Your Questions
Your Questions
Q: Dr. Eppley, I know it has been a long time since I have reached out with any comments about my implants I had gotten done with Dr. Eppley, and there are no complaints or issues whatsoever. Everything is stabled and seems to have been well integrated.
My only question for Dr. Eppley would be about the possibility of contact sports such as wrestling? Would there be any issue with involving myself in sports such as that regarding my implants or should I be fine to proceed?
Thank you very much and hope everyone is doing well!
 A: Good to hear from you after a few years from your custom periorbital facial implant surgery. You should have no problems with participating in all sports including wrestling. Your facial implants are well healed at this point and should never be able to be dislodged or displaced short of extreme external trauma of which sporting activities does not fall into that description.
A: Good to hear from you after a few years from your custom periorbital facial implant surgery. You should have no problems with participating in all sports including wrestling. Your facial implants are well healed at this point and should never be able to be dislodged or displaced short of extreme external trauma of which sporting activities does not fall into that description.
I wish you continued success and happiness as you continue on your upward trajectory in life.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My right eye brow has uneven bone little bit prominent could you please help me correct it.
A:For brow bone asymmetry due to a greater prominent on one side this is often a reflection of an overgrown frontal sinus on one side. The key question is whether its reduction can be done by burring or a bone flap setback, usually it is the latter that is needed. But I would have to see some pictures to determine its level of prominence.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I sent a few photos that you analyzed and you indicated that one side of the face droops lower than the other. Can this be corrected by a face lift or any other measures.
A:It is not that one side of the face droops, it is that one side of the face is structurally lower than the other side. Drooping is a soft tissue problem while structural asymmetry is a bone problem. Thus a facelift will not be effective.
In facial asymmetry the first and most important question when considering what can be done is what areas bother the patient the most? What do you see that brought your attention to the asymmetry? Facial asymmetries are complete (top to bottom) but not all areas of asymmetry can be effectively corrected, some have better value in doing than others. Thus the need to prioritize the area(s) from which then I can tell you what can or can not be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about two stage skull augmentation:
1. How do the scalp expanders work?
2. Does it hurt to have them?
3. How long do they last until permanent implant?
4. Can the scalp expanders be placed anywhere on the skull?
5. Will the scalp expanders alter the appearance of the face(eyes) if used to widen skull? (Not wanting to stretch face)
6. Before any implant is put inside head can I have blueprints of the implant(s) so I can 3d print them and test the look of the implant on my skull?
7. I genuinely believe I look better with a wider skull and have pictures to prove my belief. I add volume to my hair and have been sculpting it for a decade in a way to achieve the desired look of my skull. I want to have as much widening of my skull possible so that’s why I inquire about the scalp expansion.
I would like to discuss in more detail the desired look I would like to achieve with Dr Eppley before any implant models are made. I have pictures if that is necessary. I can also video chat with him again to show him in person if that’s better for him.
A:In answer to your two stage skull augmentation questions:
1) Scalp expanders work like pregnancy….an internal slow pressure on the overlying skin to ultimately allow for a bigger mass underneath it.
2) Beyond their initial surgical placement, no.
3) The usual time period for scalp expansion is between 6 and 12 weeks before the permanent implant is placed depending upon how much scalp expansion is needed. (which is based on the size of the custom skull implant)
4) Yes
5) Unless the scalp expander is placed in the forehead it will not alter the appearance of the face.
6) You are referring to the .STL files of the implant designs. They are available from the manufacturer once the final implant design is completed but not during the various stages of the implant design. Setting an implant model on your head is not all that helpful as it will not sit properly as it is placed on the outside of the scalp as opposed to under the scalp where it will actually reside. Thus it is not a very accurate representation of the final aesthetic result.
7) Many skull augmentation patients, if they have hair, have long demonstrated the benefits of a larger skull base through hair manipulations. Thus I don’t question any patient’s aesthetic desires. I am only focused on what can I achieve in the safest and most effective surgical process. I think in your case for added head width the key question is whether one needs a one vs two stage skull augmentation approach. The best way to figure that out is imaging of your pictures to show the different potential outcomes between the two approaches.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about otoplasty reversal. Before meeting you, I consulted another doctor experienced in reversal otoplasty who suggested using a tissue-banked rib graft. After consulting with you, I returned to this doctor for a second opinion, and here is what he said:
“Alloderm is a very soft material that has no rigidity at all. You have to use something that can resist the body’s desire to pull the ears back inward. Only stiff rib cartilage will do this – or use of a goretex implant. Alloderm will not provide sufficient structural support and/or resistance.”
I apologize for any inconvenience caused; I’m simply trying to make the best decision to avoid a third surgery. Could you please discuss this and give me your thoughts on the other doctor’s opinion?
A:Normally that would be a correct statement if the goal was to drive out the entire concha/ear framework for the reversal and it was being placed down on top of the mastoid bone to serve as a stiff strut. Thus a very stiff material is needed and cadaveric rib cartilage would be what I would use. But your ortoplasty reversal case is different in terms of the magnitude of the goals and the location of the interpositional graft to try and achieve them. You need a slight correction of the helical rim, mainly on one side AND you don’t want a stiffer feeling ear. Thus in your uncommon otoplasty reversal I would not use rib cartilage in the traditional manner. A roll of Alloderm placed just behind the helical rim will make it come out a few millimeters and has no chance to make the ear feel stiffer.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a consultation with another doctor who also does facial implants. He told me that I have a flat jaw and that through the x ray he can improve on this and I think make it sharper, not sure…..Can you do this too?
Heres a pic I just took now. I think he looked at the xray and the jawline went straight but then there was a disconnect. He said he could perform surgery for this. Can you do this?
I want this in addition to the facial implants
Side note: I have holes in my skull following browbone ffs shaving. Can a facial implant be used to cover this? Thanks.
Also I was considering an implant on my head as my head at the back is flat thanks a lot!!
A:The question is not whether you can have a change in your jaw shape or whether that is best done with a custom jaw implant (from a 3D CT scan) as those type of procedures I do every day…but what type of change are you seeking that looks better to you. Thus the firsr step in any form of facial structural change is to do some computer imaging to determine the patient’s aesthetic goals. To begin that determination I have attached some initial imaging. (although be aware that in such assessments all three facial angles must be considered, not just the side view.
Holes in the bone after a brow bone flap setback are defects into the frontal sinus. Implants are generally not appropriate for covering them since they are exposed to the sinus cavity in which the risk of infection exist. The more appropriate coverage material is hydroxyapatite bone cement to fill them and smooth over the bone.
A custom jawline can be done with a custom skull implant during the same surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,What would the estimated cost to remove this occipital protuberance from the back of my head? I’m growing my hair out more these days but I’ve always been self conscious about it and it is still very visible. Also, is there anyone who can do this procedure closer to Texas?
A:This appears to be an occipital knob although a side view picture would be more revealing of it. I would have no knowledge of whom, if anyone, does this surgery in Texas…but I know how to find out. Put the search term Occipital Knob Skull Reduction in Dr. Google and see what comes up. Otherwise I will have my staff contact you later today to pass along the cost of the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a question regarding my two stage skull augmentation procedures. Let’s say I later wanted to have a larger implant, would it be possible to change the implant?
I’m sure I’ll come back to you later for more volume.
A:I believe you are asking if one gets a 275cc skull implant can they come back later for an even larger one, like 350cc or 375ccs, and that answer would be yes. (one year ore more later) The first implant acts as its own tissue expander to go beyond what the first actual tissue expander accomplished.
Dr. Barry Eppley
World-Renowned Plastic Surgeo
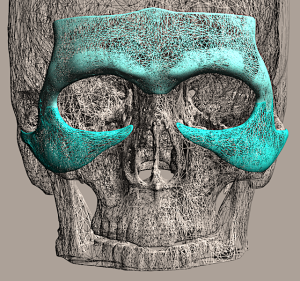
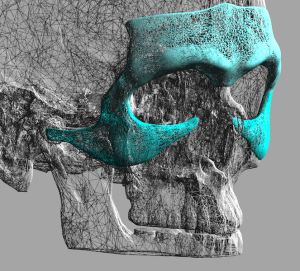
Q: Dr. Eppley, I was wondering about a reduction of dark circles and under eye hollowing. I am desiring a more uninterrupted eye cheek junction. I am wondering if a custom malar infraorbital rim implant would have an anti aging effect on my face. A:Custom infraorbital implants (not standard infraorbital implants as they don’t saddle the rim) are most effective at improving undereye hollows which is a volume problem. Dark circles may or may not be significantly improved as their cause is not just a volume problem. Any shadowing that occurs from lack of infraorbital rim projection that contributes to the dark circles will be improved. But if hyperpigmentation is a significant cause of the dark circles it may have no to minimal improvement.
In other implants correct bony deficiencies (hollowing) and overlying soft tissue contours (dark areas by shadowing) by their push out on the overlying soft tissue. They can not change excessive pigment in the tissues.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I’d like to know more about your services. I have a flat head and I know there are different ways to correct it.
A:here is only one definitive method for augmenting the back of the head, a custom skull implant, in which the amount of augmentation is controlled by the stretch of the overlying scalp to accommodate it. (see attached Imaging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have included additional photos to determine if only the hairline advancement procedure would be beneficial in my case and I would not need the frontal bossing reduction as well. I have drawn two distances on my forehead. Ideally, I am looking to move my hairline forward so it reduces or eliminates to top of my head for being bare.
A:What these pictures clearly show is that the amount of frontal hairline advancement is 3 cms. (30mm+) That amount of hairline movement means two things:
1) It would require a first stage scalp expander. (1.5cms or half of what you have shown is possible without it…and even that may be a stretch)
2) If you can truly get a 3 cm hairline advancement the need for the frontal bossing reduction will be reduced and/or eliminated.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I came across some of your answers regarding the modified subcranial 180 degree orbital osteotomy used to widen the eye distance by 3-4mm. My question about this is it possible to move the eye lower using this technique as well? To correct orbital/eye asymmetry if one eye is higher than the other and only 3-4mm of down move is needed. Thank you!
Q:You are referring to orbital decompression (lowering of the eye) which could be done at the same time as inferior orbital box osteotomies.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Interested in a consultation for JAW IMPLANT. I already have a chin implant from a previous 2016 surgery.
A:Many custom jawline implant patients have a prior history of a chin implant. The question is not whether the conversion to a full jaw augmentation can be done but what type of lower facial change are you seeking. To begin that visual discussion of your jaw augmentation goals I would need three pictures to do that initial imaging. (non-smiling front, side and ¾ views)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would be open to discussing the wrap around jawline implant further. Is it possible to see the impact of this on the front profile?
A:You are probably not properly interpreting what the role of facial imaging is. It is NOT done to show what you are going to looking like as no one can predict that with certainty. Rather it is done for two purposes: 1) to help the patient make a choice between different procedures if such options exist (which in your case they do….jaw angle augmentation alone vs total jaw augmentation) and 2) based on that choice what flavor of change do they want of their chosen procedure. For jawline augmentation the side and oblique views provide the best way to determine #1.
In other words imaging is done to help the patient make procedure choices and then use the imaging to determine what their goals are from which the surgery is designed to try and accomplish…which may or may not hit those imaged targets exactly.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I have cheek asymmetry after a cheekbone reduction fracture repair and I assume it is due to how the fracture was repaired.
 A:I have reviewed your 3D CT scan which shows the cheek asymmetry between the two sides. (see attached) While the left ZMC fracture repair was decent it is underrotated a bit back out (not uncommon) hence the bony asymmetry. The inferior plate can be seen to be detached from the maxillary bone which is probably why it didn’t hold up as this is the buttress to get optimal rotation. That issue aside the bony asymmetry is most ideally addressed by a custom overlay implant to optimize the projection of the left cheek bone to the other side.
A:I have reviewed your 3D CT scan which shows the cheek asymmetry between the two sides. (see attached) While the left ZMC fracture repair was decent it is underrotated a bit back out (not uncommon) hence the bony asymmetry. The inferior plate can be seen to be detached from the maxillary bone which is probably why it didn’t hold up as this is the buttress to get optimal rotation. That issue aside the bony asymmetry is most ideally addressed by a custom overlay implant to optimize the projection of the left cheek bone to the other side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How can I reduce this ridge in the top of my head? Do I need sagittal crest reduction. I have attached my skull CT scan for you to review.

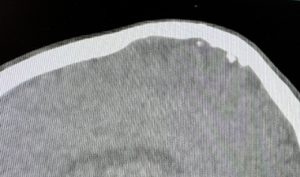 A:I have reviewed your CT scan which has been enormously in determining both the origin of your sagittal crest, its thickness and surgical possibilities for its reduction/improvement. In looking at your head shape and the scan your proper diagnosis is a PSEUDO SAGITTAL CREST which means it llooks like a sagittal crest but it not a true sagittal crest. This means it appears because the skull around it is lower/deficient which makes it just look like there is a sagittal crest but there really isn’t. This is evident by the following:
A:I have reviewed your CT scan which has been enormously in determining both the origin of your sagittal crest, its thickness and surgical possibilities for its reduction/improvement. In looking at your head shape and the scan your proper diagnosis is a PSEUDO SAGITTAL CREST which means it llooks like a sagittal crest but it not a true sagittal crest. This means it appears because the skull around it is lower/deficient which makes it just look like there is a sagittal crest but there really isn’t. This is evident by the following:
1) A true sagittal crest is when the bone is thicker than the surrounding skull bone. not thinner. Your scan shows that the crest is thinner than the surrounding, which beyond making the proper diagnosis also indicates a full reduction of it is not possible/safe. (see attached imaging) This does nort mean some reduction is not possible just that a complete reduction can not be done.
2) Technically it is the surrounding skull (parasagittal-parietal skull) that is deficient or too low and building up the bone around the crest creates the better head shape result and fully eliminates the crest appearance. (see attached imaging)
3) In short what we have learned from the scan is that the sagittal crest can be directly reduced but its appearance can not be fully eliminated. Full elimination is possible with an overall better head shape but requires a different procedure. (custom skull implant) The choice comes down to how much improvement does one want and with what amount of effort does one want to put into it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I discovered Dr Eppley after I was diagnosed with midface hypoplasia due to receiving cranial radiotherapy by mistake when I had Leukaemia aged 5. I did have a malocclusion Class III but that was corrected with upper jaw surgery. Under our health system in the UK the plan was to treat the remainder of my midface hypoplasia with implants, as well as a mid facelift, but the care I have received here has been very poor in achieving that so I am not looking elsewhere. I should also add I am not entirely sure how honest the government health system has been about the degree of my facial deformity so even to know that in Dr Eppley’s professional opinion would be most valuable.
A: Thank you for sending your pictures and 3D CT scan. Having had a LeFort I osteotomy you have maximized the forward lower midface advancement with conventional osteotomies. By your external appearance you would certainly be a good candidate for a custom midface mask implant. The only cautionary caveat is the prior history of radiation which increases the risk of complications with an implant. Whether that risk is minimal or of some significance is not known and having had radiation decade ago does not lower that risk. The adverse effects of radiation do not change with time.
With an implant in a field of prior radiation there are two approaches. One approach is to just place the implant and see what happens. This would be a reasonable approach if the risk of complications was known to be minimal. The other approach is to pretreat the midface tissues with fat injections to improve the vascular quality of the soft tissues. This would be the approach of the risk of complications was known to be moderate or even high.
The dilemma is, of course, that no one knows what your risks are from prior radiation. And there is no test to make that determination. The only preoperative ‘suggestion’ is that youm healed satisfactorily from a LeFort osteotomy…although this is an autologoous proceduer and not an implant-based one.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m experiencing complications following DJS and genioplasty – specifically extreme tightness in my chin at rest (gets worse when smiling or talking) my lower lip is curled in and the outside corners are being pulled down, new lip incompetence (did not have prior to surgery) I’m exploring genioplasty revision options but I’m concerned that reversing the forward movement of the chin might contribute to more lip incompetence since there was CCW movement in the maxilla. I’ve included my before and after planning images. The maxilla was advanced 3mm forward and CCW rotation, the lower jaw BSSO forward movement was 7mm, and the genioplasty was another 6mm. I am very petite and I’m concerned that these movements were too aggressive. I can hardly sleep with the tightness constantly pulling on my chin and the mouth breathing issue is also constantly disrupting my sleep.
A: The bony movements alone do not explain your symptoms. The amount of forward chin movement (6mms) is not excessive even when combined with a mandibular advancement….at least by the numbers. How it looks aesthetically I can not say as you have provided no before and afters to evaluate.
This sounds more like intraoral chin scar contracture of which its treatment would be either a subtotal genioplasty reversal, an intraoral scar release and dermal-fat graft or a combination.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in speaking to someone regarding front bossing procedure and forehead lowering.
A: Thank you for your inquiry and sending your pictures. The combination of a high (long) forehead and frontal bossing are aesthetically synergestic….and not in a beneficial way. A long forehead can make the bone appear more protruding while frontal bossing makes the forehead look longer.
While optimal results in forehead reshaping comes from a combination frontal hairline advancement and bony forehead reduction, they usually do not provide an equal amount of contribution to an improved shape. In many cases, and yours is a good example, the hairline advancement provides the most benefit.
Thus gettng a maximal hairline advancement is critical and, while I would want to see where you want your frontal hairline to be, it is likely it is a least 2 cms forward. But before making that presumption I need to see your frontal hairline goals by drawing on your forehead your desred new hairline location. This is critical information as it can affect how the hairline advancement is done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello. I am a transgender woman from England. i previously have had two jaw surgery and also mandible shaving as part of a few facial feminization procedures however they removed too much bone so i have a very weak mandible angle. would you be able to tell me if you do custom jaw implants? and how much roughly do they cost?
My issue is i have previously had jaw shaving v line but they removed too much bone so now i have very asymmetric weak mandible.
A: I have done many custom jaw angle and jawline implants for subtotal or total V line surgery reversals. Over resection in Non-Asian patients is not uncommon as the size and shape of the Caucasian lower jaw is often different.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello! I want to have rib removal for a smaller waist & I’ve previously enquired about shoulder narrowing surgery. I am set on having 2.5cm removed on each side. As for rib removal, I have a couple of questions. Would it be possible to remove both the 11th & 12th ribs during the same surgery? If so, would it also be possible to have the rib removal & shoulder reduction both during the same surgery? How much would it cost in total? Thank you so much & have a great day.
A: It is common to perform bilateral 11 and 12 rib removals at one time as well as combine that procedure with clavicle reduction osteotomies. Almost always 2.5cms of clavicle bone is removed per side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I would like to inquire about a consultation for chin ptosis treatment. It’s congenital, I’ve had it all my life and never had any facial surgery. I tried Botox for the first time a couple weeks ago for it and I feel like it made it even worse.
A: I am not confident that congenital chin ptosis in its entirely can be improved…at least the lower lip position can probably not be improved. The overhanging chin pad and the deep siubmental crease can be improved by excision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, 1. Would any cosmetic skin treatments like microneedling or Fraxel laser therapy pose a risk to my implants? (in particular the malar implants but also the chin or jaw implants)
2. Have you ever heard of apthous ulcers causing jaw hardware infection? I am taking rapamycin for longevity benefit, and this drug causes occasional canker sores. I want to make sure that I don’t put my jaw hardware at risk, and would stop the rapamycin if you thought there was a significant risk that a canker sore could lead to a hardware infection.
A: In answer to your questions:
1) Facial implants are not at risk from any ‘invasive’ skin treatments such as microneedling or laser resurfacing.
2) Apthous ulcers are a superficial mucosal (wet or dry) eruption that is far removed from the subperiosteal location of your facial implants. There is no infectivity risks to your implants from them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it safe for someone to get Botox if they are allergic to cow’s milk, Casein & or egg?
A: Botox is a synthetically derived toxin in which its production does involve albumin, a cow’s mild protein. So if one has a true albumin allergy then one should not get Botox. However a lactose intolerance does not count as an albumin allergy.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, you did my breast augmentation back in February of 2017. I have had a wonderful experience so far! I am simply curious when or what I need to do to “check” to make sure they are good. I know it’s usually 10 years it is requested to get new ones, but can go longer. Just seeing if I should be planning for something in the coming years.
A: Good to hear from you after all these years. With silicone breast implants there is no reason to ever replace them unless they fail. (disruption of the containment shell known historically as a ‘rupture’) Unless you have implant symptoms (pain, change in breast shape) you just get your mammograms as you normally would do on that schedule which will also show implant integrity There is no need to replace them every ten years unless there is a compelling reason to do so as per above.
Short of any symptoms of implant failure you may live with them for many decades or even the rest of your life.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to ask you if there would be a change in volume compared to the extension, that is to say will there be more volume once the implant is placed? Or will the change not be very different compared to the scalp extension volume?
A: While a scalp expander and the skull implant may have similar volumes they have radically different shapes. Scalp expanders are round while the skull implant has a more oblong skull shape as you have seen in the design file. So don’t confuse the external effects of these two.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I hope you’re doing well. I have a lip deformity that developed after I underwent double jaw surgery and genioplasty almost a year and a half ago.
At rest, my lips don’t meet naturally and I need to force my lips closed since my bottom lip drags down and rolls outwards which exposes the wet mucosa. Forcing my lips closed causes me pain in my lower lip and chin area.
I’m thinking if I somehow can permanently augment my upper lip it will close the gap I need to force shut therefore reducing my pain. I’m interested to see what the doctor would recommend.
A: i think you have had too many alterations in the perioral region (subnasal lip lift, double jaw surgery, genioplasty) that the structure and elasticity of the lips has been adversely and probably permanently affected. The key for your lip incompetence is not to try and make the upper lip go down to meet the lower lip….as that will never happen and the upper lip already covers all of your upper teeth. The correct diagnosis for your lip incompetence is that the lower lip is pulled down as the excessive lower tooth show demonstrates. Therefore the correct approach, challenging as it is, is to free up the lower lip and try and raise up it higher up. In my experience the only effective approach is vestibular/scar tissue release, dermal-fat graft and a shortening vestibuloplasty.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My son is 6 years old has brachycephaly. At what age can this procedure be done?
A: 16 years of age is the minimum age with parental consent.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in midface and cheekbone implant but am not sure if I can afford it. I was wondering the range of cost of the procedure?
A: There are two strategies to midface augmentation in the Asian patient, standard cheek (modified for anterior cheek/infraorbital augmentation) and paranasal-premaxillary implants and a custom midface mask implant. The former is what is done when the patient’s budget prohibits the latter.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to ask if you are able to conduct buccal fat rejuvenation surgery.In a previous facial surgery,I had removed about 50% of my buccal fat and I would like to see if it’s possible to restore some of this fat in my cheeks. If there is any information you can provide it is much appreciated, thank you.
A: There are two autologous methods for buccal fat restoration or reversal, external fat injections and intraoral replacement with a solid fat graft. There are advantages and disadvantages with either approach. Fat injections are a scarless harvest and placement but their survival is not completely predictable. The solid fat graft method requires a donor site but the volume of the graft is more stable/predictable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon