic about clavicle lengthening surgery as it has a variety of issues, the most noteworthy of which is the limitations of lengthening due to the restrictions imposed by the soft tissues of the shoulder. What clavicle lengthening does is push the shoulders out and back. (improving the rolled in appearance) The issue is whether a 15 to 18mm lengthening per side justifies the effort…which is hard to imagine it would for most patients.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m 56 years old and going bald, so I would like to shave my head. However I have a bit of CVG (cutis verticis gyrata) on the crown of my head that I’m not very keen on showing off. I would like to discuss my options of what could be done to get a smooth scalp so I can shave.
A: The only two treatment options for scalp CVG are excision and release with fat injections. Generally deep inverted v-shaped CVG lines are best treated by excisions. Less inverted more shallow ones are treated by fat injections….which appears to be what your one submitted picture shows.
An achievable goal is to lessen their prominence/visibility. I would be cautions about expecting a perfeclly smooth scalp contour.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a male, 34 years old. I’ll attach an image, like I said, the sliding genioplasty movement was subtle (3 mm plus the titanium plate) and I’d like to reverse it without making the front look longer vertically if possible.
A:Thank you for the surgical information. From that I gather you had a small (3mm) advancement bony genioplasty but don’t like the result as it has made your chin vertically longer. This most commonly can happen if the chin is inadvertently plated with an opening wedge. (tilted down) It is unusual to have this occur with such a small advancement but that would be the only way it could happen. This then makes the options two fold: 1) complete reversal back to where you started, or 2) change the tilt of the chin upward to eliminate the vertical lengthening. I mention the latter since there was a reason you had the surgery in the first place and this option allows the benefits (horizontal augmentation) to be maintained but the liability of the vertical lengthening eliminated. For either option it would be important to have a postoperative x-ray (e.g., simple panorex or lateral ceph) before doing a secondary procedure to fully understand where the chin bone is now and what the indwelling hardware looks like.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have bad dental occlusion, and I am currently using braces to correct my bite, would this be able to reduce the temporalis muscle of the head? Does malocclusion increase the head muscle?
A:No form of occlusal management or change is going to change the size of the temporalis muscles. Only Botox or temporal reduction surgery can.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I previously had an occipital knob surgery with you and I was very pleased with the surgery, so I wanted to reach out about a potential other surgery; this one is likely much more minor though. Without going into a lot of detail for now, I wanted to see if you are able to fully remove this football shaped injury from my head and make it a single linear scar, or other clean scar (T-shape, etc.)? My skin below the wound is fairly lax, so it may be able to stretch further up. Thank you.
A:In regards to your current scalp injury I would be very cautious about considering any type of scalp excision based on the pattern drawn in the pictures. The scalp may seem lax but such excisions will result in a considerable scar widening…which may be worse than the original problem. The question is not whether it can be cut out and closed but how does the scar look later. Given that this looks like a fresh injury I would let this heal for at least 3 months and then let’s see what it looks like. But based on what I see now such an excision would not be recommended.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello! I’m curious about chin implants. I just got a anatomical implant in and it definitely helped with my projection, but I’d like it to be projected more. The doctor said we wouldn’t be able to do that since with the implants my face would get more oblong as well. Is this true? The angle of my mandible does go out and down, but is there a way to have the implant only provide lateral projection without it looking weird? How much would a custom implant be?
A:My answers to his questions are:
- It would be ill advised to provide comments on one’s prior surgery and any subsequent recommendations based on a description alone. I would need before and after pictures from your chin implant surgery as well as the operative note from that surgery to provide an informed opinion as to how to make further lower jaw augmentations that are in line with your goals.
- The advantage in custom implants is that you make an implant design any way it needs to be made to achieve the patient’s goals. The key is understanding what the patient’s goals are. That require computer imaging of current facial pictures.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, As a baby, I developed plagiocephaly which unfortunately to this day I still have a flat head and asymmetrical face.
I think because of the way my skull became deformed, it caused my face / forehead to go asymmetrical. My face looks completely different from each side.
This is something I have been very insecure about for most my life and was wondering if you could please provide a quotation for the implant surgery and any other information.
A:As is typical of plagiocephaly, more accurately described anatomically as cranioscoliosis, the entire skull and face is affected to varying degrees. Usually the most affected is the flat back of the head with lesser degrees of asymmetry of the forehead and face. In treating plagiocephaly in adults the common area treated is the flat back of the head with a custom skull implant…as you have described as an interest. While is done in the face varies considerably based on what components of the face bother them as well as how effective any surgery is for it. That is yet to be determined in your case.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope you’re all well. I’ve just had a revision of my initial Facial Feminisation at another clinic but I have a problem with the appearance of my eyes. One appears hollow and the other more smooth. I’d like to book an online consultation with Dr Eppley, or at least humbly request his feedback for my particular case. Please see the attached images.
I present the following images and I am grateful for any insight he is able to provide. Depending on this, I’d be willing to travel to an in-person consultation if needs be.
A:While I don’t know what you looked like beforehand the 3D CT scan clearly shows the less forward projection of the right tail of the brow, lateral orbital wall, infraorbital rim and cheek. Since not all of these changes could have occurred from the surgery, as only the teil of the brow bone was reduced ,this indicates that much of this bony asymmetry existed beforehand. Thus the brow bone reduction has now made this asymmetry more visually evident as the brow bone support has been removed both horizontally and vertically. Logic would then dictate that restoring some tail of the brow bone would be helpful in decreasing the orbital asymmetry. Such tail of the brow bone augmentation could be done by a transpalpebal (upper eyelid) approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I am thinking to get skull reshaping surgery because back and top of my head is flat. I have two questions.
1- are you using IV sedation for the surgery or general Anesthesia in your clinic?
2- are you using the MMA implants or silicone implants for the surgery?
A: In answer to your questions:
- General anesthesia is used for all skull reshaping surgery. These are not procedures that can be done under any other form of anesthesia.
- Custom skull implants is the far superior method skull augmentation. The use of PMMA bone cement is an historic and poor method of onlay skull augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope this message finds you well. I’ve been considering the possibility of a skull implant to increase my height by 2 inches and make my face wider. I’ve noticed that my head is slightly smaller in proportion to my body, and I believe this procedure could help me achieve the desired results that can help me with my professional career and finding balance in my body proportion.
Before proceeding, I would like to inquire about the safety of such a procedure. Additionally, as it’s important for my job, I’d like to know if this procedure is compatible with my lifestyle and if there are any potential risks or side effects I should be aware of. I’m a professional dancer and my lifestyle is very active.
Your professional guidance on this matter is of utmost importance to me, and I would be grateful for your advice.
A:The main comment I would to your inquiry is that it is not possible to be able to increase the height of the skull by 2 inches (50mms) without an undue risk of complications. With scalp tissue expansion one inch (25mms) is reasonable and with a low risk of complications but not 50mms of added height.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi reaching out because I am considering forehead reshaping/ contouring within the next year, but I have a very prominent protruding forehead and don’t know how possible it is. Was wondering I could send a picture to get an idea if this is even possible?
A:Thank you for your inquiry and sending your pictures. Like many patients with frontal bossing you also have a high long forehead (brow-frontal hairline distance) which exacerbates the appearance of the forehead protrusion. While frontal bossing reduction can be done it is important to realize that the forehead bone is not that thick so there are limits as to how much of the convexity can be reduced. (see attached imaging) There is also the issue on how to get there to do the reduction (incision placement but that is for a later discussion.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, So this is my x ray and I’m wondering if the implant can be placed at this angle? Instead of following the angle of the mandible downwards, my doctor said he had to place it at the same angle as the mandible (which also elongates my face).
What are your thoughts? I like the result, but I’d like a little more projection (enough to where my chin lines up with my bottom lip)
A: In your case of chin augmentation you absolutely do not want to elongate your chin. You either have a sliding genioplasty that moves the chin upward as it comes forward or you place an implant higher up on the bone. Be aware that all standard implants have their greatest projection on the lower half of the implant so moving the implant up further on the bone is not a guarantee that some elongation will not occur due to soft tissue chin pad rollout. (which is how chin implants create their effect) If you put the chin implant too high then some horizontal projection is lost and it may create a bump effect up to high in the chin. You have to be wary of trying to use a standard implant in a way that it was not designed to be used.
Biut as a general statement having to place the implant in line with the mandibular plane angle shows la ack of understanding that aesthetic consequence or full knowledge of chin implant placement techniques.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am looking to reverse a genioplasty that I had done last year. I am a 34 yr old male, basically I had an 8mm advancement a couple of years ago which in hindsight I did not really need. I got it reversed to 3 or 4mm but I still did not like the outcome. I realize that at this point it will never be back to the way it used to look but I would be content with close enough. I know Dr. Eppley is one of the few experts in this area and I wanted to see if he could reverse the 3mm, I also still have the titanium plates and screws attached.
The main issue that I had after this procedure is how I look from the front. It seems narrower, and my lower lip appears a little bit rolled in and less full like before. I know 3mm seem insignificant but in my case I have a small mouth and do not feel like a bigger chin fits my face
A: A full sliding genioplasty reversal can be completed. Whether the existing plate and screws can be used to stabilize the fully flush bone edges remains to be determined intraoperatively.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I would like to change my face shape. My primary concern is my chin. It’s short but too wide/prominent at the same time. I also would like to contour my face so that I have more prominent cheekbones and less fatty cheeks. I love my jaw but I wish it was more defined, without adding more mass. I’ve attached pictures of myself and the face shape I’d like to have. What would you recommend? Thanks so much in advance.
A: Most of your facial reshaping goals are contradictory and can not be achieved. For example to make a wide chin more narrow it must come forward along with being narrowed. Also you can’t make the jaw more defined with adding mass/volume. In essence you not factoring in the effects of the overlying soft tissues which can not be changed/reduced. Thus having a more defined facial shape comes from stretching out the soft tissues to better see the bone shape through the overlying soft tissues. You simply can not reduce facial structure into a more defined shape with your facial soft tissue thickness. In short you can’t take your facial shape and make it look like your ideal images… that is simply not going to happen no matter what type of surgery is done. To get a more defined facial shape you have to accept that more structural support (implant) that needs to be added to do so. With that comes more chin projection and some jaw width.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope your well. I am writing to you in regards to having a few questions about custom forehead, temporal widening implant as I am interested in getting this procedure done .
Lastly, I would love to see some before and after pictures to get a better understanding of what I could expect.
A: You are going to find it very hard to find any before and after pictures due to patient confidentiality. Most young people, who make up the majority of custom facial implant patients, are exquisitely sensitized of having their face shown in any capacity…..most likely how you might feel as well.
But in designing custom forehead-temporal implants what results other patients have is not all thaf relevant since every custom design is unique in its shape and thicknesses based on the patient’s aesthetic desires. Such implant designs are based on initially doing imaging of the patient’s pictures to determine their specific aesthetic goals. (known as setting the target) That is how you find out what the aesthetic outcome may be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a couple of questions regarding clavicle lengthening surgery.
Firstly, it appears on your social media that clavicle shortening* is far more prevalent? Is there a reason for this? Are there additional cases of lengthening that can be shared or perhaps a follow up photo of the bodybuilder from your article https://exploreplasticsurgery.com/plastic-surgery-case-study-shoulder-widening-by-clavicle-lengthening-in-a-muscular-male/
Secondly my question is regarding the procedure itself. I’m happy to see that you offer a sagittal split cut for increased stability and thickness. As surgeons often use ground cow bone powder for grafting purposes in surgery, I would like to know if it is possible to use human bone as a solid graft for the same purpose? For example in the saggital split, the two gaps created need to be filled with bone putty. It is possible to completely clean out a donated piece of clavicle from another human for the purposes of placing this in the gap instead of bone putty? This would act to physically prevent relapse/the clavicles sliding backwards and presumable be far more stable than putty.
If this is the case, then can the same graft be applied to a single osteotomy in the middle of the clavicle as opposed to a saggital cut?
Thank you and kind regards,
A: In answer to your clavicle lengthening questions:
1) Clavicle reductions are performed in far greater numbers because there is a greater medical need as well as being a surgery that is more effective and with a much lower risk of complications.
2) As for grafting the bone defects in the lengthened clavicle bone demineralized human bone particles is the most common graft material used in my experience. Other options include human cadaveric corticocancellous blocks as well as the patient’s own bone.
3) The reality is that clavicle lengthening has two distinct features that make it far more problematiic than clavicle shortenng in my experience. First to lengthen the clavicle you have to push out all of the shoulder soft tissue aftachments so the bone can lengthen. This not only is not easy but limiting in the lengthening amount possible. While clavicle reductions can easily shorten the bone 2.5cms or greater per side the maximum lengthening is around 1.5cms per side. Secondly, and a major issue, is that in the lengthened clavicle the shoulder soft tissues act like a fulcrum pushing down across the osteotomy site…often bending even a 3.5mm rigid plate. In short the biomechanical forces applied to the clavicle bone are very different between lengthening vs shortening.
3) Compared to the issues in #3, the choice of bone graft is the least important element in the whole clavicle lengthening process. If the expanded bone can not be maintained structurally stable in the short term the long term effects of the different types of bone grafts are irrelevant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Thank you very much for your reply, and for taking the time to do the imaging! After investigating the matter in greater depth, and taking into account your feedback and the imaging, here are some thoughts that may help to advance the discussion:
– It would appear that the lack of “strength” I perceive is a result of jaws that are a bit recessed, although not to a degree where they have caused any problems that I am aware of. However, since the issue is merely aesthetic, I question the wisdom of undergoing an aggressive treatment like DJS.
– I believe that chin projection is okay as it is and that moving it further forward would not provide an aesthetic benefit.
– Similarly, I don’t have a problem with the width of my jaw and feel that increasing it would change my face more than I would like.
– The main goal is, I believe, to moderately increase the height of the chin and the entire jawline. I originally considered a genioplasty to augment ching height but discarded it for two reasons. The first one is that I’ve been told that it leaves a step in the jawline which can be visible and certainly felt. The second is that it would give the appearance of a longer/narrower face, which is something I would not like.
– My conclusion so far is that I seem to be seeking a result along the lines of what could be achieved with a chin wing procedure that only adds height, without any forward movement. Would you agree with this, based on the previous comments? Is this something that Dr Eppley performs, or is it something that can be replicated through customized implants?
Again, thank you very much for your help, and hope to hear your thoughts.
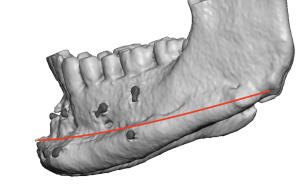 A: I think we both agree that vertical jawline lengthening is the correct aesthetic goal to which there are 3 ways to try and achieve it with varying effects along the length of the jawline:
A: I think we both agree that vertical jawline lengthening is the correct aesthetic goal to which there are 3 ways to try and achieve it with varying effects along the length of the jawline:
Vertical Bony Chin Lengthening – affects chin area only (a 1/3 jawline augmentation procedure)
Chin Wing Osteotomy – affects chin and body of mandible (a 2/3s jawline augmentation procedure)
Custom Jawline Implant – affects the total jawline from chin to jaw angles.
With that understanding the chin wing is a good procedure as long as you understand it will have no lengthening effect on the jaw angles. Once you understand where the osteotomy line is (see attached) it becomes clear it provides no improvement at the jaw angles and its effect fades as one moves back from the chin. In essence it is a 1/2 or 2/3s jaw lengthening procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon