Your Questions
Your Questions
Q: Dr. Eppley, I have some custom forehead implant questions for you.
Question 1: I was wondering if you could reshape a flat forehead into a youthful rounded protuding forehead I had in my early years using custom made forehead implants .I wanted a more concave forehead Ala Rihanna . Will it be able to look natural and not uncanny ?
Many people get frontal bone /brow bone reduction to change a concave forehead into a flatter profile is there such a procedure I can achieve the opposite
Lastly Will my forehead feel numb ? Can I still form wrinkles in my forehead ? Will my eyebrow position since I do Not want to change my eyebrow position or get a super shiny forehead . Lastly how is the scarring for the procedure like?
A: In answer to your forehead augmentation questions:
1) With the proper design a custom forehead implant would be the only way to get a more rounded and less inclined forehead shape.
2) Every forehead augmentation patient will have some temporary postoperarive numbenss andf stiffness of eyebrow/forehead movement. But this will resoolve within 6 to 8 weeks after surgery.
3) The way to avoid an uncanny/unnatural look after forehead augmentarion is to not make it too big.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, do you perform subcranial modified orbital box osteotomies?
 A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for properly selected adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is aesthetically needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect would also be desired.
A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for properly selected adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is aesthetically needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect would also be desired.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I have been searching extensively for a plastic surgery solution to my deep dark circles/hollow tear trough problem since i was young. I do not desire fillers or fat transfer because of the impermanence and unpredictability of the procedures respectively. I came across infraorbital rim implants which seem to have a beautiful and permanent aesthetic outcome. I was told by a dermatologist that the source of my deformity was a lack of sufficient bone structure around the eye region rather than tissue loss/migration. I read in a research article that an abnormally connected orbitomalar ligament can also play a role, where release may be necessary to correct the depth of the indentation. Furthermore, I read about the various customizable implants on your website and thought it would be perfect for me as i desire volume to be restored under my eye as well as an extension into the malar region to give me a more chiseled cheekbone projection that i am lacking. The tissue around this area appears to have a flat/sagging appearance because it doesn’t seem like there is enough support holding it up until i artificially mimic the motion with my fingers and lift up my cheeks. Please let me know if the implant would be suitable or if something else could be done better. I also desire more symmetry in my face as I have noticed that one side appears to be more developed than the other. I do not know exactly what procedures can correct this, as I haven’t researched too much into it, but if you can recommend something that wouldn’t be too surgically aggressive, that would be helpful for me. I’ve looked through many photos of your work and I greatly appreciate your aesthetic outcomes. I’ve attached two photos for reference of myself. Thank you very much
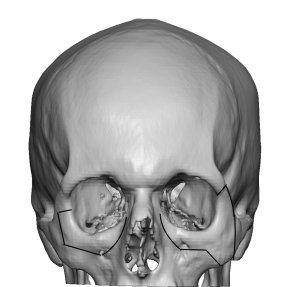
 A: You have correctly identified the proper treatment for your undereye hollows/tear troughs….infraorbital rim augmentation. The only debates are: 1) whether standard vs custom infraorbital implants are to be used (see attached) and 2) whether there should be a malar extension to them or not. The first one is not much of a debate as when you have known asymmetry beforehand using standard implants will almost always make the asymmetry appear more pronounced. That combined with the need in infraorbital bony deficiencies to add both horizontal projection and vertical rim height, only a custom infraorbital rim implant can make those dimensional changes. As for any malar extension to the infraorbital implant that is an individual aesthetic decision of which you have stated that would be a good addition for you..
A: You have correctly identified the proper treatment for your undereye hollows/tear troughs….infraorbital rim augmentation. The only debates are: 1) whether standard vs custom infraorbital implants are to be used (see attached) and 2) whether there should be a malar extension to them or not. The first one is not much of a debate as when you have known asymmetry beforehand using standard implants will almost always make the asymmetry appear more pronounced. That combined with the need in infraorbital bony deficiencies to add both horizontal projection and vertical rim height, only a custom infraorbital rim implant can make those dimensional changes. As for any malar extension to the infraorbital implant that is an individual aesthetic decision of which you have stated that would be a good addition for you..
