Your Questions
Your Questions
Q: Dr. Eppley, I have a facial feminization surgery scheduled in the fall. How long would I need to wait after this surgery to be safe to be in the ‘facing down’ position for the rib removal surgery?
A: I would wait a minimum of 3 to 4 months after facial feminization surgery so most of the healing is complete before having one’s face be positioned into a soft cradle for rib removal surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if the hydroxyapatite paste you use in the chin surgeries turns into bone later? Or does it just become hard but not into bone?
A:I don’t use hydroxyapatite paste in chin surgeries since it is a ceramic and never turns into bone. What I use is allogeneic corticocancellous bone chips and blocks which can turn into the patient’s own bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is bilateral temporal reduction risky? Does it have any history of affecting you. How long does the surgery last?
A:Temporal reduction is a perfectly safe surgery that has no adverse effects. Because it is a reductive procedure its effects are permanent.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley I had breast augmentation last year but my right breast is doesn’t look like left one, my right nipple 1 cm lower then left one, I just wondered that can we do crescent breast lifting for my right breast lower nipple. Because I don’t want big scars.
A :It is important to remember that all breast implants do is take one’s natural breasts and make them bigger. Thus asymmetries like yours (horizontal nipple level differences) after breast augmentation are usually what the breasts looked like before the surgery…but often not noticed because the breasts were smaller and the difference between them less as a result. The corrective approach, as you have noted, is a superior areolar crescent lift.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a very weak chin (I think) and was curious what you would recommend as the best course of action?
A:Thank you for your inquiry and sending your pictures. Your chin is weak but not in the traditional horizontal manner. Rather the chin and entire jawline is vertically deficient. This is also associated with a short neck and low hyoid position. There are two approaches to take with your lower face which depends on whether you want just the chin changed or the entire jawline. If it is just the chin then a vertical lengthening bony genioplasty would be the best procedure. If you desire the entire jawline treated then a custom jawline implant would be the procedure. What would separate these two procedures, besides the extent of the jawline treated, is how much vertical lengthening can be achieved at the chin. (the bony genioplasty can do more) These differences are best seen in the frontal view imaging.
Either procedure needs to be combined with neck management (submentoplasty) for the best result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in hip pelvic implants but not the kind that are simply stuffed into a pocket, I’ve been to numerous doctors and the only type of procedure they do are standard hip implants stuffed in a pocket. I have contacted a hospital in Seoul that is known for pelvic plasty but noticed one of your replies on Real Self in response to a similar inquiry. I am very lean and narrow hips and are looking to round out my figure. I am also a trans woman which only adds to my hip deficiencies. I have attached photos for your review. Look forward to hearing back from you! Thanks so much
 A: Thank you for your inquiry and sending your picture. The type of hip augmentation to which you refer is that of iliac crest implants which provides a bony augmentation to the upper hip region rather than a lower soft tissue augmentation over the greater trochanteric region of the hips. This is a procedure known as Pelvic Plasty. Until recently only South Korea offered such pelvic widening implants made of titanium…which is the ideal material for augmenting the bony iliac crest given their side position on the bone and the external forces to which they are exposed. In April 2024 the FDA approved the titanium iliac crest plates used in Pelvic Plasty for clinical use here in the U.S.
A: Thank you for your inquiry and sending your picture. The type of hip augmentation to which you refer is that of iliac crest implants which provides a bony augmentation to the upper hip region rather than a lower soft tissue augmentation over the greater trochanteric region of the hips. This is a procedure known as Pelvic Plasty. Until recently only South Korea offered such pelvic widening implants made of titanium…which is the ideal material for augmenting the bony iliac crest given their side position on the bone and the external forces to which they are exposed. In April 2024 the FDA approved the titanium iliac crest plates used in Pelvic Plasty for clinical use here in the U.S.

 I recently (August 2024) started perf0rming the Pelvic Plasty procedure which has become a composite approach combining titanium iliac crest plates with sub iliac silicone implants that attach (hook into) the under side of the plate.
I recently (August 2024) started perf0rming the Pelvic Plasty procedure which has become a composite approach combining titanium iliac crest plates with sub iliac silicone implants that attach (hook into) the under side of the plate.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have plagiocephaly (flat head syndrome). because of this, my head from front view looks wide and makes it impossible for me to wear caps. I want a little parietal bone reduction on the sides above my ears only… No matter how little it can be trimmed, i will appreciate that. Please i need your help urgently as this is bothering me a lot.
A:Thank you for your inquiry. Parietal bone reductions are done through a small vertical incision over them. The maximum amount of bone thickness is always removed which is in the 5 to 6mm thickness range.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a surgery, dermal graft and testicle implants but it didn’t work. I lost part of the dermal graft because one got infected. Regarding implants… I don’t like them because they’re too small and I can see 4 testicles as I have too much skin. So I would like “the bigger the implants” you can put (7.5 or even 8cm if it was possible) Because I have a lot skin and I would like that new implants to hide my real testicles. In fact, I don’t mind if my scrotum is tight or if my testicles go to up due to new balls. I like that. Don’t worry about that.
A: Thank you for sending your pictures. I would agree that 7.5cms size implant replacements would likely push your natural testicles out of the way and make them less visible. The current implants you have are too small and have done what I would think would have happened…show all 4 of them.
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley,After a few months after my buccal lipectomy I am thinking I want to reinsert fat back into my buccal area. Just not satisfied with the look, my face just looks too skinny. I probably just should’ve went with the buccinator myectomy and perioral mound liposuction initially, can’t change the past and can only move forward. My question is how to reinsert fat back into the Buccal area and how many ccs of fat is needed to fill the area back up properly? Thanks
A: There are two ways to restore buccal fad pad volume which is in the 2cc to 3cc range, fat injections or the insertion of en bloc (solid) fat graft back into the buccal fat pad space. Each method has its advantages and disadvantages. Usually the latter is more effective as it puts the volume directly back into where it was initially removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is sliding genioplasty an option to improve jawline/chin structure? I don’t want to have more major jaw surgery, since I don’t have the ability to take that much downtime off work. Also, I have no bite problems and no sleep issues. If sliding genioplasty is an option, I would be interested to see how much it could potentially help.
Thank you in advance!
A: Thank you for your inquiry and sending your pictures, You are correct in that short of a major lower jaw advancement a sliding genioplasty would be the correct procedure not a chin implant. The chin bone needs to move as far forward as possible, maybe even being a jumping type of genioplasty to maximize the forward movement and avoiding adding any vertical length to the chin. This would have the same aesthetic effect as moving the lower jaw forward with the exception of the position of the lower lip and the depth of the labiomental fold. (which can only be improved by the lower jaw advancement since these are teeth-based positioned structures) I would also do liposuction of the neck to enhance the effect of the chin advancement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I might be interested in the bicep implant. Maybe you can give me some more information on cost and if there are any scars after the surgery.
A: Thank you for your inquiry. There are two approaches to the placement of a bicep implant, on top of the muscle under the fascia (subfascial) or under the muscle on the bone. (submuscular) There are advantages and disadvantages with either implant location. There are also different incision locations between them as the subfascial technique puts the scar high up in the axilla and the submuscular technique puts a small incision in the inner arm area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in having Forehead Augmentation Surgery. I am a transgender woman and I have had my brow bone shaved down. While it improve my appearance, it still did not give me the forehead I am looking for. I want to achieve a more rounded/flat, feminine forehead, right now mine has a slope that is not appealing in a female.
I have read that the most common approaches are bone cement and custom-made implants. I am interested in learning how much this type of surgery would cost (both with bone cement and implants), and how long would I need to stay in the area.
I am attaching four images, one showing my current profile, another one showing what I would like to achieve, and two more images of a CT Scan that I recently had done showing the anterior and lateral side of my head.
Thank you very much for your attention to my inquiry.
A: Thank you for your inquiry and sending your picture. You are correct in that ‘old style’ bone cements and contemporary custom implants are the two most commonly used options for forehead augmentation. There is also a newer standard ePTFE preformed forehead implant. Each has their advantages and disadvantages which ultimately comes down to what incisional access is needed to place them, how far back along the upper forehead and to the sides of the forehead does the augmentation need to cover, how precisely can each method achieve the aesthetic forehead goals in a smooth and even fashion and their costs to perform them.
Because of your prior surgery you undoubtably have a long frontal hairline or more posterior scalp scar for access so the incisional differences between the forehead augmentation methods is irrelevant. If you throw out costs the custom forehead implant is always the best choice because you control every dimension of the implant prior to its placement so achieving the final goal in a smooth manner with no edging is the most assured. Bone cements are also a good option for you because you need to be able to turn down the forehead flap so an open visual field exists to apply, shape and let the cement cure. This requires the long incision which again I assume you have. There are two different types of bone cements, PMMA (plastic) and HA. (hydroxyapatite) HA is the best bone cement to use because it is composed of inorganic calcium phosphate crystals which is the most similar to bone…but it has a significant cost factor to it. PMMA is the most economic bone cement option. Off-the-shelf PTFE (Goretex) forehead implants are used primarily for the Asian female who wants a rounder forehead and limited incisional access to do so. But they are more a central forehead augmentation method.
If you look carefully at your own side view imaging prediction notice that the frontal hairline remains the same indicating that the augmentation shown is more of a central augmentation effect that only needs to feather out as it approaches the hairline. (and probably the bony temporal lines as well to the sides) Given your more central forehead augmentation goals (which are probably in the 5 to 7mm increase at most) and keeping an eye on costs, bone cements vs a preformed ePTFE forehead implant are good choices for you.
As for logistics you would fly in the afternoon/evening before surgery, have surgery the next day and then fly home the following day.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am very unhappy with how long/big my head is. I am wanting to inquire about a skull reduction procedure, and specifically reducing the size of the back of my head; seeing if what I would like done is even an option.
Thank you for your time.
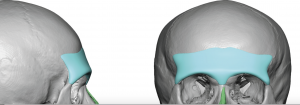
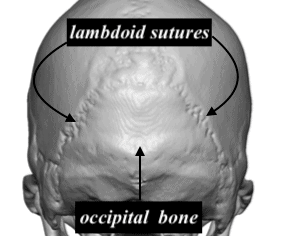 A: Thank you for your inquiry and sending your picture. You have a classic occipital bone protrusion whose border is the lambdoid sutures. This is where the occipital bone grows outward out of proportion to the adjacent parietal and temporal bones, hence the protrusion. The occipital bone can be reduced and brought back into alignment with the surrounding skull as the per attached illustration.
A: Thank you for your inquiry and sending your picture. You have a classic occipital bone protrusion whose border is the lambdoid sutures. This is where the occipital bone grows outward out of proportion to the adjacent parietal and temporal bones, hence the protrusion. The occipital bone can be reduced and brought back into alignment with the surrounding skull as the per attached illustration.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am writing to you as an expert in male facelifts that are bald. I am interested in knowing if I am a good candidate for the surgery. (pictures attached)


 A: Thank you for sending your pictures. I am not certain what qualifiers one as a ‘bald male facelift expert’ but I have certainly done a few such patients. The basic maneuvers of a facelift remain the same but with the caveats of some alterations of incisional placement around the ears. It is important that the anterior ear incision not go above the helical root and descends to the earlobe in a retrotragal fashion and that the posterior ear incision and backcut not go beyond the shadow of the outer helical rim. The submental incision for the central neck work remains the same as in any other patient. The key to any male facelift, and the bald/shaved head patient in particular, is to have little to no evidence around the ears that the surgery was done. Limiting the incisions around the ear does compromise how ‘aggressive’ the facelift result can be but I think most men will settle for visible improvement of their neck/jawline with no minimal scarring vs a perfectly tight jawline and 90 degree neck angle with visible scarring.
A: Thank you for sending your pictures. I am not certain what qualifiers one as a ‘bald male facelift expert’ but I have certainly done a few such patients. The basic maneuvers of a facelift remain the same but with the caveats of some alterations of incisional placement around the ears. It is important that the anterior ear incision not go above the helical root and descends to the earlobe in a retrotragal fashion and that the posterior ear incision and backcut not go beyond the shadow of the outer helical rim. The submental incision for the central neck work remains the same as in any other patient. The key to any male facelift, and the bald/shaved head patient in particular, is to have little to no evidence around the ears that the surgery was done. Limiting the incisions around the ear does compromise how ‘aggressive’ the facelift result can be but I think most men will settle for visible improvement of their neck/jawline with no minimal scarring vs a perfectly tight jawline and 90 degree neck angle with visible scarring.
While longer scars that trail away from the ears do allow for more skin removal/tightening and better results, there is no forgiveness/improvement when such scars are done. This is an example of a patient that came to me with such facelift scars. No scar revision will ever make them go away. This is what one wants to avoid.
Dr. Barry Eppley
Indianaoplis, indiana
Q: Dr. Eppley, I like your explanation about Brow Bone Hypoplasia on website and I am thinking get this done, I am asian and I like the asian model’s result on that section, my purpose to have brow bone raised to have more eye depth and more defined look.
I do have couple questions if you don’t mind, where and how long is the incision for PMMA or HA on brow bone? in the hair? so the forehead skin would be opened to reach the brow bone right? I know Radiesse is calcium hydroxyapatite (CaHA) gel microspheres filler , can we reach the same result using Radiesse filler , multiple times of injection of course since most of it dissolves . lastly, 3D, you meant 3D printing right? what material do you use for that? is there a risk of implant movement in normal daily activities or exercises?
 A: Thank you for your inquiry. Permanent brow bone augmentation is done best by a custom brow bone implant, not injectable fillers or any form of bone cements. These require big incisions to place (bone cements) and are unreliable in shape. Custom brow bone implants are placed through small incisions using an endoscopic technique. Being preformed by computer design they have a reliable shape and can be properly placed to provide the soft tissue push to create the desired aesthetic effect. Once these implants are in position and secured they will never move despite what one’s daily activities or exercise regimen is.
A: Thank you for your inquiry. Permanent brow bone augmentation is done best by a custom brow bone implant, not injectable fillers or any form of bone cements. These require big incisions to place (bone cements) and are unreliable in shape. Custom brow bone implants are placed through small incisions using an endoscopic technique. Being preformed by computer design they have a reliable shape and can be properly placed to provide the soft tissue push to create the desired aesthetic effect. Once these implants are in position and secured they will never move despite what one’s daily activities or exercise regimen is.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,After a few months of thinking about this I think I want to reinsert fat back into my buccal area. Just not satisfied with the look, my face just looks too skinny. I probably just should’ve went with the buccinator myectomy and perioral mound liposuction initially cant change the past and can only move forward. My question is what would be the price to reinsert fat back into the Buccal area and was it documented the amount of cc in fat that was removed to fill the area back up properly? Thanks
A: There are two ways to restore buccal fad pad volume which is in the 2cc to 3cc range, fat injections or the insertion of en bloc (solid) fat graft back into the buccal fat pad space. Each method has its advantages and disadvantages. Usually the latter is more effective as it puts the volume directly back into where it was initially removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I only need a change my nose, a rhinoplasty revision. There is implant in my nasal bridge. My nose was very flat before the implant. What I need now is reduction the tip of nose and a symmetric nose. Is that possible?
A: Thank you for your inquiry and sending your picture. While obviously I have no idea what was done actually in your rhinoplasty (other than some type of implant was placed) I don’t yet have enough information to determine what type of nasal improvements can be done. To provide a qualified answer to that question I would the following two pieces of information: 1) a front view picture and 2) a copy of the operative note from your prior surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is ” Cool Sculpting ” an effective method of permanently reducing fat from underneath the chin? (double chin)
A: From an ROI (return on investment) standpoint…no. Surgery is far more effective. Such technologies exist for those patients who are willing to go to great lengths to avoid surgery…and are willing to accept a very modest non-surgical type of result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I was wondering whether you can return back to a contact sport like boxing after temporal muscle reduction and if so how long is it you have to rest.
A: You should be able to return to contact sports within 30 days or less after temporal reduction surgery. Since tissue is being removed you can not hurt the surgical result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been thinking about getting this looked at for some time. I am missing a tiny bit of bone in my brow bone just under my left eyebrow causing my eye to move freely within its socket (vertical orbital dystopia) as well as having a prominent left brow and what I’d like to do is get an MRI or anything to figure out what I could do to achieve symmetry within my face.
A: I think your right vertical orbital dystopia (VOD) is really part of an overall right facial hypoplasia. But the first place to start is to to get 3D CT scan of your face which will clearly show the location and extent of the right facial bone differences from that of the left side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a quick question for you, can you suggest a surgery to define my jawline (picture 1) so it looks like picture 2?
I noticed that when I tighten the skin around my jaw, like picture 2, I get the desired effect on my side. I have already a strong jawline by nature ( picture 3) but its not showing on the sides for some reason. Could you help with this in your practice?
A: What you are doing by biting down is flexing your masseter muscle creating a jaw angle enhancement of increased width. This is a pure lateral ramus augmentation which should be achievable by placement of an implant underneath the main section of this muscular region. How much implant width is needed to create that effect is speculative but I would estimate between 10 to 12mms per side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am currently interested in Lip Reduction. Based on my research, it appears that you have extensive knowledge in this procedure, so I just wanted to ask for your opinion so that I’m better informed.
I had a Lip Reduction procedure done almost 6 months ago and noticed almost no difference, except at the far left/right sides. I believe this may be because my doctor only removed tissue from the wet mucosa region. In fact, when I look at the scar in my lower lip, there is wet tissue on both side of the scar. From what I’ve read in your blogs it appears that the correct approach to Lip Reduction is to remove some amount of dry and wet vermillion? Or is the correct approach only to remove dry vermillion up to the wet/dry border? Why do you think so many doctors incorrectly remove tissue in the wet mucosa region only? Thanks for your opinion, I appreciate it! For reference I’ve attach a before and after photo.
A: I can not speak for what other surgeons do or what your surgeon may have done in regards to the approach to lip reduction surgery. But I have learned that effective lip reductions come from removing the more exposed dry vermilion, which is more effective at rolling back the exposed vermilion height. (which is how lip size is perceived) The wet mucosa is very mobile and will have little effect on reducing the exposed dry vermilion. I suspect that placing the scar line in a potentially more visible location is a more risky proposition to some surgeons.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My aesthetic concern is that when i look down my jawline disappears and i have a double chin, even from a raised head I have a slight wobbly double chin despite being like 145 5’10”.
I was wondering if off the shelf implants would work because I do not need to look like a movie villian, though I’d like to go for as dramatic off the shelf implants as available.
A: The difference between custom vs standard chin/jawline implants is not that one creates a more dramatic effect than the other one. It is more about controlling the implant design/dimensions before surgery and making the implant to specifically fit the patient’s anatomy. This potentially lowers the risk of certain aesthetic complications.
That being said in lieu of a custom jawline implant the other options are a standard chin/sliding geniopasty with standard jaw angle implants. Given your chin recession and the submental fullness a sliding genioplasty would be more effective at resolving these issues than a chin implant because of the forward pull of the chin bone on the submental musculature.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have inherited weak cheekbones from my father that have resulted in both under eye circles from the lack of cheek support and an overall very flat profile. It makes me look tired and even ill, but no weight gain can impact that area of my face. I would much rather have full, feminine cheeks with a visible curve.
1. Is this possible to achieve through standard implants or are custom ones necessary? Can you place tear trough implants and combined submalar shell implants at the same time?
A: It is never a question of whether a custom infraorbital-malar implant design is the superior approach for the complex topograpy of the eye-cheek area…because it always is. You only choose the old style approach of combining standard tear trough and cheek implants for pure economics reasons with the understanding that an inferior aesthetic outcome is better than none at all.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had a lip lift (about a month ago). The Dr. was a renowned and qualified surgeon who had excellent reviews and is considered one of the best at lip lifts. I only wanted a few millimeters off. about 3 mms. Despite my request he ended up taking off “half my lip” as he said or over 8 mms. I now have an A frame deformity. My mouth is constantly gaping open. I read your website about avoiding this. Is there anything that can be done to fix this? I’m heartbroken and in shock and depression. I also wonder if other places have a formal way of agreeing on pre-op plan in writing? Because there was no formal written agreement there was obvious miscommunication. I’m wondering if it is normal for this big of a procedure to just be verbal consent and no formal surgical plan or blue print, so to speak. Any help or advice you can give would be greatly appreciated.
A: One of the fundamental principles of all surgical lip lifts and advancements is that they irreversible. Once the skin is removed there is no putting it back. Subnasal lip lifts do relax/settle/drop down to some degree up to six months after the procedure. That is usually but a millimeter or two. So all you can do is give it time and see how much, if any, dropping of the central upper lip occurs.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have hip implants but they don’t look natural. You can see the contour of the entire perimeter of the implants. I have had them revised and the revision did not conceal the edges of the implants. Two questions:
1. Could sculptra be used to surround the hip implants and soften their edges so that my curves are nice and smooth?
2. Could fat injections or flap surgery be used to cover the hip implants and soften their edges so that my curves are nice and smooth?
Looking forward to your feedback.
A: You have three options to treat hip implant edging. 1) Injectable filler or fat injections, 2) reposition the implant under the capsule that currently exists (improved soft tissue cover) or 3) improve the edge shape of the implant. (some implants do not have a true beveled feathered edge) Since I don’t know what hip implants were used in you I can say how that would apply to you. In my experience #2 alone possibly combined with a better implant shape usually improves/solves the problem.
Dr. Barry Eppley
Indianapolis, Indiana
 Q: Dr. Eppley, I’m 25 year old I’ve having similar skull issues as attached, Is it possible to be reshaped kindly advise.
Q: Dr. Eppley, I’m 25 year old I’ve having similar skull issues as attached, Is it possible to be reshaped kindly advise.
A: Plagiocephaly is one of the most common reasons people present for skull reshaping surgery. Whether it is the back of the head and/or the forehead both skull regions can be reshaped.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a cranioplasty surgery done over 15 years ago which filled in my large brow bone and dents in my forehead. We did an MRI of my skull. He cut me from ear to ear and went that far with the cranioplast. The problem is that he did not raise the top of my head. My head looks very flat and slopes down to the back of my head. I wanted to know if I could get a custom implant to fit along with the cranioplast and raise the top of my head. I can sent a picture of what I am referring to.
A: Thank you for your inquiry and sending your pictures. Certainly a custom skull implant can be designed to raise the top of the head and otherwise create an overall head shape that matches better with the prior anterior cranioplasty procedure. The 3D CT scan will clearly show the PMMA material of the forehead and brow bone areas from which the design of an implant to create the desired changes to the rest of the skull can be done. The existing scalp scar provides a convenient point of access to place the implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, At birth they pulled my head so hard my skull really stretched out. I camouflage it well with my hair but its still bothers me. Are there any possibilities for Total skull replacement with custom implant?
A: While you can replace your skull bone with an implant, that will not be of any benefit since you can’t squeeze it down or make it smaller because of the brain which has expanded to fill that space that the skull shape has created.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have lip incompetence/mentalis strain. I have tried relaxing with Botox and it had worked but it is not permanent. I have been to the orthodontist and I have a slight skeletal open bite for which they said only jaw surgery would be able to fix my incompetent lips. However jaw surgery is a very risky and expensive procedure and I do not want to go through with it. Can a sliding genioplasty be able to bring the chin in a more forward manner and reduce the strain/incompetent lips? Thank you!
A: Improvement in lip competence and reduction of mentalis strain in some sliding genioplasty patients is one of the potential benefits of the surgery. But that would depend on what type of chin movements are done and what is the anatomy of the patient’s chin initially.
Dr. Barry Eppley
Indianapolis, Indiana