Your Questions
Your Questions
Q: Dr. Eppley, i just wanted to mention that I participate in a lot of contact sports especially in wrestling and kickboxing so would getting such a surgery be a good idea due to the constant pressure and blows put on my skull and would the implant be strong enough and hold its place in my skull. Also, are titanium implants an option? Because few other surgeons have that, thanks
A: In answer to your questions:
1) I never seen a solid silicone skull implant be a problem of exposed to external trauma. You can not fracture, fragment or deform a solid silicone skull implant. It is very much like putting a bumper on your skull. These implants are hard enough to get into place. They can be made to move or displace later as they cover too much surface area and their position is locked in by encapsulation.
2) Titanium implants are not used in aesthetic onlay skull surgery due to their tremendous cost as well as the needs to have a full coronal scalp incision for their placement. It is not that they can not be done but they provide no better benefits with their added liabilities.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I had a couple of questions regarding the amount of lengthening and the result prediction/estimate. You had previously mentioned that a patient could get close to 2 inches of overall broadening. On a page on your website (https://www.eppleyplasticsurgery.com/does-shoulder-widening-surgery-by-clavicular-lengthening-widen-the-scapula-as-well/) it is stated that there is about an 80% correlation between widening of the bone and of the soft tissue/deltoid to deltoid measurement.
As for the specifics of my surgery, you said that you could do 2 cm lengthening per side. 80% of 4 cm comes out to 3.2 cm, so about 1.26 inches total. In addition, I measured the surgery prediction before and after photos in multiple spots around the shoulder and factored in my current bideltoid measurements, and it looks like about 1.13 to 1.26 inches total widening, so a similar result to the above estimate but not close to 2 inches total.
Don’t get me wrong, the after prediction is an improvement. But I wouldn’t want to have an inaccurate idea of what to expect. My questions are:
1. Am I perhaps missing a factor in play when looking at this, or is that loosely1.26 inch total bideltoid increase a good estimate? I certainly realize each patient can experience different results, but I did have concerns when the numbers didn’t seem to add up to begin with, especially coupled with the fact that they came out to be very close to my own measurements of the picture, which was closer to one inch than two inches
2. Is more than 2 cm lengthening possible or do you think it would significantly increase chances of complications to the point of not being feasible? Perhaps 2.5 cm to 3.0 cm. I read a post on your website (https://www.eppleyplasticsurgery.com/can-clavicle-lengthening-be-done-as-much-as-3-5cms-per-side/) stating that 2.5 was the upper limit to what you believe would be reasonable. I noticed some minor discrepancies on surgery details on different pages of the website (I imagine due to new data becoming available or your own experience), so I wondered if that 2.5 limit is still your current limit at this time.
A: Understandably you are probably misinterpreting the role of computer imaging. While it is interesting to calculate how much shoulder widening was actually done on the image vs what amount of bone is actually lengthened, which turns out to be a pretty good correlation, that is not the actual purpose of the imaging.
Its role is really to determine what is the minimum threshold for the patient to consider the surgery worthwhile. If what was imaged was the ‘maximum’ amount of lengthening possible, would the surgery be worth it? That is its real role in helping the patient determine whether they would be satisfied. What I want to obviously avoid is to do this surgery and the patient say later that he thought it would be more.

 As to what more could be, or what is the maximum lengthening possible. that is really a question of geometry as well as one unknown factor….how much sagittal split lengthening can be done until the bone won’t heal. For example, if a sagittal split bone cut is made 3 cms in length, almost 10mm of bone contact in the middle can be maintained for 2 cm of lengthening of the clavicle. (see attached) This we know is safe/bone will heal. But if the split was made 4 cms in length, for example, the bone lengthening would be 3 cms per side. Would that heal as well as 2 cms lengthening per side….maybe.
As to what more could be, or what is the maximum lengthening possible. that is really a question of geometry as well as one unknown factor….how much sagittal split lengthening can be done until the bone won’t heal. For example, if a sagittal split bone cut is made 3 cms in length, almost 10mm of bone contact in the middle can be maintained for 2 cm of lengthening of the clavicle. (see attached) This we know is safe/bone will heal. But if the split was made 4 cms in length, for example, the bone lengthening would be 3 cms per side. Would that heal as well as 2 cms lengthening per side….maybe.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Last year I had a skull reshaping surgery (plagiocephaly is my problem), but i had an infection and they took out the skull implant. I treated infection for six months and now I ma cured I would like to try it again .
Can I have the information of how you treat the patient who has had this type of skull implant problem.
Thank you
A: Thank you for your inquiry. To determine if you are a good candidate for a second attempt at skull augmentation for plagiocephaly I would need some more information:
1) What type of skull implant was used? (what material and how was it made?)
2) What type of scalp incision was used for placement of the skull implant?
3) What was the identified bacteria? (cause of the infection)
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What’s the biggest oval size buttock in plant that can be placed intramuscular?
A: The general volume ranges of intramuscular implants is in the range of 300cc to 400ccs dependent on the size of the patient. Larger patients would be closer to 400ccs while smaller patients would be closer to 300ccs.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know what the cost of doing an extensive skull shaping surgery would be. I basically want some projection of my glabella tapering down the eyebrows and also I would like to add thickness to the forehead both below and above the hairline if possible.
I would also want to increase the sides of my head from the temporal region back. I have seen your custom implant designs and my overall goal is to basically get a thicker skull all around maybe 1 cm of thickness on the sides less on the forehead I would think due to managing the hairline proportions.
I am fine with scars, I believe I have the hair to cover it up well enough. What is a price range for what I would want? Do you preform this kind of thing more often now, once per week? I believe this will be more requested in the coming years (brow and head).
A: Thank you for your inquiry and detailing your skull reshaping goals. In custom skull implants, virtually any surface area coverage and thickness can be designed. That is never the question. Rather the key issue is whether the volume of the skull implant designed can ‘fit’. The concept of fit in skull augmentation means the ability of the scalp to safely tolerate the underlying implant without a significant increased risk of incisional dehiscence and scalp stress. (potentially seen as increased risk of infection and hair shedding/loss) As a general rule the volume of custom skull implants needs to be under 200ccs. Such volumes are always calculated in the design process and such information helps guide the implant design.
Just by your description (1 cm increase on the sides and coming across the forehead) I can tell you without even an implant design that is going to make a skull implant over 200ccs in volume.That would need an implant design that virtually covers 2/3s of the skull’s surface area. (to have an adequate feathering of the implant to blend into the rest of the skull’s convex surface area and to not look unnatural) As an aside to this observation, most patients way overestimate their skull augmentation needs by thickness and under estimate the expansive effects of large skull surface area coverage.
But for the sake of discussion for now let’s assume that your implant thicknesses/size is correct. That leaves you with two options; 1) do a two stage skull augmentation which requires a first stage scalp expansion or 2) reduce the dimensions of the implant so that it falls under 200ccs volume.
Dr. Barry Eppley
Indianapolis, Indiana
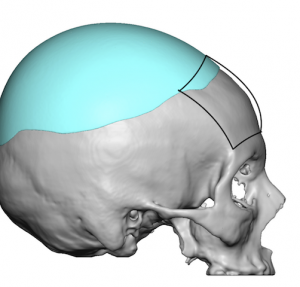
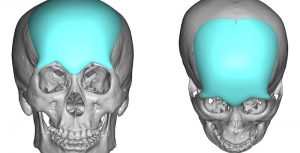
Q: Dr. Eppley, Hi! My head is flat and small I want it to be rounder and more asymmetric and not embarrassing, Specifically the top and back of my head are flat they don’t contain that roundness which some people have it.
A: Thank you for your inquiry and sending your picture. This is the most common area that women request for skull augmentation. In determining how much skull augmentation can be achieved there are limits to how much the scalp can stretch to accommodate a skull expansion by an implant. Thus the first decision to make is what degree of skull augmentation can one accept vs how much is one willing to undergo to achieve their ideal result. This is where the concept of immediate vs a two stage skull augmentation procedure must be considered. To help make that determination I have attached a drawing of the likely differences in shape between these two choices.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had this x-ray a few days ago, and here it is clear how wide my clavicle is and that my ribs are very close to my hip bone, for this reason you do not see a thinner waist, having this type of ribs so large and united, does it make it impossible to operate and have a lot of risk since several important organs were down?
A: Thank you for sending your picture and x-ray. Rib removal surgery does not pose any risk of organ injury, that is a common myth/misconception about the surgery. I see nothing in your x-ray that would preclude you from having rib removal surgery.
Dr. Barry Eppley
Indianapolis, Indiana
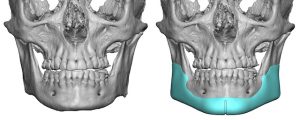
Q: Dr. Eppley, I am 4o years old, past surgeries include Lefort 1 osteotomy, rhinoplasty, septoplasty, along with braces. I had a class III malocclusion, maxillary deficiency and crooked nose. I feel very subconscious about the look below my eyes and my hollow cheek and eye area. Like my jaw area is out too far now. I would like to see what you would recommend to make me look better. Thank you
 A: Thank you for your inquiry and sending your pictures. What you have is essentially an incompletely treated midface deficiency. While the alveolar level of the midface may have been treated/corrected by the LeFort I osteotomy, every structure north of that was ‘left behind’. To get a more complete midface augmentation effect a custom midface implant is the definitive procedure and far easier to undergo and recover from that the LeFort I osteotomy by comparison.
A: Thank you for your inquiry and sending your pictures. What you have is essentially an incompletely treated midface deficiency. While the alveolar level of the midface may have been treated/corrected by the LeFort I osteotomy, every structure north of that was ‘left behind’. To get a more complete midface augmentation effect a custom midface implant is the definitive procedure and far easier to undergo and recover from that the LeFort I osteotomy by comparison.
There are different variations of the total midface implant that are customized to the patient’s specific aesthetic needs but the general footprint of the implant is largely the same.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi. I had calf implant surgery to help correct the imbalance In my lower legs. I tore both inner heads of my calves during spotting activities. I am not happy with the implants that I have. They only look somewhat ok when viewed directly from behind. The projection is all wrong and they are not nearly wide enough. The implants do not resemble a natural calf muscle. I wanted custom made implants shaped to my leg. I called a company name Implantech and they can help with custom implants unless you know and use another. Please let me know if we can speak further. Thank you.
A: While you can have custom calf implants made that offer better surface coverage by design, I would caution you that your existing calf implant replacements is not quite as simple as just swapping them out. The now etsablished implant pocket will need to be extended which is difficult to do through a remote behind the knee incision. There is also the risk of creating a visible scar line between the old and new calf implant pockets due to the capsular release needed to accommodate the larger implants. This can create an unaesthetic line down over the new larger calf implants.
While this aesthetic issue may not occur one needs to be aware of its possibility since there is limited control over how the overlying soft tissues will respond to the edge of the capsular release.
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about skull reshaping (or temporal implant). I have already done a back of head augmentation 4 years ago, but it was in South Korea and with bone cement. I initially suffered from back of head asymmetry. The back and one side was flattened. The operation i have done in South Korea helped for the back of the head, but one side is still a bit flattened. The doctor said it coulnd’t go there because of temporal muscle. The flattening begins juste behind the ear.
My first question is : is it necessary to remove what have be done with the first operation ?
And if the answer is yes, is the scar big to remove that ?
A: What you had done was a bone cement augmentation which must stay restricted to bone as it will not stick to muscle. Because most plagiocephalic back of the head flatness wraps around the side you ended up with incomplete correction.
You can simply add what is missing by a custom implant design from a 3D CT scan which can wrap around the side going from the bone cement and as far forward as needed over the temporal fascia for the correction.
For now I assume the existing scalp incision/scar can be used for placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have testicle implants that I am not happy with. They are by AART and they feel a little too hard. Do you use Implantech Extra Extra soft implants? Are they worth me looking into? It’s hard for me to find anyone who has used them or knows about them. I am interested in you doing the procedure to change them.
Thanks
A: I can not speak for AART testicle implants as I have never used them. I have only used Implantech’s testicle implants where an ultrasoft solid silicone durometer is used as that is what I insist they be made of so they feel appropriate. I can only assume that the softness of the silicone testicle implant I use is softer than that of AART.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, You say that it is possible to start the custom skull implant process after the scalp expander stage, only you told me that the scalp expander must stay in place for 6 weeks and that the average time for the implant process is 13 weeks. The scalp expander will have to stay in place for 13 weeks under the scalp. Is this not a problem?
Also regarding the scalp expander device, does it imply any particular conduct in daily life? Stop doing sports? Avoiding certain activities or situations? Can I sleep normally?
I would also like to know, when the patient comes for the scalp expander, can you examine our head and discuss together the best correction to make? And make a mold of my skull, for example?
Concerning the fixation of the implant, you talk about small screws, can this lead to cranial lesions? How do you fix them? I have seen several of your videos where you insert the cranial implant but I have not seen any where you fix it with the screws. Is there a place where I can see them?
A: In answer to your scalp expander questions:
1) Scalp expanders can stay in literally forever. The time of 6 weeks for scalp expansion is the absolute minimum time…longer is always better.
2) I wold avoid contact sports while the scalp expander is there. You sleep in whatever position is comfortable.
3) The 3D CT scan can be used to make an exact 3D skull model if one so desires.
4) Almost every skull implant I have ever done had the use of small screws. They do not cause cranial ‘lesions’.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My facial asymmetry is something that has bothered me for quite some time now. The left side of my face is clearly larger than the right, and my right eye appears to be farther back than the left. I believe I may have a minor case of hemifacial microsomia. It is especially noticeable when my head is tilted up. Could a custom-fitted jaw implant on the right (smaller) side + fat grafting help to minimize the asymmetry? Also, are there any options to reduce the asymmetry in my eyes?
I have attached some photos if you wouldn’t mind taking a look.
Thank you,
A: Thank you for your inquiry and sending all of your pictures. You have a classic right facial hypoplasia which affects all of the structures of your right face to varying degrees. The jawline, orbit and cheek bones are the most affected. Custom implants for the jawline, orbital floor/rim and cheek are the most effective treatment approach. Fat grafting in a yung lean person is almost never ofany benefit because it survives poorly.Tye greatest limitations are in the eye itself as it is able to be raised a bit but can not be brought forward. (it is important to remember that the eyeball is attached to the optic nerve so trying to pull it forward has obvious risks)
But beyond these general concepts the first place to start is by getting a 3D CT scan of your where the skeletal differences between the two sides of your face will be clearly seen and which serves as the basis for custom facial implant designs to treat the asymmetry.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, Hi I have a longer side of my face, I had double jaw surgery here in Montana, but it didn’t change the length of my left mandible which is too long and I wish for a symmetrical face please help thank you so much
A: Thank you for your inquiry and sending your picture. Since you have had orthognathic surgery you must have postoperative x-rays from the surgery. Those would be helpful to review the different lengths between the two sides of your lower jaw to determine what could be done and how such a jaw reduction may be able to be done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi there, i would like to lengthen my forehead with implant, is this possible ?
A: That depends on what you mean by ‘lengthening the forehead’. A forehead implant can potentially increase between the eyebrows and the frontal hairline in some people and based on the implant’s design.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have retracting testicles and seem to be always clenched, which make them look even smaller. Would I be a candidate for the “encased” implants or how would that be approached?
A: Thank you for your inquiry and sending your picture. My concern is that scrotal skin seems very tight and it is unclear how much it could stretch to accommodate more internal volume. That issue aside given your testicle:scrotal size ratio the wrap around testicle implants would be the only effective approach….which also helps with the scrotal sac skin issue as this implant approach uses your existing testicles as part of the implant. (unlike the side by side implant approach where the implant adds entirely new volume)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Due to my remote location (Australia) I won’t have access to a surgeon who works with custom/3d planned implants. I am in need of vertical augmentation, and i also have some asymmetry which means the implants have to differ somewhat. If need be, would it be possible for a surgeon with the vertical lengthening implant to shorten/cut down the vertical length of the implant on the spot, say from 11mm to 9mm lengthening, or would this be impossible?
 A:I am bit uncertain as to the exact nature of your question as there are no standard vertical lengthening total jawline implants. You may be speaking in reference to the standard vertical lengthening jaw angle implants which can be intraoperatively modified. (reduced)
A:I am bit uncertain as to the exact nature of your question as there are no standard vertical lengthening total jawline implants. You may be speaking in reference to the standard vertical lengthening jaw angle implants which can be intraoperatively modified. (reduced)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am concerned about my lower third and overall facial features from a purely aesthetic point of view. I am planning on signing up for an official consultation but I first want your opinion and some advice. Thank you in advance for your time.
 A: Based on just this one front picture it is clear that the major deficiency in the lower third of your face is vertical in nature. What you need for better facial balance/proportions is vertical jaw lengthening which can only be accomplished successfully by a custom jawline implant design. Whether there may be other jawline dimensional needs can not be determined by just a front view picture only.
A: Based on just this one front picture it is clear that the major deficiency in the lower third of your face is vertical in nature. What you need for better facial balance/proportions is vertical jaw lengthening which can only be accomplished successfully by a custom jawline implant design. Whether there may be other jawline dimensional needs can not be determined by just a front view picture only.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I’m a former patient for a two step skull implant. First off it was life changing for me! But years later, I still feel flat in the back of my head and I’m also interested in a forehead augmentation. I’m curious what a process like this would be since I already have an implant over the top of my skull? Thank you!
 A: Good to hear from you as it has been almost 5 1/2 years since your skull implant placement. I believe the question you are asking is whether you can have a forehead implant with an indwelling skull implant. The answer would be yes as forehead implants do not ever pose the same volume issues as your existing skull implan did. The only questions about the forehead implant are logistical in nature such as its actual design and incision location to place it. The forehead implant would need to be designed to integrate with the existing skull implant, making it essentially like an extension of it for a more complete form of skull augmentation effect.
A: Good to hear from you as it has been almost 5 1/2 years since your skull implant placement. I believe the question you are asking is whether you can have a forehead implant with an indwelling skull implant. The answer would be yes as forehead implants do not ever pose the same volume issues as your existing skull implan did. The only questions about the forehead implant are logistical in nature such as its actual design and incision location to place it. The forehead implant would need to be designed to integrate with the existing skull implant, making it essentially like an extension of it for a more complete form of skull augmentation effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, hello. I had double jaw surgery before. Can a custom made Total jawline implant be placed on it?Is there any risk?
A: It is very common to see patients who have had prior jaw surgery (sagittal split osteotomies, chin wing osteotomies, V line jaw reduction) for custom jawline implants. Such prior surgeries pose no issues for performing the surgery nor increase the risk of complications from it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, there’s a small discussion going on (url below) on one your patient’s threads about the shoulder rolling which you write can occur temporarily during healing. The point I’d like to clarify with you please (so I can add to the discussion), is, skeletal wise, how do/can the shoulders go back to being straight/back again despite the ‘geometry’ of the clavicle bones being shorter and thus pulling the shoulders forward?
Also, post healing, would back arch exercises (which really pull the shoulders back) be contraindicated, or would they be fine?
A: All I can say about it is that, so far, no patient has told me yet that inward shoulder rolling is a long term problem. The operative words here are ‘told me’ which could mean maybe some patients have it but have not gone out of their way to tell me about it during our postop virtual followups.
The medical answer to your question is that, according to the orthopedic literature based on extensive clinical data from patients with unoperated clavicle fractures where length shortening is a common sequeale, shoulder function is not adversely affected when the clavicle length has been compromised by less than 30% of its original length. They do not comment on appearance since this is from the orthopedic surgical literature.
Once the clavicle is full healed (8 weeks) shoulder/back stretching can certainly be safely done which would very likely overcome any inward shoulder rolling from clavicle length reduction if it persisted.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Are the insertion of the forehead implants performed by you? If so, how invasive/risky is it, and would they be placed behind the forehead muscles?
 A: In answer to your forehead implant questions:
A: In answer to your forehead implant questions:
1) Since I am the surgeon I am the one who performs all aspects of every surgery that I do.
2) Having many forehead implants the risks of the procedure are really aesthetic in nature…how well does the implant design achieve the patient’s aesthetic forehead reshaping goals.
3) Forehead implants are placed in the subperiosteal tissue plane directly on top of the bone which places it behind all overlying soft tissue layers.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would I be suited more to the V to Y mucosal advancement lip lift? As there is no scar but not sure it would achieve the look I want?
I like the curved off look going from the top to the sides rather than straight diagonally down, so that it gives a more fuller top lip
I’d like my top lip practically matching my bottom lip for size
Also if you can tell me is the scar noticeable on the Gullwing liplift?
Here are a few photos top 3 are me the rest are how I want my upper lip to look.
 A: The vermilion advancement procedure is the correct lip reshaping procedure given your objectives. ironically the scar line in men does better than in women because of the hair bearing skin. (see attached)
A: The vermilion advancement procedure is the correct lip reshaping procedure given your objectives. ironically the scar line in men does better than in women because of the hair bearing skin. (see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley: I am planning to get cheekbone reduction and currently my biggest concern is skin sagging. But i already accepted the risk of skin sag i just want to minimize the severity. I read somewhere cheekbone reduction through coronal incision reduces the risk of skin sagging. Is it true? Which method is better?
A: It is true that the risk of soft tissue cheek sagging with a superior coronal incisional approach in cheekbone reduction osteotomies is less. This is because the stripping of the soft tissues off of the cheek coming from an inferior (below the cheekbones) intraoral incision is avoided. But there are adverse aesthetic consequences to the scalp approach as well, primarily the long scalp incision, the risk of visible scarring and the longer duration of the surgery which will increase the cost of surgery.
Ss you can see no approach to cheekbone reduction surgery is risk free. Your decision as to how to do cheekbone reduction surgery is based, therefore, or which risks you choose to accept if you have the surgery.
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a cheek implant put in 25 years ago. Due to stress I have been grinding my teeth at night. I do wear a mouthguard. Twice over the past few months, I have woken up in pain where the implant is located. The first time I thought I had an infection in my gums and I took penecilin. It did go away but I was also very careful about managing the grinding. I just woke up 3 days ago with the same pain. I believe it is the implant and not a gum problem. I can’t even chew on that side it is too painful.
A: I believe what you are experiencing is a problem with your cheek implant. Undoubtably with such old cheek implants they are probably placed anteriorly with a downward angle, putting them close to the maxillary vestibule. Short of a tooth-related problem, which I can not say does not exist, the next culprit would be the cheek implant. The key question now in their management is whether implant removal alone is enough or whether replacement is desired.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in cheek implants hoping to eliminate the concave appearance of my cheeks and if possible strive for a more symmetrical appearance.I had cheek implants last year and think there’s plenty of room for improvement;).
Thank you for your time and I look forward to hearing from you.
A: Thank you for your inquiry and sending your pictures. The key to determining how to augment your cheeks better is to know what type of cheek implants you have in and where they are located. There is no sense in guessing or eyeballing how to improve things. That is why I would get a 3D CT scan which will reveal that valuable information. Once you know what isn’t working well it allows one to determine what will work better.
That is a scan we can order for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question. Is it possible to have a sliding genioplasty for the chin and create a custom wrap around jaw implant together. Reason I ask is that I think I need vertical length in my chin and it’s my understanding that chin implants only give horizontal lengthening.”
A: Combined sliding genioplasties with custom jawline implants are not uncommon. They are done when the desired chin augmentation dimensions, usually vertical, exceed what the soft tissue chin pad can safely cover. This usually is done when the combined vertical and horizontal augmentation dimensions exceed the combined number of 12.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I believe I may have excess perioral fat, and I am writing to enquire exactly what these pockets of fat around the highlighted area is.
I am situated in London England therefore I am asking to get an opinion on what exactly the right procedure could be. I have already had complete buccal fat removal however this treated my middle cheek and not the perioral area.
Could these be treated with an injection such as Kybella or would micro lipo be a more appropriate approach?
A: Kybella never works for fat reduction in that area, it requires liposuction alone or combined with a buccinator myectomy. In thinner faces it is most likely going to require both to create your outlined effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My concerns are that my sagittal ridge reduction will be sufficient enough. That there will be no long term affects from having it done. And that I can fly home the day after the surgery as I was told at my virtual consultation.
A: In answer to your questions:
1) In sagittal ridge reduction the maximum amount of height is reduced that the bone thickness will permit. Whether the line you have drawn can be achieved can only accurately be determined by a preoperative 2D CT scan to visualize and measure the bone thickness.
2) I am not aware of any long term effects from the procedure.
3) A drain is used and is removed the following day. One can go home thereafter.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I for two years I have been looking for a solution to my problem. I had a genioplasty (periosteal detachment of the mandible with milling of the chin bone relief with the pineapple ball). Since then, my chin is hyperdynamic (spasms all day long) and all the chin tissue is falling (including the mentalis muscle). It is very annoying and my chin is very long like a witch at rest and even more when I laugh. You can see my incivilities and I have to force my mouth shut. Here in France, the problem is little known. I have read your articles, you are an expert in this matter. Can my chin problem be totally corrected? I’m talking about aesthetically because my face is disfigured because of this witch’s chin and medically because I can’t even close my mouth and the spasms make me tired.
The first picture is me before genioplasty. Is it possible to get back the exact same chin I had before the surgery? Can surgery solve all my problems both aesthetically and functionally? Or is it complicated?… What do I have to do to remove the mentalis and the submental skin? I would like to get back the exact same chin I had before.
A: This is exactly what I would expect to happen from a poorly thought out chin reduction procedure. When you detach the soft tissue and reduce the bone support this creates the problem of soft tissue chin pad excess. The chin pad has virtually no ability to contract when the bone support is removed leading to chin ptosis, either at rest, smiling or both. As a result, the redundant soft tissues ball up and the mentalis muscle never works quite the same because it has lost its original working length.
Improvement is possible and the technique to do so depends on whether the chin bone is desired to be restored or not. If so I can consider an intraoral sliding genioplasty with muscle/chin pad resuspension. If not then a submental excision/tuck is needed.
Dr. Barry Eppley
Indianapolis, Indiana