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in testicular enlargement. I have attached some pictures of my scrotal ultrasound.
A:With natural testicles at 3.9cms on the right and 3.7cms on the left you are in the ‘gray one’ of the two testicular enlargement methods. If you were a bit smaller than the side by side method with 6.0cm or larger imnplants with a very low rate of problems could be used…and which is always the preferred method. If you were any bigger then the wrap around method is preferred with its relatively higher rate of complications which is always the risk of implant separation from the testicle. In this size testicle it tis always a difficult decision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in testicular enlargement. I have attached some pictures of my scrotal ultrasound.
 A:With natural testicles at 3.9cms on the right and 3.7cms on the left you are in the ‘gray one’ of the two testicular enlargement methods. If you were a bit smaller than the side by side method with 6.0cm or larger imnplants with a very low rate of problems could be used…and which is always the preferred method. If you were any bigger then the wrap around method is preferred with its relatively higher rate of complications which is always the risk of implant separation from the testicle. In this size testicle it tis always a difficult decision.
A:With natural testicles at 3.9cms on the right and 3.7cms on the left you are in the ‘gray one’ of the two testicular enlargement methods. If you were a bit smaller than the side by side method with 6.0cm or larger imnplants with a very low rate of problems could be used…and which is always the preferred method. If you were any bigger then the wrap around method is preferred with its relatively higher rate of complications which is always the risk of implant separation from the testicle. In this size testicle it tis always a difficult decision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in an implant that could give a more forward grown forehead/browridge and slightly reduce the slope as well as a vertically longer forehead. My 2nd interest would be correcting a very weak/almost non existant occiput. Ideally it should go from the browridge all the way to the end of the occiput. My last concern is that my head size is way too small for the rest of my body, so a rather large augmentation would be preferred. I would like to know under which price range such an implant would be in. Thank you.
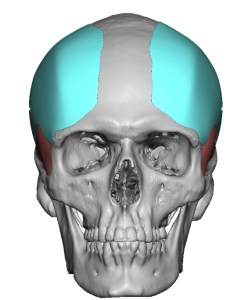
A: Essentially what you are referring to is a one piece skull implant design that goes from just above the brow ridges all the back to the occiput. While that can be done such large surface area implants add a lot of volume in which the scalp has a limited ability to stretch to accommodate it. This the size/thickness of the implant must factor in the soft tissue scalp which means either a smaller volume implant is used and immediately placed or a two stage skull augmentation is done using a first stage scalp expansion to end up with an implant that would have double the volume.
To best understand the aesthetic differences between a one vs two stage skull augmentation with that surface area of coverage I would need a side view picture to do some imaging to show you those different effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 26 old female and I write you because I have a concern about the shape of my forehead bone. I thought it was lack of fat and thin skin, because i can see bones in all my body, but I read one comment of you under the post of a girl with more or less the same case of me in which you was talking about frontal deformity. I would ask you if in my case it’s a deformity of the bone. Thank you and best regards
A:While you did not clarify your exact forehead shape concerns I am going to assume based on your pictures that you are referring to your forehead eminences also more commonly known as forehead horns. (paired upper forehead bumps) Whether that bothers you or not determines whether it is an aesthetic deformity. Presuming that it does those forehead horns can be reduced/burred down to have a smoother forehead contour.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I´m a 42 year old male interested in getting custom-made wrap around jaw (and chin) implants. While considered reasonably good-looking, I´ve always been lacking in self-confidence owing to what I perceive as receding, narrow chin and weak, underdeveloped, receding lower jaw. To address the aforementioned – I´d had a Medpor two-piece chin implant (5mm projection) inserted back in 2008. As it failed to address any one of the described issues, I´ve had it removed in 2015 and replaced with a large silicone chin implant, which, alas, also proved insufficient and inadequate in providing me with a full, robust, chin and lower jaw. To add to the existing problem, the implant also rotated downwards and suffice to say it doesn´t sit properly in its pocket. Since then I´ve tried to treat the receding jaw with fat transplant along the lines of my jaw but that failed to give me that chiselled and robust look the lower jaw should project.
That custom wrap around jaw and chin implant should address
1. receding chin – projection
2. narrow chin – width
3. “short” chin – vertical length
4. depressed jowls – projection
5. receding, underdeveloped lower jaw – projection, width …
Is that achievable? Can wrap around implants “elongate” the lower third of my face the same way Chin-Wing can? Since I have a fairly pronounced case of receding chin, would it be possible in one procedure to remove my silicone chin implant do genioplasty AND on top of that insert wrap around jaw and chin implants? Or is that rather too ambitious? The reason for asking is that I´d rather skip the hustle of undertaking several trips all the way from Sweden, Europe. Also, would fat transplant interfere in any way with the custom made wrap around implant, at least in terms of blunting the final results? If so, should/can it be removed during the surgery?
Finally, would it be possible to get an approximate cost estimate for the surgery at this point?
Of course, I do have more questions, especially in relation to patient safety (for patients outside the US), results, recovery, accommodation during my stay etc., but let us leave those for another time.
Thank You!
Looking forward to Your answers.
A:What you are describing by what you want to address is exactly what a custom wrap around jawline implant does. What it can achieve dimensionally is far superior to the chin wing osteotomy. Your surgical history describes exactly what the limitations of the procedures you have done for lower third of the face augmentation are. The only question is where the custom jawline implant is needed by itself (with simultaneous chin implant removal) or whether your chin augmentation needs as such that it is better to combine a sliding genioplasty with the custom jawline implant. That determination will require photographic imaging of your face as well as a 3D CT scan. Your fat grafts do not need to be removed nor so they pose any limitations in the result as they are likely of low volume.
When you get a chance please send me some facial pictures so I can begin the imaging process. The 3D CT scan can be done in your country as my many Swedish patients get in their geographic area.
All surgical planning is done in a virtual manner so you only come here one time for the surgery. Followups are also done virtually.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was looking at the head reduction surgeries, in particular occipital reduction. I just have one question left before I want to arrange a consultation
My question is, in general how much head circumference reduction can you expect. You posted that the average reduction in the back is around 7 milimeters. So does a 7 milimeter reduction in the occipital area result in a 7 milimeter head circumference reduction aswell or is it different? Is it possible to calculate it? I know its a hard question to answer but if you could give me an average estimate of the head circumference reduction that happens after the occipital reduction from previous patients. I sent a picture so you can look at it as well.
Thank you for your time
A:That is a very good question to which there is no exacting answer since the reduction in bone projection does not correlate with reduction in circumferential measurement in a linear manner. I am certain there is a mathematical way to answer this question based on spherical geometry but that is beyond my expertise. Rather than circumferential measurements I focus on what aesthetic effect will be achieved in profile projection which is a lot easier to see. Certainly the red line you have drawn in your photo is beyond what 6 to 7mms of bone reduction would achieve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have upper and lower lip incompetence and due to that i have mentalis strain. My upper lip is brought down with botox but I still have a lower lip incompetence and I think this is due to a receding chin (not that much). But, I have had also an open bite but I now have porselein crowns. So my teeth touch but I feel like my jaw is still not in the correct place. I don’t want to get a jaw surgery and was considering chin filler. Will this help with my lower lip incompetence? And does filler still work if it is injected in a restrained chin? Or should the chin muscle first be relaxed, which will make my lower lip hang more?
A: The benefits of injectable fller is that they are easy to do and are reversible. Whether adding volume to the chin by fillers will improve your lower lip incompetence i can not say but there is one way to find out…do it!
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is there a solution for eyes with relatively no support? I have extremely deep set, sunken eyes. I am prone to lines and premature wrinkles. There is almost virtually no fat. From far away, they are “black holes”; shadows are cast.
I want youthful, forward eyes. It’s impossible to change the position of my eye (it is quite far back in the socket”, but perhaps there is a difference solution? Implants?”
Please let me know your thoughts,
A:Deep set eyes means that the eyeball position relative to the surrounding orbital rim is further back. Since the eye is tethered by the optic nerve its position can not be changed. Thus only the surrounding supralateral orbital rims can be reduced to make the eyes look less deep.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a plastic surgeon in Canada. I have taken Dr Eppley’s implant courses. I have a case I wanted to ask Dr Eppley. I performed a male face and neck lift. At the time I placed temporal shell implants. The left implants migrated superior, and the right sits slight lateral. When should I revise this? What should be done differently at the time of a revision? Thank you for your help.
A:This is an initial pocket creation issue most likely. As a general rule they really don’t migrate superiorly…at least not in my experience. Under creation of the initial pocket is easy to do. While a secondary pocket expansion can be done the real question is what is going to hold the implant down into the proper position in a soft tissue pocket where fixation of the implant is not usually possible?? It may work just by expanding the pocket but the definitive solution is an implant that has a bigger footprint than the original one.
Another option is to leave the implant where it is and fat graft around it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to reduce the sides of the frontal bone? I’ve always been very insecure about the shape of the sides of my forehead bone. It is not a big amount of bone that I want to be reduced. Just the sides. Could I show a picture of my forehead to show what I mean?
A:You are undoubtably referring to the sides or bony temporal lines of the forehead…the most common area of the forehead to reduce in females that have too wide or square of a forehead. But seeing a picture of your forehead would help to confirm my assumption.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, ! I had a 7 mm medpor implant placed 4 months ago. I immediately knew that it was too big and begged my surgeon to remove it at 2.5 weeks post op. I did not want to wait 3 months for the results as I was certain I would have it removed and I was afraid that the longer it was in the harder it would be for the tissue to return to its pre-op shape. He refused to remove it and insisted that there would be no harm in waiting. I sought out other surgeons in my country to have it removed, but he was the only one that could do it and so I had to wait.
3 months later I had it removed. I asked him beforehand if it was necessary to do muscle re-suspension/soft tissue management, but he said no. He believed that it would just snap back to how it looked before.
Well, I am now 1 month post op and I think it looks pretty bad. I know I am still swollen, but my chin pad squares off when smiling and sort of “hangs”. I have a hard time believing that it will just fix itself like he promised. I haven’t been able to get in contact with my own surgeon (and frankly I don’t trust him anymore), so I was hoping that you could tell me if this was normal or if I might need another surgery to fix it?
A:Time will provide the ultimate answer to the question of whether the soft tissue sequelae from the Medpor chin implant removal will need to be addressed. It would be fair to say that the chin pad soft tissues just ‘snapping back into place like before’ was never a realistic outcome as the osteocutaneous ligaments have been released to place the implant. It is more likely than not that what you are seeing now will not significantly improve. But the soft tissues do need to heal more and fully relax before any secondary management is done which should not the considered before 3 to 4 months after the implant removal if not longer.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, About 3 months ago I had plastic surgery and was given a MEDPOR Cheek Implant. I am not happy with it at all and want it removed as soon as possible.
I googled MEDPOR Cheek removal and your information came up.
Will my skin be saggy after even having it in there only for about 3 months?
Or can something be done to counter act?
I just would like to look like myself again.
Hope to hear from you soon.
A: The time that the implant has been in is irrelevant. The surgical act of releasing the osteocutaneous ligaments tp place the implants is the source of any potential soft tissue sagging. There is no surgical technique that can reliably replace/restore the ligamentous attachments. Thus you remove the implants and see whether such soft tissue sagging is significant or not.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 24 year old male who currently has a Vertical Lengthening Chin implant (Medium) in. This implant has made my face more wide, square and my chin now comes a little past my bottom lip. I actually like this new look, but I am very bothered by the mandible area not blending into the front of my face. I have a slightly visible ridge on one side too. I presume that this is because the rest of my jawline is not as thick as the implant – so it does not have a very seamless look to it.
I am interested in a Vertical Lengthening Jaw implant to bring down the jaw angle and make my new chin look more natural. However, I want there to be something that fills the space between the Vertical Lengthening Jaw implant and my chin implant so that there are no visible or very palpable ridges/deformities/etc. I do not mind more bulk on my face, as I am very slim and the bulk of the chin implant has improved my aesthetics.
I have looked through the Eppley blog and researched the potential options for my goals. It is not in my budget to have a custom wraparound jaw implant. I am not preoccupied with the sharpest angles or the most symmetrical face so I am hoping an off-the-shelf or semi-custom option would satisfy my goals. I’d like an elegantly squared off look like the reference photos I have attached. From my research, I am interested in these potential options listed below (unless there is an option that you find to be more appropriate, of course):
– Vertical Lengthening Jaw implant and carving from a silicone block to fill out the lengths of my jawline in accordance with the chin/jaw implant(s)
– Semi-custom implant of some sort?
I am inquiring about the cost of these options and what you think would be the best option for me in particular. Anything that will not show irregularities and is more affordable than a custom wraparound implant would be a considerable option.
A: There is no question that the only effective way to make the jawline behind the chin implant be augmented in a seamless manner to it is a custom implant design approach. Any other method is going to have its aesthetic complications because 1) placing jaw angle/jawline implants is infinitely more challenging than the simple chin implant and 2) there are two sides/implants which adds to the difficulty of the procedure. I would not even try to do it any other way because I well know what will happen. There are times in this type of surgery, and this is one of them, where trying to do in less than an optimal manner just creates a whole new set of aesthetic problems.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My head is flat on the back and underdeveloped on sagittal and frontal, and it’s been troubling me and cause I h me depression just being aware of it 24/7. I got a few questions about the procedure. 1. Is it bone cement you’ll be using for skull reshaping surgery, or silicone padding? 2. Is possible to go through one anesthesia and have three incisions and reshaping my forehead, back of my head and my sagittal area in one procedure? 3. I’m 21 this October and I’m a trans women, but I am international. Does skull reshaping surgery count as part of my Facial Feminization surgery, and if so could that be covered by insurance? 4. What are the expenses, risks and possible problems of this procedure with my condition?
A: Although I do not have a full understanding yet of your skull reshaping needs (a description along doesn’t tell me exactly what needs to be done) but in answer to your questions:
1) Custom solid skull implants are far superior than the use of bone cements in aesthetic akull augmentations.
2) Multiple area skull reshaping procedures can be done in a single surgery through multiple smaller scal incisions as opposed one large bicoronal scalp incision.
3) I do not participate in any medical insurance programs.
4) To provide an accurate cost of your skull reshaping surgery I would need to fully understand the procedures needed. This can be done by an assessment of some pictiures of your head.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I had a breast reduction two years ago, I am concerned about my nipples are not erected, look flatter, inverted. I think my surgeon did a nipple graft. I want to know of this can be corrected.
A: If you had a free nipple graft type breast reduction then the nipple will have no sensation or ability to become erect. It will also lack projection and appear more flat. These new features of the nipple can not be changed.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have two divets in my jawline, one on each side, not too far from my jaw angle. These are from a mandibular osteotomy done in the 90s. Can these divets be filled in somehow? I have looked into dermal fillers online; the area seems to be a sensitive one so I’m a little apprehensive about that. I’m attaching a picture of my right jawline. Unfortunately, you can barely see the divet here, but it really impacts the smooth line of my jaw. I’m a transitioning transwoman and I’d like to have a nice smooth jawline. Thank you
A: These are classic jaw angle/antegonial notch deformities from mandibular osteotomy surgery. They are best reconstructed by an implant which is ideally done using a custom design approach since they are undoubtably asymmetric in shape. Short of this ideal approach there are standard vertical lengthening jaw angle implants which can be used but applying standard shape implants to a noin-standard shape problems has its own disadvantages. (asymmetry)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, can I get scalp augmentation for a height increase?
A: At best skull implants can raise one’s height by 2.5cm to 3cms which often requires a two stage approach. With the immediate insertion of a skull implant (one stage approach) the height increase is limited to 15mms.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I recently got a ‘skull implant’ and they used a material called PMMA. After getting the procedure done i am unhappy with the stiffness of the material. If i lay down and put my fist at the back of my head is leaves an imprint and overall PMMA leaving imprints when i press hard on my skull is something Line Surgery never told me. Is it possible to remove the bone cement and then add a silicone implant, and is the silicone implant squishy like the bone cement ? i want an implant that isn’t squishy , thanks.
A: You have an ‘old style’ skull augmentation using PMMA bone cement. One of the known problems in using PMMA, and there are many, is that it is almost impossible to get it smooth or avoid implant edging which can often be sharp. This is probably the source of your symptoms and not the hardness of the material per se since is not much harder than your natural skull bone.
Solid silicone skull implants, in which I have placed over 500 of them, have never had any of the current problems in which you describe.They are solid silicone implant not like gel-filled silicone breast implants.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, do you have any before and after pictures of the brow ridge implants?
A: There are many brow bone implant designs and actual examples of brow bone implants on the following sites: www.exploreplasticsurgery.com and www.eppleycustomfacialimplants.com.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, i lost my left testicle when i was three years old. At the age of 38 i decided to implant a testicular protesis, but with the result i am very unsatisfied. The protesis is to small and very hard, so the feeling is very unnatural. My natural right testicle is about 6cm long and 4,2 cm wide.
I am looking a long time for a prothesis with enough size so it fits better to my natural testicle. On your Home page i found a solution: “Solid Silicone Testicle Implants”.
I want to know, is it possible to buy this prothesis, so my german doctor can implant it? Or is it nessecary to travel to you to replace it? How much are approximately the costs?
Thanks for your reply.
A: I am not a manufacturer/seller of implants. I only make custom testicle implants for patients in which I do the implantation.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My primary concern in pursuing shoulder narrowing surgery is that I do manual labor for a living and am worried about losing my range of motion as a result of this surgery. I’ve done research into successfully healed double-clavicle fractures where range of motion is maintained, which makes me feel better. Ultimately I’m at a point where some loss of range of motion would be acceptable in exchange for noticeable results.
A: Your concerns are understandable and common but in my experience to date I have yet to see any postoperative range of motion issues after surgery. Nor would I expect such to occur given the much larger clinical experiences in non-surgical and surgical clavicle fracture repair. (not an exact corollary but close)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve had a lip lift about 4 weeks and even though the distance between muse and mouth is still almost as before the nostrils have been made wider and the base distorted
Will this improve in time or is thus the final result? I’ve added before and after photos
If this is the final result can a plastic surgeon narrow my nostrils to their original size and shape easily and if yes after how many months?
I’m very depressed as I had a beautiful nose by birth and now my whole face seems different and the nose too big for my face!
A: This is undoubtably at 4 weeks the final result as it related to the width of the nostrils…more healing time is not going to make them more narrow. A secondary nostrill narrowing proceduer can be done 3 months after the lip lift surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have infraorbital rim implants already and am currently planning for double jaw surgery to correct bimax recession (I’ll be having lefort 1 and BSSO with counter clockwise rotation).
Is it ok that I have infraorbital implants so far as getting this surgery done? When I’ve seen diagrams for lefort 1 procedures, the screws and plates do extend up into the cheek area (though I don’t think they go quite as far as the orbital rim, but it seems in close proximity). I’m worried when I consult, the surgeons may tell me they need to remove the implants because they are in the way of where they need to secure the plates. However, I have seen that there are multiple variations in the sorts of plates used, with some that do not extend around this area.
A: With the use of standard infraorbital rim implants I don’t see any problem with the performance of a LeFort I osteotomy or the fixation needed to secure it.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, It indeed is possible to remove the existing silicone chin implant, perform sliding genioplasty (should there be a need to that, of course) AND insert a wraparound jaw implant (that would cover the chin too) in the same surgical procedure…(?). if so, wouldn´t that place too much strain on the chin, as it would take the biggest brunt of the surgery (implant removal, genioplasty + new implant)?
- If I gather correctly, wraparound implant can elongate the lower third of the face in the manner ChinWing can…(?).
- As for the fat along my jawline, it´s been almost a decade it has been injected, but it is still very much present and does mimic a facial implant to a degree (ca. 7ml of fat on each side) which is of concern to me for it may interfere with how the final result would look like. Hence my question: could that fat be take out – at least partially – either in a separate session under local anesthesia a few days before the main surgery, or under the same surgery…?
- Finally: silicone or peek custom implants? Which are preferable in terms of patient safety, avoidance of (delayed) infection, aesthetics and easiness of placement on the jawbone…?
A: In answer to your questions:
1) Removing a chin implant, replacing it with a sliding genioplasty and simultaneously placing a wrap around jawline implant does not place excessive strain on the chin. I have done it many times.
2) A custom jawline implant elongates the lower jawline more effectively than a chin wing osteotomy.
3) Once fat is injected in the face it is very difficult to remove. Attempts to do so would require a microcannula liposuction approach done months before the definitive jaw augmentation procedure.
4) A solid silicone jaw implant offers the easiest insertion/placement and eae of revision or reversibility.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I had a genioplasty of 6mm advancement 4 months ago and I still want to get it reversed. Is a full reversal too risky? Will it cause too much skin sagging. I am 19 years old and my first surgery was actually a success except the fact that I don’t like the results. The 3 first pictures here are the post-op 4 months later. Thank you for you answer!
A: I think the risk of any skin sagging with a 6mm sliding genioplasty reversal is fairly low. Skin sagging is more likely to occur from chin implant removal than a sliding genioplasty.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a rather prominent zygomatic arch, it doesn’t really bother me or anything, but what really bothers me is the fact that my front part of the skull is quite narrow compared to the proportion of the zygomatic arch protuberance, which makes my face have kind of unevenly shaped, by starting wider and progressively narrowing as it goes, forming an irregular oval face, so my question is:
It is possible, through a cranioplasty intervention, to widen my cranial frontal laterals, in order to straighten the sides and muffle the protuberance of the zygomatic arch, following the same width or so, nothing too exaggerated of course, but making the change.
I uploaded 2 photo references of what I am trying to look after.

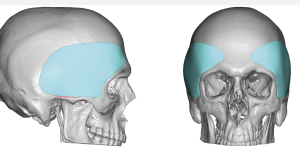 A: You are specifically referring to a family of head widening implants that I commonly perform that run the spectrum of standard anterior temporal implants to custom extended temporal head widening implants. (see attached implant designs) Based on your pictures and description of aesthetic needs it would probably be very similar to the anterior head widening implant design in the 3 to 4mm range of maximal thickness.
A: You are specifically referring to a family of head widening implants that I commonly perform that run the spectrum of standard anterior temporal implants to custom extended temporal head widening implants. (see attached implant designs) Based on your pictures and description of aesthetic needs it would probably be very similar to the anterior head widening implant design in the 3 to 4mm range of maximal thickness.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve been researching plastic surgery for the past couple of months and I’m considering getting several facial procedures done. Recently my eye was caught by clavicle lengthening. My narrow shoulders have been pointed out to me for as long as I can remember and have solidified themselves as a pretty big insecurity. I am 6′ tall with a shoulder width of 16-16.5″ bone to bone. In theory, it sounds amazing, but I have a couple of questions. Would I be able to reach a width of 18″? It’s a bit of an arbitrary number, but I feel like I’d be content with less , as long as I look more proportionate. Since a V-Taper is sought after in bodybuilding, could shoulder widening make it more pronounced? With the shoulder being formed by the clavicle and scapula, how does clavicle lengthening affect the scapula? Does it get pulled alongside the clavicle and could it look unnatural if it’s lengthened too much? Is the clavicles strength permanently compromised after the surgery?
A: These are all great questions in regards to the shoulder lengthening by clavicular expansion osteotomies to which I can say the following:
1) The average in shoulder width by lengthening osteotomies is about 1 ¼ to 1/1/2 inch collectively. (both sides) So going from 16 inchs to 18 inches is not going to occur from the surgery.
2) I think the primary effect of shoulder lengthening is that it makes the shoulders more square in appearance. That effect is more obvious than being wider.
3) Shoulder lengthenng is ultimately restricted by the scapula and its soft tissue attachments. Thus teh scapula is not lengthened or changed in position of any significance. It is the reason that shoulder lengthening can be more than it is.
4) Once fully healed the bone strength should be normal biut that takes a while to get there. (up to 6 months) Of course of one never removes the fixation plate the combined plate-bone unit is more resistant to fracture than the natural bone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon