Your Questions
Your Questions
Q: Dr. Eppley, Usually, when smiling, the blue line in the image is very short and the lips appear to be in approximately the same position. However, since I am Class II, my chin is receding and the blue line is longer. Would this be possible to try genioplasty, labiomental sulcus filler, etc. to shorten the blue line even a little?
A: No form of chin surgery can change the position of the lower lip, either at rest or in dynamic motion.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, have a bone spur,or piece of bone sticking out the back of my head it causes headaches , it hurt, and it stings been dealing with this most my life , and I never new there’s a alternative for this.
A: The spur on the back of the head to which you refer is known as an occipital knob and can have a sharp edge to it. While usually asymptomatic it can occasionally be a source of chronic discomfort. It can be removed in a straightforward surgical procedure done as an outpatient.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I need some advice from someone experienced with chin implants. I have had two failed surgeries in 7 months. Now I need a third one. I prefer if that is the last one.
I have been looking at Implantech for the third surgery. The one my norwegian doctor used is sebbin:
My face was “long enough” as it was. I didn’t want any downward projection of the chin implant. I wanted forward projection. As Dr Eppley will see from the CT scans. Its the opposite of what I am after. Now its a lot of downward projection. An not much forward. This is due to the wrong placement downward and also that it has be sinking down after surgery as well. I prefer not below my own original chin at all if that is possible. Which implant would be best for me is the quest here.
My surgeon for the first two surgeries would be very happy to join med on a call
A: As your scan clearly shows this is an implant placement problem not an implant style-size problem. It doesn’t matter what the chin implant is if it can not be placed properly.
I do not talk to surgeons to teach them how to handle their complications, that is not my responsibility nor what I am willing to do.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My right eye brow bone is getting a little larger than normal I feel like the bone has grown a little and I feel pressure between my eye brows all the time so if there is a doctor or a way to help this would be a lot.
A: You should have a 3D CT scan to evaluate the fractured brow bone area to see if it is really bone overgrowth or just scar tissue/nerve injury.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a couple questions about my eye area:
1. The first two pictures show my current eye area completely relaxed. Do I have ptosis of the upper or lower eyelid? If not, would ptosis surgery or any other procedure work to lift my lower or upper eyelids a bit?
2. One of my desired outcomes is moving the inner corners of my eyes a couple millimeters inward, as shown in picture 3 as a slight morph of the second picture. I notice I get this result when I pull very slightly with my fingers inward, and the eyelids still remain attached to the eyeball. This makes me think I have loose skin or medial canthal tendons. I have seen mixed opinions online, and you stated in a post that this would be difficult to achieve without risking scarring. Suppose we didn’t really care about scarring. I have seen procedures designed to achieve this effect, such as C-U plasty (picture 4), which cuts the medial canthal tendon and moves one end inward, as shown in picture 6, and W-V plasty, which simply removes some skin to tighten the area. These generally are designed to correct telecanthus. Would one of these procedures, or any other ones that tighten skin or the tendons, realistically work for my case?
A:In answer to your eye reshaping questions:
1)Do you have true ptosis….not really. Maybe a 1mm. But one does not have to have true ptosis to have ptosis (upper lid elevation) surgery.
2) Lengthening the inner eye corner towards the nose is not done by any medial canthal tendon surgery or any of the procedural diagrams which you shown. (those are for webbing/hypertelorism surgeries) It is done by a tissue rearrangement technique known as a Y-V lengthening surgery. This has more favorable scar formation than its cousin, V-Y narrowing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to get the rib removal done, I’m wondering if I’m a good candidate and if I’d be one of those patients that would have a dramatic difference or subtle difference. I’ve looked into getting a BBL but I’m hoping maybe a rib removal will slim my waist enough where I wouldn’t care to enlarge my hips. My waist currently is about 25in and my hips are about 33/34. I would like my waist to go down closer to a 21/22 so wondering if that’s possible with my anatomy.
A:Thank you for your inquiry and sending your pictures. Your question is a good one in that with your body type (tall and thin but with a vertically long buttocks) you could go either direction of a BBL or rib removal. I don’t think either one is a bad choice. Whether rib removal results are subtle or dramatic is open to personal interpretation. But what I can say is the following: 1) Dio I think your waistline results will drop from 25″ to 21″… no (tall and thin patients do get the best results but that would be expected too much in my experience) and 2) an expected change in your waistline shape I have shown in the attached image prediction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 42yo Male to Female Transgender Person. Im intrested in your Scrotoplasty. Do you also offer Orchiectomy Surgery ? As atm im using Androcur as a Testosteron Blocker.
A:Testicle removal can be done with scrotoplasty although if the eventual goal is to have SRS (sexual reassignment surgery) then this procedure would be unnecessary. The transfemale that may be considering such a scrotoplasty usually is not progressing onward to SRS.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My head big size 61 sm. Can it be reduced?
A: The question is not whether it can be reduced but whether it can be done enough to justify your efforts and goal. In reality skull reduction is best suited for spot area reductions rather than a major overall head size reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello. I have a flat spot located at the parietal area. It is very noticeable to my hairstylists and although it also is not appealing cosmetically I would like to get this looked at by someone as I believe it could be a cause of my migraines. Does your office have the ability to a virtual approx. 30 minute free consultation via Zoom meeting? Is it possible for my severe flat spot on my head to be causing migraines?
A:I am not aware of any association between a flat spot in the skull and migraines. Augmentation of such areas is done for cosmetic purposes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had orthognathic surgery in April to correct jaw misalignment and a pretty serious overbite. I now have hollowness in my midface and some asymmetry of soft tissue between my left and right side of my face, and I am looking to get opinions on which midface implants would be the best option for me.
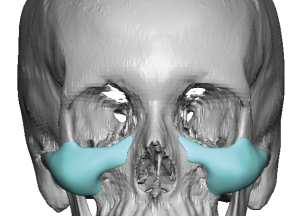
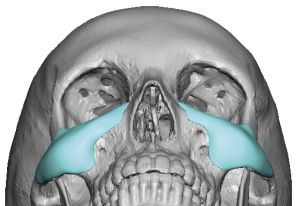 A:This is a pretty common sequelae post LeFort I, particularly if one had some infraorbital-malar deficiency to start. This is treated in many such cases by a custom infraorbital-malar implant design as per the attached images.
A:This is a pretty common sequelae post LeFort I, particularly if one had some infraorbital-malar deficiency to start. This is treated in many such cases by a custom infraorbital-malar implant design as per the attached images.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How safe is the rib removal surgery? I’d it safe to have those ribs removed and gone?
A: Despite its name and misconceptions about the surgery. it is a very safe procedure in experienced hands and very few complications or side effects. (an occasional self-resolving seroma is the only ‘complication’ I have ever seen. It is far fewer side effects and risks compared to more well known body contouring procedures such as tummy tucks and BBL surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to tell just based on the photos I sent earlier alongside these pics of my design if the implant can be totally camouflaged with those techniques as well as perhaps with a midface lift? I notice when I simulate one it improves not only my nasolabial folds (which seem to have gotten more pronounced after this implant was installed in addition to the double jaw surgery I had at the same time which included 8 degrees CCW and 2mm impaction) but also improves the step off beneath the implant. The upper portion of the infraorbital contour is still visible though.
If I opt to have the implant removed, do you think I would experience midface sagging based on the design shape and my anatomy? I am 27yo for reference.
A: A midface lift has zero chance of making any improvement in the visible outlines of these implants. Lifting with your fingers is not replicative of what will happen from a midface lift in a young person with otherwise taut skin.
Camouflaging implant edges comes from volume addition.
The question is not whether you will have tissue sagging after implant removals, as you will, the more pertinent question is how significant it will be and whether the sagging is a better aesthetic problem than that of the implant show.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello is there a procedure to make the chin less prominent and not make the smile look so “forced”? I don’t want that under bite look. I got cheek filler and it looked how I wanted.
A: I could see how cheek implants would make the chin look less prominent as it helps ‘pull out the midface above it. Fillers a good test to see if that effect is a positive one which clearly it was. You might also combine those with paranasal implants to enhance the midface augmentation effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Looking for solutions to eyebags and darkness under the eye at 18 years old.
A: I can appreciate the undereye hollows, the darkness not as much. Undereye hollows can be treated by synthetic fillers, fat injections or implants. As a very young person the first step is to try fillers to be sure augmentation provides the proper aesthetic effect. If it does then a more permanent solution with implants can be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have very large temporal muscles that I want reduced. They stick out significantly from the side of my head after yawning as well as chewing when I haven’t for a long time. It is not normal to look like this with such bulges. What is involved in reducing the temporal muscles. I have attached some pictures for you to see what I mean. I also feel an extreme tightness/discomfort whenever I’m chewing when I haven’t for a long time.
A: While removal of hypertrophied temporal muscle can be an effective procedure, not all of the temporal muscle areas can be reached from an incision behind the ear and certain areas need to be avoided to prevent jaw dysfunction. (see attached diagram which in yellow shows the area where temporal muscle ca be removed)
You have a uniquely distinct area of temporal muscle hypertrophy that I have never seen before in its precise location. This is exactly where surgical muscle removal can not be done. as the aforementioned diagram shows. This can, however, be treated with Botox Injections which can effectively shrink down the size of the muscle in a non-surgical manner. A good 50 units per side as an initial treatment will produce a visible reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, . I’m interested in hip augmentation and I have the following questions:
1- I know that you advise having fat injections first on the hips but, is it possible to augment the hips with custom implants first and, if implant edge reveal becomes an issue, to come back and fix it with fat injections?
2- If the answer to the previous question is “yes”, then how soon can one have fat injections on the hips after having custom hip implants?
3- Would the fat be injected just on the edges that can be seen?
Thanks in advance
A: The reason that I advise fat injections before hip implants is the hope that the fat will create enough of a hip augmentation result that implants will not be necessary. Hip implants have a high rate of complications so they should only be done when autologous augmentation is not an option. (don’t have any or enough fat to harvest)
Fat injections are a treatment option (along with synthetic fillers) for the most common hip implant complication of inferior edge show Such show is not evident until 8 to 12 week after placement when all swelling has resolved and the soft tissue shrink wrap effect has occurred. Fat injections are placed around the visible implant edge to try and camouflage it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am assisting in research for my girlfriend regarding a breast lift. She wants her breasts to be higher profile (more northern pole mass). We kind of understand that a normal breast lift will not achieve what she wants really.
She has 500cc silicon implants already. I was researching the REFINE tissue anchor and stumbled across your practice.Can you provide a little information on the REFINE system and if you think she can achieve that real high profile look she is wanting?
A: I would not have confidence that the Refine Breast Lift can produce sustained breast lift results on top of a large implant. Not to mention the difficulty of navigating around a implant to do so. This needs assured volume like a different and larger breast implant or upper pole fat injections.
As a general rule you can’t lift your way into increased permanent volume.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Looking to get six ribs removed to get smallest waist possible. Wondering if this is something you would consider doing or if it’s too dangerous. Thanks so much!
A: You are referring to Type 2 rib removal which I do frequently. The question with any form of rib removal is not whether it is dangerous, as it is not, but how effective it will be for the patient’s waistline reduction goals. I would need to see pictures of your torso to help make that determination.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a pretty healthy and lean person overall with a low body fat percentage. However my face holds a lot of face that isn’t proportionate to how much overall body fat I have. As a result, my cheeks are chubbier then they should be and I have received buccal fat removal but that did not really impact much as the fat is above the buccal fat area. My question is there anything that can be done to remove the fat, not sure what other procedure would even work but is there anything that would spot target that?
A: In the upper cheek area to which you refer there are no significantly effective methods of fat removal. This fibrofatty area is not a great area for liposuction and there are branches of the buccal facial nerve so the risk vs reward benefit is not great.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I get orbital box osteotomies if I have had prior orbital decompressions?
A:As for the close set eyes the only effective procedure in an adult would be a subcranial 180 degree orbital box osteotomy. But having had orbital decompression with bone removals, both medially and laterally that is a procedure that would probably not be effective now. (the bone would probably fracture)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, what are the side affects of skull reshaping surgery?
A: This patient failed to provide what procedure to which he refers. Skull reshaping is not a procedure, it is a broad term related to a collection of over 30 procedures done to augment or reduce parts of the skull/head. In other words I can’t properly answer the question unless I know the exact procedure to which he refers.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in hip implants. I am tall and lean with little fat.
A:Thank you for sending your pictures. With a very lean body and with decent thigh musculature despite the lean frame I can certainly see why the interest in hip implants. My initial general comments in hip implants based on a lot of patient experience is the following statement:
Hip implants have a fairly high rate of complications so patients have to be selected very carefully to try and lower those risks. There are two major risk factors, 1) thin patients with little subcutaneous fat (inadequate soft tissue cover) and 2) implants that are too big. (too thick for the tissues to adequately support them) The key to lowering these risks is to avoid putting in an implant size that exceeds their soft tissue capability to adequately handle it. (aka provide good camouflage of its edges)
While these hip implant issues certainly apply to you (thin subcutaneous fat layer) the key to lowering these risk is keep the implant projection at 1.0 to 1.2cms and the vertical length of the implant not overly long. (less than 20cms)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m just wondering in clavicle reduction (shoulder narrowing) surgery will this cause long term side effects like hunched back or muscle pain or upper body motion restriction?
A: No it will not.Such effects would only occur in longer segments of clavicle bone removal than the procedure is capable of doing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some other follow up questions relating to a skull implant. I’m trying to get a better idea of how this will impact me in the long term if any medical issues arise that I would need testing or imaging for. Would this affect my ability to get an EEG, especially measuring any activity in that frontal area where the implant is placed, either from the screw or the implant itself? Have you had any patients that have reported any impacts or limitations to diagnostic testing of the head/brain due to this kind of procedure?
A:When it comes to CT and MRI imaging a skull implant or its titanium screw(s) do not pose any restrictions on getting it or affecting the obtained images. When it comes to an EEG this is not a question that I have ever been asked before or have ever had a postop patient who needed an EEG. So I can not provide a qualified answer in that regard. I suspect that neither pose an issue, particularly the implant. But if any doubt don’t use a titanium screw for fixation. (it is nit usually an absolute necessity in some skull implant cases)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi can you guys do a male to female head/ skull reshaping to make my head more like a female shaped head, if so how much would that cost?
A:Feminizing the head is largely a function of reducing prominent areas such as the bony temporal and particularly the forehead since it is the most visible part of the head given hair coverage. But determining one’s skull reduction and its potential benefits has to be done on an individual basis so there is not a standard formula for doing so. This process starts by first getting some pictures of your head, getting a description of your head shape concerns and then doing some imaging if the hair permits it. Thus what your specific skull reshaping needs are remains undetermined presently and until that is better known we can provide a cost for doing so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, as you can see in the photos i have an irregular shaped forehead. I’ve gotten CT and MRI scans and they say nothing is wrong. But I’ve always had discomfort in this area, all my life. Unfortunately I’m not located in Indiana, but I can’t find anyone that can do this. I have a copy one CD format of my CT scan. Please help.
A:What you have are classic prominent forehead eminences. (aka forehead horns) These are aesthetic bony prominences so a CT scan is not going to show any abnormality, it will only show how thickness of the bone in that area of the forehead. These are not known to be associated with discomfort so I have no explanation for that symptom. In improving the shape of your forehead there are two very different directions to go, reduction vs augmentation. In a flatter maie forehead reduction of them would be the unequivocal choice of treatment. But your forehead is sloped/narrow so camouflagung them by building out the forehead around them is an option. But in the end the approach is one that the patient aesthetically prefers.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have questions/concerns about my facial implants which were placed six months ago and have healed fine.
1)Are there still risks of infection?
2)If so, what precautions can I take to minimize the risk of an infection occurring?
3)Can a general infection cause an infection in my facial implant?
4)For instance, is it possible for a foodborne infection, like one from eating raw fish such as sashimi, to lead to an infection in my facial implant?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a chin implant with terino style 1 back in February. The issue is that the chin looks pretty different from the front and the mental crease has drastically increased; the bottom part sticks out more than a normal chin should. What can be done, if anything at all to fix this problem?
A:What you have undoubtably discovered is that when considering chin augmentation you need to factor in what it may look like from the front as well as how it looks like in profile. Too many patients and surgeons only make chin implant decisions based on how things may change in side view. By definition every chin augmentation will deepen the labiomental fold, this is unavoidable. The more horizontal projection the implant has the deeper the fold will get. How much projection a chin should have is open to personal interpretation so this is an important issue to determine before the surgery. I would ask if computer imaging was done before surgery of differing amounts of horizontal chin projection so YOU could provide insight into what looks good to you….but that is a question to which I already know the answer. (it was not done)
That being said the only way to improve your current concerns is to replace the implant with a smaller one.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, In attempting to find a solution for my columella show (image included below) I recently read a paper “Alar Batten Cartilage Graft: Treatment of Internal and External Nasal Valve Collapse” published in Aesthetic Plastic Surgery (paper attached).
My photo below shows my current situation – my previous surgeon seems to have conducted an alar rim reduction in conjunction with the lip lift. As a consequence, I have less support in my sill and very little philtrum. Elevating my columella also raises my upper lip (which is not an entirely unwanted effect [exaggerated below] as it helps to address some asymmetry).
I found the paper very informative, largely because it contains a case showing a nasal sill being elevated and stabilised through the use of an alar batten graft. This is in Figure 11 (shown below), which also demonstrates a case of congenital nasal valve collapse. The postoperative images show a profound improvement in the nasal sill anatomy, which I find quite remarkable. While I understand the primary purpose of the alar batten grafts, I’m curious about the specific forces at play that led to this significant change in the nasal sill.
Do you have any insight into this effect and how it might be applied to my situation? My hope was that through a series of alar grafts and a columella retraction suture(s) I might be able to improve my current situation, though I’m unsure whether increasing the projection may also assist.
A:The answer to your question regarding nasal sill/rim retraction is that structurally the three maneuvers of alar rim grafts, tip derotation and columellar retraction suturing are all that is possible to try and improve your current situation. All I can say about them is to increase the chance of their success is: 1) all three must be done concurrently (difficult problems require maximal effort) and 2) a rib graft may be needed to provide adequate material for the grafting. The other alternatives are combined septal and ear cartilage grafts.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have found your website a fantastic source of information. I hope you don’t think I’m taking a liberty by contacting you but I wonder if you would kindly answer a question for me as I can’t find the information elsewhere. My daughter had injectable HA based filler (2ml I think) in her chin about 18 months ago and the effect is still apparent. She’s just had a sliding genioplasty (no jaw surgery because of TMJ problems) as part of orthodontic treatment with the filler in place. The surgeon had plenty of photos of her natural appearance throughout the orthodontic process so he was well aware of her natural chin line and told her not to worry about dissolving the filler first. He did a 10mm advancement only but the result is very dramatic and the chin is too prominent at present. She is 2 weeks post surgery and obviously still has some swelling on her chin but I think the filler is making the chin look over projecting. Psychologically this is having a huge effect on her and she is currently very unhappy with her new look. I have read on your site that the healing process does a good job of dissipating and absorbing the filler but I’d be extremely grateful if you would give me some idea of how long this would take. Would it be along the same time frame as healing, so that in a few months time, the filler would have gone along with the swelling? If she needs to have the filler dissolved, how long after surgery should we wait before having this done?
I think you sincerely in advance for any advice you can give me so that I can put my daughter’s mind at rest. As you can imagine, it is a worry for me too.
A:While the filler will dissolve over the next 6 weeks I would doubt that this dissolution effect will make much of a difference on the true final result. (filler becomes compressed when the bone or an implant is put behind it…..thus its residual effects are not that significant) But it isn early and the true answer about whether the chin is overprotected or not takes a good 6 to 8 weeks to know for sure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon