Your Questions
Your Questions
Q: Dr. Eppley, How do you think a ligated temporal artery turns into connective tissue? For example, if after a few years the nodules unravel, will blood flow through them again?”
A: Once blood flow is cut off by the sutures the blood flow is stopped and does not return even if the sutures dissolve as the internal lumen of the vessels is now clotted and fibrosed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Will my lip swelling on the right side subside in time or is this a permanent complication at 8 months post op? I had v line surgery with aggressive contouring on the right side, and a genioplasty to shorten length of my chin 8 months ago. I still feel the swelling in lips, on the right side, with a slight pull to the right and down. Will this swelling improve on its own?
A:It would be fair to say that whatever you see at 8 months postop is probably permanent. This is not swelling at this point.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My nose bridge looks low on the upper side. Can a forehead reduction help give a raised nose bridge appearance?
A:Your nasal bridge is low and our brow bones are protrusive so it is the combination of both that contribute to your concerns. While brow bone-forehead reduction would be beneficial you are never going to do that procedure due to the long scalp scar that would be needed to do so. Thus the only acceptable option is nasal dorsal augmentation (see attached imaging)…which not only addresses the low nasal bridge but also makes the brow bones-forehead look less protrusive.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I had jaw reduction surgery before but they cut too much. Can I have jaw implant surgery to get the old shape?
A:I see lots of overdone and/or V line surgery regrets of which custom jawline implants are the only way to partially of fully reverse the effects of the bone removal surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 39 years old trans woman. I am looking to feminize my upper body. What procedure(s) would you recommend to achieve a feminine upper body? Please get back to me as soon as possible as I am currently planning the next steps in my transition. Thank you ☺️
A:The two most commonly performed procedures for upper body feminization is shoulder reduction and breast augmentation, either done separately or together. (the attached imaging shows the likely shoulder reduction result)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
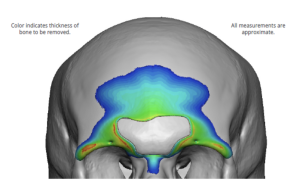
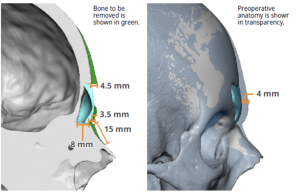
Q: Dr. Eppley, I wanted to know from the dr If there is a cranio facial surgery that can reduce the height of my top scalp? I feel it’s high abit like a cone shape. Thank you!
A:You are referring to skull reduction in which the outer cortex of the skull bone is removed whose result (how much reduction ) is controlled by the safe amount of bone removal permitted.(see attached imaging prediction)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have healed well from my initial shoulder narrowing surgery and am pleased with the change in my shoulder width. I was curious if the clavicles can be cut a 2nd time for even further narrowing?
A: Secondary clavicle reduction is theoretically possible…although I have never yet done it and your request would be the first. The question is not whether you can cut out more bone but whether the shape of the much reduced clavicle bone would support the hardware needed to hold it together while it heals. A preoperative x-ray may provide some insight into that issue.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Hello, back in 2018 i underwent cheek augmentation via cheek implant. i wanted a model look, so i wanted auumentation laterally(so that my midface have the classic hollow look in comparison to my high cheek bones). on the quote it was written zygomatic arch implants. however when i looked into my OP report it said M shaped medpor implants(not mentioning zygoma),size small. on the colnsult we agreed on medium size zygomatic arch, allegedly custom made. however i did get a fat transfer into cheeks a bit priorly to implant surgery, awhile back. and after implant surgery he informed me that he had to go with small implant instead. right off the bat, i was unhappy with results. and 5 years later, i finally have to courage to remove the implants. as i look over the OP report, i wonder how would he just come up with smaller size implants on the table, if zygomatic ones are custom? what are M sized implants, is that different from zygomatic arch implant? could it be something like a regular malar implant?as i suspect placement might be different(over bone or soft tissue?). should i inquire that with the surgeon before removal consult with you? to provide you with the fuller picture?
A: I can not address or will respond to what took place between you and your surgeon both before or during cheek implant surgery…..I was not there. My only general comments would be:
1) As I perceive and do zygomatic arch augmentation with implants, there are no standard implants to achieve that effect. They must be custom made to extend back along the entire zygomatic arch. Standard cheek implants are not zygomatic arch implants
2) Contemporary custom facial implants are made from the patient’s 3D CT scan.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had some questions about a procedure involving the epicanthic fold area. My eyes are a bit close together mostly because of the exposure of my tear ducts. I had been looking around at possible procedures to increase the distance between my eyes, and found a few studies in which reconstruction of an epicanthic fold was done. I was interested in seeing if you would be able to offer something like this. I don’t really have an epicanthic fold, and don’t really desire one, but I would like something similar to increase the distance between my eyes. I’ve attached photos of my eyes & the edited result I desire. Again, I would not really like the “fold” that many asians typically have, but perhaps just more skin covering the tear duct. Thank you for your time!
A: What your edited image shows is a change in the angulation of the inner corner of the eyes, a more downward location of the corner which may slightly increase the distance between your eyes and create the appearance of more skin covering the lacrimal lake area. Since you don’t have an epicanthal fold This is most effectively done with a tissue rearrangement technique as shown in the attached diagram.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope this message finds you well. I have been extensively researching jaw implants for over a year. Your expertise and reputation in the field have greatly impressed me, and I am planning to schedule an appointment at your office very soon. I am seeking your professional advice on a few concerns regarding jaw implants, particularly considering my age and current circumstances.
Age and Jaw Growth Concerns:
I recently turned 20, and my orthodontist confirmed that my jaw has stopped growing since 2020. However, there is a possibility of continued growth until I am 25.
Given this, am I too young to receive a jaw implant? What risks are associated with getting the procedure at my age?
Is there a way to determine definitively if my jaw has completely stopped growing, ensuring a successful and complication-free implant procedure?
Concerns About Fillers:
I have a strong preference for a permanent solution over fillers, such as Radiesse and Volux, which I find temporary and unsatisfactory.
Despite this, I have been recommended fillers due to my age. Considering my financial readiness do you think it is worth waiting until I am 25 for a jaw implant, or is it feasible to consider an implant now?
I have attached front and side profile pictures, as well as front and side x-rays of my skull, to provide a comprehensive view of my current jaw structure. I hope these images will assist you in giving me the most accurate and tailored advice possible.
A: In answer to your questions:
1) Whatever mandibular growth occurs after age 18 is minimal and in the sagittal direction, thus making that a non-consideration for any type of jaw implant.
2) The risks of any facial implant procedure is age irrelevant.
3) There is no such thing as a risk-free surgical procedure particularly when it involves an implant.
4) Your jaw deficiency is primarily vertical (height) in its dimensional needs. This is evidenced by the adequate projecting chin but deep labiomental fold, bunched up chin pad tissues and vertically short chin combined with a flat mandibular plane angle behind it. The correct augmentation approach is a vertical lengthening bony genioplasty (6 to 8mms) with custom jawline implants behind it. (see attached imaging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Perusing through your website I realized that there is a section where people ask you questions and your answer them back,since I could find where I could submit you questions I would like to ask you here if you don’t mind!
I would love an advice from a world leading expert like yourself in jaw angle implants,i live in Brazil and here the only material used in this procedure is the off the shelf medpor implant but I found an oral and maxillofacial professional who does custom PMMA jaw angle implants,since information about this procedure done with PMMA implants is very scarce and almost non existent I would like to make you some questions before proceeding with said professional:
A – From what I gathered,PMMA has a higher chance of infection than silicone,but how much higher is this risk exactly?I read that silicone jaw angle implants have a 4% to 6% chance of infection,how much it is for PMMA?
B – MEDPOR is more difficult to remove due to tissue in growth,does PMMA has the same issue?
C – Is PMMA implants visible on CT scan for future removal or replacement?
D – Does PMMA offer any advantage at all compared to other materials available on the market?As I said,I live in Brazil and,unfortunately,due to geographical and financial reasons I could only afford to do this procedure here with the off the shelf MEDPOR or with customized PMMA implants
Sorry if this seems too lenghty,I just think it is vital to ask all of this to the most experienced professional out there in this procedure,I would be kindly thankful to you if you could help me navigate through this all!
A:In answer to your questions:
1) PMMA has a higher infectivity rate than silicone in the face but how much higher is not precisely known.
2) PMMA is non-porous, unlike Medpor, thus its tissue attachments are less. But it is still not an easy material to remove because it is so hard.
3) PMMA implants would not be visible on a 3D CT scan.
4) I see no advantages to PMMA material over Medpor other then the ‘customizable’ part but I really don’t know what that means. The term custom can have various interpretations.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I have a few questions for Dr. Eppley. I came across this youtube video showing a type III forehead reduction being performed, and it highlighted the challenges with dealing with the frontal sinus. Could you ask how you will handle it? Does the surgical facility have a live CT and planning software similar to what was used in the youtube video above?
Finally, I attached some pictures I took when Dr. Eppley marked where he thought he could shave down to without doing a Type III flapback procedure. I now realize CT images are reviewed to see how much bone is available for shaving – is this limited by the frontal sinus? If so, after reviewing the CT footage, does he think those markings are still accurate?
A: In answer to your brow bone reduction questions:
1) I am not sure what is meant by the ‘challenges’ of an open Type 3 brow bone flap setback procedure. Brow bone surgery essentially its frontal sinus surgery.
 2) In today’s world as much of FFS is done through insurance new technologies have been developed using the patient’s 3D CT scan to help ‘guide’ the surgery. To those of us who are very experienced in this surgery we feel this is not worth the added expense. ($5,000 +) But if insurance is paying for the costs of such technology then why not get it. It is very cool technology and it is done from the same engineers from which all of my custom implants are made, so I am very familiar with it. But in the aesthetic patient who is paying out of pocket one has to put a value on what it brings to the surgery. (i.e,, does it make for a better outcome)
2) In today’s world as much of FFS is done through insurance new technologies have been developed using the patient’s 3D CT scan to help ‘guide’ the surgery. To those of us who are very experienced in this surgery we feel this is not worth the added expense. ($5,000 +) But if insurance is paying for the costs of such technology then why not get it. It is very cool technology and it is done from the same engineers from which all of my custom implants are made, so I am very familiar with it. But in the aesthetic patient who is paying out of pocket one has to put a value on what it brings to the surgery. (i.e,, does it make for a better outcome)
3) I have your 3D CT scan from your previous surgery so the brow bone reduction prediction by imaging has an anatomic basis for it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I previously had rhinoplasty 15 years ago with another surgeon who had made my nostrils smaller at the area where the nostrils meet the cheeks. As a result, the nostrils are now too rounded off. I would like for the nostrils to restored as close as possible to what it was originally. I believe the procedure would involve some skin/tissue grafting. Before booking a consultation, I would first please like to know if the doctor performs such a procedure and whether it would lead to unsightly, significant scarring?
A: It is ‘easy’ to make the nostrils more narrow as defined by the usual good scarring as a result of the tissue excision. The converse of nostril widening, however, is a different story. As you have correctly surmised it requires the addition of a graft (chondrocutaneous graft from the ears) to replace what has been removed after the nostrils are released from the cheeks. Such interpositional graft replacements, while increasing nostril width, will have a different skin color from that of the nose and cheeks since it comes from the ear. Thus it will be visible and will not look exactly as it did before even though nostril width may be restored. Such nostril base grafting is really a reconstructive procedure and not an aesthetic one. (unlike nostril narrowing) Thus I would be cautious when considering this procedure for aesthetic restorative reasons.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve already submitted a form in order to schedule a consultation with you for removal of medpor implants with you.
The question I have is how sufficient do you find the passage from the OP report that I’ve submitted here in order to assess what implants we are dealing with ? To my knowledge, I don’t see in this report 1) where he placed the implants over bone or soft tissue (could you guess that merely from where the incision was made?) 2) where exactly they have been placed. I do not understand why the Op report says “M shaped implants” (when we agreed on zygoma implants), what do these numbers stand for? I understand you were not a part of this procedure, but I would like to provide you with the most accurate picture.
As I’ve learned from your forum there is a different level of difficulty for procedure, depending on positioning of the implants? Better yet, would you like me to get any of the images prior to the consultation? So, that you provide your opinion and accurate quote?
Please advise me, what additional information I might need to inquire from my previous surgeon or if I need to complete an MRI/or a 3D scan (your forum mentions that sometimes implants are not visible on a 3D scan).
A:In answer to your questions:
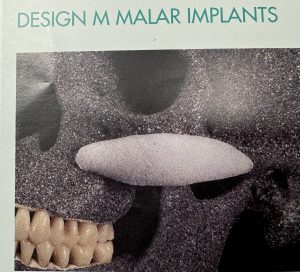 1) The operative report state these are the M style Medpor cheek implants which, when you look at their shape, are an ‘arch’ style cheek implant. In other words these are the closest to a zygomatic arch implant as standard implants can be. (see attached picture)
1) The operative report state these are the M style Medpor cheek implants which, when you look at their shape, are an ‘arch’ style cheek implant. In other words these are the closest to a zygomatic arch implant as standard implants can be. (see attached picture)
2) I would have no doubt these implants are placed at the bone level under the soft tissues.
3) As you have noted Medpor implants are rarely visible on a 3D CT scan. (occasionally that can be seen in some patients)
4) You get a 3D CT scan IF the primary goal is to replace the existing cheek implants with custom designs. The scan is not necessary for removal alone as noted in #3 above.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Thank you for your prompt reply.You mean there is no way at all for shoulder narrowing to narrow the shoulders while at the same time avoid making the shoulders lower and more downwardly sloped? Even adjusting a different part of the clavicle bone won’t help? Of course, I’m all for shortening it but it would be nicer if I could have it shortened whilst maintaining its height, even if it meant more surgery. I’d really love to have it with you but the shoulders looking lower is a major concern of mine.
A: I refer you back to my original response. The vector of movement does not change regardless of where you are on the clavicle bone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is there a way to keep the shoulders at a normal height after shoulder narrowing surgery? I want the surgery but not if it makes my shoulders look lower and more sloped downwards. I want them to remain at the height they are at now but shortening the clavicle bone will make them look shorter and I want to avoid this. Thank you.
A: Wbat you are asking is the antithesis of how shoulder narrowing surgery works based on the natural shape and posirion of the clavicle bone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am wondering if Dr Eppley can do two procedures at the same time. I was going to have revision rhinoplasty with the other doctor late this June but I though it may be better to do them at the same time with Dr Eppley.
Background – I had cartilage taken out from my ribs for nose tip. However, the cartilage is protruding a little bit on the septum especially when I smile or laugh. I’ve attached the pictures. It’s right below the tip. I’ve had this since 2019. The other doctor, who originally did it, has recommended to redo it to reposition the cartilage.
A: Sure. Provided the rest of the shape of the tip of the nose is fine, which I think it is as that end of the cartilage is away from the point of tip projection, then the end needs to be trimmed off through a small lateral columellar incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I would like to know if there is a way of fixing high-set supraorbital rims, without using implants? I was wondering if HA Paste could be an alternative to lower them?
A: Implants are the only effective approach to lowering the shape of the high set supraorbital rims. HA paste would be the least efective method to do it as a soft material when mixed that has to set it has no ability to push the tight brow tissues lower in the set process. It requires a firm material in its crystallinization process.
Although to be completely accurate HA paste might be effective for this purpose IF a full coronal scalp incision was used for access and as well as a full release of the brow soft tissues. But the scalp scar in doing so may not be an acceptable asthetic tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to have the horizontal edges of my lips expanded, aka a commissuroplasty. I have a hard time opening my mouth wide when eating, at the dentist, and smiling.
A: I would agree that the corner to corner width of your mouth is small as it is barely wider than the width of your lateral nostrils. (bialar distance) Mouth widening surgery can make its appearance wider but I have some concerns about whether it would really improve mouth opening as the widening process creates some scar tissue at the mouth corners. A wider looking mouth does not always translate into one that opens more easily or wider.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to restore the ear tragus?
A: An essential part of restoring a lost tragus is that skin is needed to cover the cartilage graft that provides the foundation of the tragus reconstruction. I can see the scar tissue that crosses over the tragus site which undoubtably is the result of the mechanism that caused the lost tragus. Such scar tissue is not good coverage for tragus cartilage graft so the chance of a successful result is very low.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want a more defined chin using an implant instead of genioplasty, and not sure if the Terino square chin is right for me, and wanted to consult with you. Thank you.
A: I assume the preference for an implant over a genioplasty is that you desire a more square chin shape over your current rounder more tapered chin shape. In that regard you are correct as only an implant can make the chin less round/wider/more square shaped. Of all the available standard chin implants only the Terino style has a wider less round shape. While a custom chin implant design provides the best control over all aspects of a chin implant’s shape if you had to use a standard implant the Terino would be your only choice.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, is a CT scan/3D CT beneficial to have done prior to a consultation for custom facial implants. Thank you.
A: The 3D CT scan is the platform on which custom implants are designed but they doi not tell us what to do, only how to do it. So no a 3D CT scan is not required or beneficial for the initial consult.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in an operation to ligate the temporal artery, I can’t find a specialist in this field in my city, maybe you know someone from Russia who does similar operations?
https://exploreplasticsurgery.com/category/temporal-artery-ligation/
What studies should be done before ligating the temporal artery?
The surgeon I visited said that it was impossible to do this and directed me to do a CT scan. You write that an ultrasound is enough, which is very good, this is great news.
Does this procedure have any side effects? Could such a procedure cause high blood pressure, stroke, blindness, or baldness?
Is it possible to ligate the artery on both sides of the head?
Can I do football or bodybuilding after this?
A:In answer to your temporal artery ligation questions:
1) I know of no one in Russia or most of the rest of the world that does temporal artery ligations.
2) There are no preoperative studies needed for this procedure. (Ct scan and ultrasound provide useful information, it is a superficial artery you can see where it is)
3) There are no known adverse side effects from the procedure that have ever been seen nor would they be expected.
4) Doing the procedure on both sides of the head is common.
5) There are no physical restrictions after the surgery once one is fully healed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a wider shoulder frame & am planning on shortening them. I want to shorten both clavicles by 3cm each.Thank you!
A: 2.5cms clavicle shortening per side is the usual amount. Unless you are extremely tall (greater than 6′ 2″) the length of the clavicle and the hardware that must be applied may not permit a 3cm reduction per side. This is a technical limitation which is the result of the reverse S- curves at the inner and outer third of the clavicle.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’d like to inquire about skull implants. Flat back.I have a few questions..
1. Does the implant move around or stay in place?
2. Does it eventually have to be replaced?
3. Is there a massive headache afterwards?
4. How long does this procedure typically take?
Thank you, kindly !
A:In answer to your skull implant questions:
1) Skull implants do not move around or change position once placed.
2) Skull implants are structurally stable and do not degrade or break down, thus they never need to be replaced due to material failure.
3) Patients do not typically complain of significant head pain by the morning after surgery.
4) The operation for custom skull implant placemen takes 90 minutes to complete.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I suffer from a deep bite and the lower third of my face is smaller than the rest ( small face syndrome) so I would like get a proper symmetry by jaw augmentation if that would work?
A:The first important question with a deep bite is whether you should treat the primary problem with jaw repositioning surgery (double jaw surgery) or to camouflage the problem with implants and/or a bony genioplasty. Do you have any thoughts on that potential decision?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have measured that my mid face ratios and facial height to width ratio are close to ideal. I am interested in changing the features themselves and the bone structure to create a more harmonic, masculine appearance. For now, I want to focus on the bone structure. I would like to fix asymmetry and get a sharper, more angular bone structure with wide, prominent zygomatic and cheek bones. The last picture is a very crude morph of the bottom middle one, approximating an ideal result with jaw and cheek implants and several other surgeries. Based on the images and additional information, does it look like I would be a good candidate for angular-looking implants, particularly cheek and zygomatic? Or would my skin be too thick to get a sharp result, resulting in a bloated appearance?
Additional information:
– I will likely have double jaw surgery. In the pictures, my jaw is jutted forward to hide recession and simulate a possible result as a base for implants. I believe my maxilla is recessed.
– My skin is dry on my cheeks but oily on my forehead, and I rarely get cuts from shaving, if that helps indicate skin thickness.
– I often see my cheekbones in artificial lighting but not really in natural lighting. My body fat percentage is 10%.
A:I believe the fundamental question is whether IOM (infraorbital-malar) implants will create a sharper more angular midface/cheek appearance in your face? I don’t think your soft tissues are prohibitive in that regard BUT it would need to be combined with defatting below the IOM level (buccal lipectomies and perioral liposuction) to have a reasonable chance to come close to your own image changes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got iliac crest implants in Korea along with small hips implants. I now have some dents under the implants. Is there a way to solve this using silicone implants? Perhaps longer implants or change in implant contour? Or implant positioning?
A Hip augmentation is challenging in that it is really a vertically long area and is actually comprised of three zones, Zone 1 = iliac, Zone 2 = trochanteric and Zone 3 = lower hip region. This makes it aesthetically difficult to just augment one single hip area/zone and get a smooth contour from top to bottom. As you have learned augmenting zone 1 with the plate creates a relative deficiency in the lower two zones. Adding the current silicone implant augments zone 2 but can leave a stepoff at that transition point.
This leaves two potential solutions:
1) the current implant needs to have a better taper towards its inferior edge rather than be shaped like a mound in cross-section, or
2) use a longer implant with a taper.
This is actually a common problem in all hip implants. (inferior edging) I would start first with having the current implant with a more distinct taper towards its inferior edge but probably a longer implant is ultimately what is needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had two otoplasty surgeries last year. On the first surgery the surgeon worked only with sutures and there wasn’t a big change. On the second surgery he worked on the conchal bowl and the results were more what I wanted. The issue is my ears still feel stiff and unnatural and it makes me uncomfortable how they don’t bend how they used to. If I remove the sutures and I guess scar tissue will they feel like they used to? My main issue was the conchal bowl so I don’t really mind if the anti helix changes back to how it used to be, just really wanted them to feel more natural.
A:Whether you remove the sutures or not your ears are not ever going back to a completely feel in terms of stiffness…they will always be a bit stiffer than before the otoplasty surgery. There certainly is no harm in opening the ear up and removing sutures and scar. But how much improvement you get in the feel of them is unpredictable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am considering rib removal surgery, of the floating ribs, and also shaving of the ribs, rib removal of rib #9-10 the ribs that are attached. Or I’d like to do everything I can to have my waist line slimed as small as possible. I read something about doing something to the lat muscle, I do have wide Lats cause I’m into pole fitness. I have always had a more athletic figure broad shoulders and I’ve always wanted a hour glass figure shape. I had a BBL maybe over a year ago and it left some lumps in my stomach, even though I did the massages. I think what happened is they tried to take to much fat out of my lower abdomen below my belly button, and they didn’t take ANY fat out of my upper abdomen below my boobs. I didn’t have enough fat on my lower abdomen so it caused ripples which destroyed my tummy. Because they tried to take a liter of fat out of only my Lowe abs and there just wasn’t enough there. I use to love how my stomach looked and how I hate it & have to cover it all the time! and there is a lump above my belly button since they didn’t take ANY fat out of there. I cried when I looked at the before and after pics of my tummy, I feel like I spent so much money to look worse! Then I did before. My belly button looks gross now. My butt barely looks bigger at all, and if I could choose I’d rather not have a lumpy tummy. Is there anyway you can correct that? Or do some sorta body sculpting on my abs so it looks half way normal, I’ve had to wear a garter set, or only high waisted pants to cover my tummy since the BBL, and it’s effected my work. Cause I can’t wear a low bikini. It looks like cellulite on my stomach. Does the doctor do webcam consultations or in person consultations? Because I’d really like to speak to the doctor himself to see what his opinions are about what is possible in my case. And then get a estimate of costs so I can start saving up, and see what kind of financing options are available to me. And I’d also like a BBL while we are in there since we are going to be removing the ribs and sucking out all the fat in my midsection.
A:Thank you for your inquiry and sending all of your pictures. Unfortunately you show all the effects of being a poor candidate for BBL surgery. The abdominal irregularities are the direct result of trying to take fat from someone who simply didn’t have it to give. Thus the thin smooth subcutaneous fat barrier between the skin and the abdominal wall has been disrupted and can never be restored. Trying to do further liposuction to try and smooth it out will only make it worse. The only potential liposuction benefit is in the upper umbilical area where there is some residual fat thickness so at least that could be made less raised.
The conclusion is that, while liposuction always has the risk of postoperative irregularities, that risk is magnified when the abdominal fat layer is thin and then an aggressive approach is used for the fat removal. This is largely irreversible and don’t waste a lot of money chasing treatments and surgeries that are not going to really fix it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon