Your Questions
Your Questions
Q: Dr. Eppley ,10mm chin implant removal and replaced with a 8mm sliding genioplasty… 8 weeks ago. Having discomfort in area under the lip which I try ought was just the scar healing but it seems to be a bit lower than the scar and only on the left side. It is so sensitive that it makes it feel like the whole chin is restricted when I open my mouth to talk. It feels like something needs to be cut to release this tension….
The area you can see where my finger nail covers is very tender and hard/firm to the touch and when I open my mouth and speak/ talk it feels like something is going to rip because it’s all so tight. I really don’t know what it could be. It’s very small area like I can pinch it with two finger tips and get the whole left side of my mouth feels strange. The right side is fine.
A: It certainly sounds like a release is needed with a small fat graft for this spot area of tightness after a sliding genioplasty.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,, I underwent bimaxillary surgery which in my opinion was unsuccessful and after removing the titanium plates I found myself with holes in the central part of my face… I removed the maxillary plates because they gave me a strange appearance but now I find myself worse than before… I see my midface as completely empty, ugly and aged… i ve been thinking to have silicon midface implants but don’t know which specifically…which u suggest in my case.
A:To augment/fill in the maxillary defects you have two basic options:
1) Bone graft the maxillary defects using either allogeneic bone blocks and chips. (you could harvest your own bone but that is probably not too appealing
2) Fill in the defects with hydroxyapatite bone paste/cement
3) Make custom implants to do the contouring.
I would lean towards options 1 or 2 because it is likely there may be bone defects exposing the maxillary sinus cavity of which implants may not do well in that circumstance.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, is there a way to correct nasolabial folds caused by my deep canine fossa ideally something more permanent and not filler. Thanks for your time, have a nice day.
A:Nasolabial folds are largely created soft tissue ptosis. In the upper part of a nasolabial fold near the nose (and over the canine fossa) bone augmentation by an extended paranasal implant can help soften this part of the fold…but I would not call it a complete correction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible for a head to be too big for reshaping?
A:I think the question you are really asking is whether a skull reduction at certain head sizes would not be particularly effective. (aka nit make much of a difference) Abd that answer would be yes that is possible. Which is why I always try to image what the changes would be using the patient’s pictures before surgery to help them make the decision about the merits of the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,I was wondering if the skull augmentation procedure that will be done will also change my hairline. I was hoping that it would by default as the whole skull would be widened but I wasn’t sure. My hairline is quite feminine due to my narrow skull. I used to shave my hairline to make it more masculine. Anyways I was just wondering if it would aid in that or if I should worry about that after the surgery.
A: In standard skull augmentations the hairline is not changed. In larger two stage skull augmentations it probably will change it a bit in the favorable manner to which you refer…but not drastically.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I read the piece by Dr Barry Eppley concerning removal of a pulsatile facial artery near the mouth. I have had this for about 15 years following an injection of facial filler into the area. It is always visible and it would be a real blessing to me if it could be removed. Please could you get in touch concerning this procedure.
A:Probably developed an aneurysm of the facial artery before it bifurcates near the corner of the mouth. I presume this was from filler injections for the nasolabial folds.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, ( have been interested in getting shoulder reduction surgery for the longest time and want to learn more its recovery.
A:Recovery from shoulder surgery is mainly the restriction in arm motion that is needed. In the first 2 weeks after the surgery I have patients keep their elbows close to their sides as much as possible. In essence you will be short arming with free use of forearms and hands. In the next 2 weeks the elbows can go out to 45 degrees, the following two weeks 90 degrees and thereafter one can have complete range of motion of their arms. More physical activities like sports etc one would be wise to wait to 10 to m12 weeks after the surgery. Thus recovery is not so much about pain but about the short term arm motion limitations. Such a unique recovery requires some forethought into the immediate postoperative management right after the surgery and how quickly you can return home.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley I have under eye hollows. Can they be improved with laser c02 treatments and plasma under eye injections? Because I had that done recently, no change as of yet.
A:Those are procedures that you have as a first step to see what can be achieved non-surgically for your undereye hollows. You hope that they are effective but, if not, then one proceeds to a surgical approach. (infraorbital implants) In essence you need to ‘prove’ that surgery is needed and would be the only effective treatment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
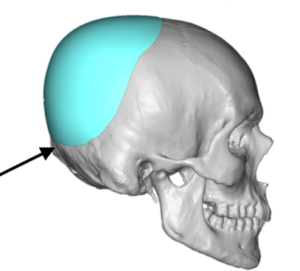
Q: Dr. Eppley, I want to get skull reduction surgery. When I was a child and teenager growing up I was bullied relentlessly for my head being big. The back of my head is so big that everyone says that it looks like a peanut. I think it might be a deformities or something. But I want to get skull surgery so that it doesn’t look like a peanut. I just want the round of my back head to be straight.
A:You have a large occipital bun skull protrusion which can be reduced with an estimated result as shown in the attached pictures. X- rays would be needed to determine the thickness of the bone but in every occipital bun deformity I have seen it is because the bone is thicker not thinner.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Emailing in regards to your shoulder reduction surgery. I’ve been looking extensively into this for the past 3 years and I’ve been hesitating whether to proceed with it due to the lengthy nature of recovery and the overall benefits of how much can be removed. It’s a big factor for me as unfortunately I have very wide shoulders and scapulas. (I was wondering if the scapula can be slightly shortened or manipulated too), I’ve seen that you can remove around 2-3cm on each side (more towards the inch measurement on each side), I am desperate for this but I want to know that I can remain functionality and still be able to move them effectively and that the screws won’t release if I happen to move my arm in a different position by accident? In regards to my height I am 6ft but my shoulder span is very broad. Hopefully you can help me with my queries.
A:In answer to your shoulder reduction questions:
1) At 6′ tall you can remove at least 2.5cms per side, maybe 2.75cms per side. That always makes for a very visible difference as can be seen in the many before and after pictuers of the surgery on one of my websites. (www.eppleyplasticsurgery.com….go to the Shoulder Reshaping page) By looking at other patients you can get a feel for the type of shoulder shape change that occurs. It will also be important to do some imaging of your shoulder pictures as well to see what type of change is realistically possible.
2) In regards to the scapula there are more limited changes that can be there. A prominent spine/ridge can be reduced but you can’t change the width of the scapula…which is usually what is the aesthetically disturbing feature of it.
3) Of the hundreds of shoulder reductions I have done no patient has experienced postoperative range of motion limitations.
4) The main risk of the surgery is early hardware loosening and non-union…which is why I apply both a superior and anterior plate. No one to date has suffered screw pullout or plate displacement in the early healing phase.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can gynecomastia surgery be combined with chest implants as I think I need both.
A: Thank you for sending your pictures. In your case you could do gynecomastia reduction surgery with pectoral implants and the reality is you really can’t have one by itself with a satisfactory aesthetic result. Your chest lacks volume and has sagging so dual need is present. With teh use of implants y9ur gynecomastia reduction needs (based on pictures alone obviously) would be liposuction with a superior crescent nipple lift. I can not tell at a distance if there is a distinct mass underneath the nipple or not. If there is then this would also require its excision as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have Mild plagiochephaly. I’m looking to see what my options are about contouring my orbital rims possible reducing one side and planting and contouring the other , also maybe options about the asymmetry in the forehead to address the protruding side and the flat side
A: The effects of plagiocephaly in the forehead can be treated by reduction of the more prominent side, augmentation of the less projected side or a combination of both. While ultimately the patient must decide of the three approaches is the most aesthetic change, the other important issue to consider is surgical access. (length and location of the incision) Any bone reduction requires a much larger incision to perform. A custom left forehead-brow bone implant can be placed through a much smaller incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to ask you if it is possible to use a Funnel for inserting wrap around chin implant through submental incision to reduce the risk of infection and if so do you believe Supore od Medpore (I believe this is the same) material can be utilized? Some doctors (such as Dr. Ramirez) do this, and what is your view on it? The rate of infection with submental approach and keller funell should be close to none so no removal would be presumably required and probably (I assume) recovery is quicker?
A: The funnel insertion device has its merits in body implants but is of little value in facial implants. The device is made to change an implant’s shape so that it can pass through a much smaller opening than the natural width of the implant. That has great value in round, semiround and oblong ultrasoft body implants who need such deformation to get through a small entrance incision. But facial implants are comparatively smaller, are more rigid, and their shape can easily be changed to fit through a small emtrance incision. The most rigid materials (e.g.,Medpor, PEEK) rely on a segmentalized implant design to bypass a change in shape that they do not permit. Such rigid mat
While a silicone jawline implant can be introduced through a submental incision it still requires intraoral incisions to be pulled through and positioned. This is the most likely source of contamination and a funnel device will not help in that regard. Medpor and PEEK segmentalized jawline implants require the same three incisions with identical intraoral exposure.
While implant placement techniques can drive down the risk of infection to low levels there is no zero risk of infection no matter what techniques are used.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,. I am 23 and have questions regarding my jaw, more specifically the lower jaw/chin. My chin, or at least the part of my jaw below my lower lip, is very long. From a side profile, it also seems to have plenty of downward growth, compared to a more desirable forward angle. I was wondering if my aesthetics could be largely improved through some sort of chin reduction, or if the correct procedure would be something like a full jaw surgery.
Basically, not only do I want the vertical length of my chin to be shortened, but I also want that to be reflected in a sideway angle, so that my jawline looks more forward projected. I attached a photo of a close friend that I would say have an “ideal” lower jaw, although I am of course no expert in aesthetics. The rest of the attached images is me, and I would like your opinion on what seems reasonable and possible results I could expect. If nothing can be done in my case I understand that as well.
A: In the vertically long but horizontally short chin, an intraoral vertical reduction bony genioplasty is needed. In this surgery (see attached) a vertical edge of bone is removed and the lower chin bone is moved forward and upward into a new more forward and vertically shorter position. It may never be as vertically short as that of your friend’s chin but it will be significantly better.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have extremely hollow cheek and huge hollows under the eyes. In the past, I got filler but that is very temporary. I want to go Cheek/under eye implant. I am also a runner so would these implant be ok if I keep running. Also I have big bumpy nose and can’t breath freely, want to go through from Septorhinoplasty. Can I club both the treatments ? IF so then how much would it cost approximately ? I know it varies from patient to patient but just want to know the estimation to make my mind. I am 40 years old male, East Indian. Thank you very much for taking time to answer my query. Can I get surgery in September? Thank you.
A:You are specifically referring to custom infraorbital-malar-submalar (IOM) implants whose position will be unaffected by any form of physical activity. A septorhinoplasty can be done at the same time.
As the custom implants take several months to go through the design and manufacturing process to get them ready for surgery a September surgery would not be possible.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hallo , my question or my problem is that I have really a very thin wrists (14 inches) each one of them and I am in my twenties. I wear all the time long arm T-shirts that my wrists are not showing. I am really insecure about them. So is there maybe a chance or way that I can increase my wrists.
A:Unlike the forearms the wrists pose some limitations for augmentation as they join with the the hand at a flexible joint area. As a result an implant can not cross the wrist crease and any augmentation must stop at this point. (see attached image) So the wrists can be augmented but it depends on how one defines the location of the needed augmented area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve seen a lot of videos and posts about jaw implant revision surgeries you have done. If I were to downsize my implants (assuming same style), how would you compare the swelling with getting brand new implants. Would it be just as bad or less since the body’s had implants there for over 6 months?
A:The postoperative swelling from revising/removing/replacing existing jaw angle implants, compared to the initial implantation surgery, depends on the material of the implant. If it is silicone or PEEK it would be less. If it is Medpor or PEKK it will be the same or maybe even worse. It is more about the soft tissue attachments than it is about an existing pocket.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a flat head at the back (occiput), all the way down. I have attached a picture of a woman with a similar head shape to mine (but my head is also flat at the top). I was wondering if it’s possible to put implants at the lower part of the back of the head, and lower sides of the head, besides the rest of the back of the head and the top of the head aswell (I would like to do a large skull augmentation).
I have attached pictures where I have circled the areas that are flat on lower part of the head specifically. Is this possible, or do you for example have to take the protruding bone, neck and Temporalis muscles into consideration?
I was also wondering approximately how much a l arge skull augmentation (the whole back of the head, and the top of the head) would cost?
I would be grateful if you had time to answer. Thanks in advance, and have a great day!
 A:While implant augmentation of the back of the head is very common in my practice the inferior extent that can be augmented is at the nuchal ridge line. This is where all the neck muscle attach which can not be released. (see attachedmimage) So as you have correctly surmised the nack muscles (not the temporalis muscle) must be taken into consideration.
A:While implant augmentation of the back of the head is very common in my practice the inferior extent that can be augmented is at the nuchal ridge line. This is where all the neck muscle attach which can not be released. (see attachedmimage) So as you have correctly surmised the nack muscles (not the temporalis muscle) must be taken into consideration.
The term ‘large skull augmentation’ can mean two different things…..the extent of the skull surface area coverage or the actual size/thickness of the augmentation. But as a general rule when a patient uses that term, particularly a female, it does refer to a two stage approach to get adeqauate scalp stretch to accommodate a large skull implant. Computer imaging of pictures help clarify what is actually needed but for now I will assume this is what you would need.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to have a brow ridge or glabella implant placed without using a scalp incision, maybe an upper eyelid incision? Additionally, could hydroxyapatite be an alternative to implants in this area?
A:Custom brow bone implants are usually placed with endoscopic visualization through a very small scalp incision (1.5cms) which may be aided by upper eyelid incisions. Hydroxyapatite cement has many limitations for brow bone augmentation but one of them is that it requires a full coronal scalp incision to place.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have had two previous reconstructive surgeries on my forehead. Originally a feminisation surgery was performed which went poorly, using an unusual technique of essentially recreating the conditions of a frontal sinus fracture and suturing it all back together. Following that surgery I had a revision with another surgeon to try to correct that defect and finish the feminization work using a type 3 approach. Unfortunately whilst the revision went well I still have a depression/defect from the original surgery which seems to be presenting with a loss of volume around the inner eye causing skin laxity and some concern to me long-term. I’m curious what approach you might suggest in addressing this given the proximity to the nerves in this area and my having fairly thin skin. I am fairly recently post surgery so I’m really just trying to understand better at this point.
I have attached some 3d images of the CT scans taken at each stage. Hopefully the issue is clear enough.
A: If the issue is a loss of brow bone contour (indented and not smooth) I would use hydroxyapatite cement to fill it in and smooth it over. This would be the most appropriate contouring material for the frontal sinus area as well as the most assured method of a completely smooth contour with seamless edging. It would only take about 5 grams of material to do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a L shaped malar osteotomy to widen the cheekbones and a chin wing osteotomy for my jawline 4 years ago.Both of these ostectomies have left me with visible bone gaps(depressions) on the bone as per pictures attached. What would be the best way to correct this issue? Would HA paste as a grafting on the bone be the best solution for this issue based on your experience?
A: These defects could be filled in/over with either bone chip paste or hydroxyapatite cement. Since you have undergone an autologous method of facial bone augmentation my assumption is that custom implant overlays would not work for you. (even though they would provide the best contouring method)
In applying three types of putty like biomaterials their application is challenging in tight intraoral applications in terms of obtaining a smooth contour and getting a firm set.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I previously had Zygomatic Sandwich Osteotomies which left my cheeks very irregular. I would like to ask if its possible to use an off the shelf implant and place it over the cheek defects to cover it to act like a cover basically. Or this has to be custom implant? The depth of the defects are around 2mm which is significant in my opinion but my previous surgeon believed that this shouldn’t be visible on the skin surface.
A: You certainly could use an off-the -shelf implant to cover over the defects if you weren’t opposed to an implant. A thin 2mm implant is what you would need to do so.
2mms doesn’t sound like much but in the cheeks that is more than enough to be seen.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have Mild plagiochephaly. I’m looking to see what my options are about contouring my orbital rims possible reducing one side and planting and contouring the other , also maybe options about the asymmetry in the forehead to address the protruding side and the flat side.
A: The effects of plagiocephaly in the forehead can be treated by reduction of the more prominent side, augmentation of the less projected side or a combination of both. While ultimately the patient must decide of the three approaches is the most aesthetic change, the other important issue to consider is surgical access. (length and location of the incision) Any bone reduction requires a much larger incision to perform. A custom left forehead-brow bone implant can be placed through a much smaller incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have been looking into options for decreasing the width of my head. I really don’t want to do surgery now so was looking into non-surgical options. My head is exactly like the pictures attached. The picture attached is a patient of yours that had, “Bilateral head width reduction through excision of bilateral posterior temporal muscles”.
Can this be achieved through injection, nonsurgical? botox?
Thanks and hope to hear from you
A: Such a result can only be achieved by surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to reduce the appearance of maxillary alveolar protrusion with custom implants? Say like paranasal combined with custom cheek implants if someone was trying to avoid jaw surgery to reposition jaws?
A: Theoretically midface augmentation should make the maxillary alveolar protrusion look less so. Computer imaging in profile will provide better insight into that potential effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am looking for information on chin ptosis surgery.I have had a number of chin and jaw surgeries and currently have a sliding genioplasty plus an implant on top. I now have bad lower lip incompetence and chin ptosis. From my understanding, the muscle needs to be resuspended and fixated to the chin bone/implant. I included some scans of my chin as it is right now.
A: Given the chin surgeries you have had I would doubt that ‘simple’ muscle resuspension would be effective at all. You have to be mindful that the two surgeries you have had intraoral sliding genioplasty and presumably an external submental incision for placement of the custom jaw implant have completely stripped off all soft tissue attachments AND expanded the chin tissues. Besides the scarring there is now a relative discrepancy between the expanded structural support and the soft tissues needed to cover it. As a result the soft tissues are not going to elevate in any significant amount and most certainly won’t improve lip incompetence. Ljke most soft tissue retractions this is a tissue deficiency problem and thus tissue rearrangement alone will likely fail.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in shoulder and waistline narrowing? Would it make sense the come back after shoulders are healed to have the hardware removed and the ribs done at the same time?
A: That would make perfect sense and is a very practical way to stage it with hardware removal in mind.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, So do implants made of metal guarantee no infection????
A: No material is better than another at implant infection. The surface characteristics are probably more important than the material as smooth surfaces are less prone to infection than textured/porous/irregular surfaces. (bacteria love to adhere to microscopically rough surfaces)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can the top of my head bene made less tall?
A: How much skull height that can be reduced is controlled by the thickness of the skull bone. But as a usual estimate the maximum bone that can be moved is in the range of 7mms. How that number transfers to your skull height requires imaging of your head pictures to show.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to schedule a consultation. I had a few questions,What is the implant material? Can Titanium be used? I had an orbital fracture when I was young and titanium screws are still in my orbital bone. Is this a problem?
A: For custom facial implants a variety of biomaterials can be used including titanium….but it would by far be the most expensive. Titanium screws in the implantation site are not a contraindication for implants over and around them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon