Your Questions
Your Questions
Q: Dr. Eppley, I have a question regarding the intraoral approach to treating horizontal hyper-projection of the chin.
In your previous discussions, you emphasized that the most effective method for addressing hyper-projected chins in the horizontal plane is bone burring via a submental approach. However, it seems that many plastic and maxillofacial surgeons may lack the experience or training for this procedure and often prefer intraoral osteotomies instead.
I was wondering if a wedge osteotomy could be considered a viable alternative for reducing chin projection, as opposed to a reverse sliding genioplasty. If so, would the wedge osteotomy present similar aesthetic challenges as the reverse sliding genioplasty, such as soft tissue redundancy in the submental region and a boxy chin appearance in the frontal view? Additionally, would this technique inevitably reduce the vertical height of the lower third of the face?
I greatly appreciate your insights and guidance on this matter.
A: The key to any horizontal chin reduction lies in the soft tissue and not the bone. It doesn’t matter how the bone is reduced, what matters is what is going to happen to the excess soft tissue chin pad once its bone support is lessened. Only the submental approach allows for soft tissue removal/tightening. This issue is not going to be overcome by any intraoral osteotomy..
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 29 years old male who is going to have a sliding genioplasty (8-10 mm horizontal projection) next week.I am very concerned about the large step off areas located both superior and posteroinferior parts of my advanced distal chin fragment.I know that their occurence will be inevitable because of my large horizontal advancement(8-10 mm).
My question is that
Can we get a fully filled up smooth bone contour by properly grafting those two step off area bone gaps (particulary the one locating at the inferoposterior area of my chin) with allogenic bonny grafts like hydroxapatite which will be replaced by my own bone?
Thanks for answering.You are the most skilled plastic surgeon I have ever seen.
A: With a low angled and long osteotomy cut there is usually no significant step offs in my experience with 10mm+ sliding genioplasties. But for the sake of this discussion you are askng about grafting them should they occur to which I can say the following:
1) Hydroxyapatite is a ceramic calcium phosphate material which does not turn into bone….but it doesn’t have to as a permanent bone void filler material.
2) Allogeneic or cadaveric bone chips have the potential to allow bone ingrowth…although it is usually not robust or complete.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m wondering what I should do of my ears position and rotation, is it possible to rotate them to be more straight, or would a reduction help at all? I don’t know if they are lowset or just big and tilted. What can fix this
A: They may be a bit low set and with a backward tilt, neither of which can be changed. I would no advise ear reduction either as with a large concha that would look odd with the usual high-low ear reduction technique. The only ear reduction technique that could be done is a mid-conchal excision method but that may make more of backward tilt effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m not interested in having more chin. I have too much as is. am *scared of this ending up appearing as though I have a more lengthened chin, but I am still interested if this fixes the problem. There’s also a curved line above the tissue of my chin present when resting or static. Would this be addressed if I were to have this procedure?
A: Lengthening the chin does help soften the deep labiomental fold. The deep labiomental fold exists because the bone is not long enough to support the size of the soft tissue chin pad.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr., Eppley, would you have any idea what type of metal was used for chin implant screws in 1995? (I need to have a MRI, but no one knows what type of metal it is). Do you know if titanium screws were even used yet in 1995? Thank you!
A: Most likely titanium in 1995 but no one can say for sure. The x-ray will not provide that information as the material density between titanium, stainless steel, and vitallium is not that different.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some facial asymmetry and I’m potentially interested in pursuing custom implants as a solution.
When ordering a CT scan of the head, is there anything special I have to ask for to totally maximize image quality, other than that they use the thinnest possible slices and send me 100% of the raw data with no postprocessing?
A: We place the order for the 3D face CT scan so there is no confusion about how it is done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in learning more about testicle implants and exploring how it may be possible to achieve an oversized low “bull” look. I have seen a few different self achieved cases over the years that have turned out incredibly aesthetically pleasing to me, however the one I adore the most was self injected silicone (~700ml) which I have reservations on for obvious reasons. The “locked in” sheath look he accomplished is amazing, but I am not sure if that is achievable in a medically safe manner. I am fully fine with limitations on penetration if something like that is possible. My testicles naturally ride high and my scrotum is pretty stretchy which leads me to believe that I may be a good candidate for side by side. I would eventually like to have an oversized look similar to the attached images.
A: To achieve that look it would take custom side by side testicle implants. Whether that would require more than one set of implants to come closer to that look is the unknown question.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
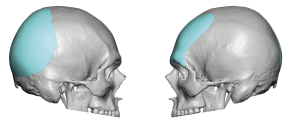
Q: Dr. Eppley, Hi there, I have a question about skull reshaping. I have a shaved head so I’m concerned about scarring. Is there a way to do this surgery without visible scarring on the scalp?
My head shape and hair style is very similar to this. Before I proceed, I just wondered if this is a realistic procedure for someone who keeps a shaved hair style or if it must leave large visible scars.

 A: Sagittal ridge/crest reductions are one of the more commonly performed aesthetic skull reshaping procedures. The shaved head or bald male patient is the typical patient who presents for it. While no form of skull reshaping surgery can be without incisions and resultant scars the incision used in sagittal ridge reduction are very small and heal in a near imperceptible manner. No patient has ever stated the fine line scar bothers them or had requested a scar revision.
A: Sagittal ridge/crest reductions are one of the more commonly performed aesthetic skull reshaping procedures. The shaved head or bald male patient is the typical patient who presents for it. While no form of skull reshaping surgery can be without incisions and resultant scars the incision used in sagittal ridge reduction are very small and heal in a near imperceptible manner. No patient has ever stated the fine line scar bothers them or had requested a scar revision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a male looking into a chin augmentation as my chin is recessed upon researching the implantech website, I had some follow-up questions. If my primary goal is to increase lateral projection, and I have a deep mental crease: what implant would be most suitable for me, the flowers mandibular glove, the extended anatomical, or the Terino 1?
They all seem like great options, just unsure which would be best.
A: Since you mentioned lateral (horizontal chin augmentation along with a deep labiomental crease my assumption\ is that you may believe that one of the three chin implants styles may not magnify the depth of the labiomental fold. The reality is any form of chin augmentation os going to do exactly that regardless of chin implant style. It cannot be avoided as the labiomental fold is a fixed anatomic point that lies above the part of the chin that is affected by implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am inquiring about a virtual consultation for thigh implants. I just want my thighs far more proportionate to my body. Actually, I’d like them to be larger in comparison to most other things, but I still understand having realistic expectations. I don’t care to have the “muscular” look, just looking to make them more proportionate as I’ve always been an active person and muscle building lacks in this area. I’d like for them to stick out past my stomach in front for a “thicker” look to them.
A: I don’t know if thigh implants could realistically be tissue tolerated (made and inserted) to have that much anterior projection in the subfascial pocket location. That would appear to be at least 2 to 3 cms of implant thickness (if not more) and I would highly doubt the fascia could be expanded that much. You would have to have the implant placed on top of the fascia, which can be done, but the risks of complications increases considerably in doing so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Could you possibly explain what a scalp expansion would look like. When I review your patients that received a first stage scalp expansion, the process seemed to take months. Do most patients remain home for this process? Or is it not obvious to anyone? I’ve seen pictures of patients with tissue expanders and I am a little scared of the “bubble”-or expander. I wouldn’t mind this if I was able to conceal it, because the images I’ve seen are maybe exaggerated? I guess what would help me to consider this would be if I understood the scalp expansion stage to be a “concealable” process!
A: 1) Scalp expansion is a 3 month process.
2) All scalp expander fills are done by the patient at home.
3) While scalp expansion for aesthetic skull augmentation does not stand out like the overfilled expansion needed for scalp reconstructions.,I would not say it is completely undetectable in its latter stages of the fill process.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am more interested in a genioplasty than a chin implant.I am looking for movements around 12 mm horizontally and 5 mm vertically. However, I am concerned that a minor impact to the chin in the weeks following the procedure could cause it to relapse a little? How rigid is the plate, before the bone is healed?
A: By looking at your pictures I suspect that the combined movements of 12mm horizomtal and 5mms vertical may be a bit over estimated. But that issue aside I have never seen a patient lose fixation stability after surgery from trauma (if they had it) but that does not mean it could never happen. But the best way to address that potential concern is to add a smaller stabilizing plate on each side of the main plate. (three point fixation)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, hi , i am looking forward to see the options for reducing my head size significantly.
my head size, height not of an average ppl
it’s nearly at 10 inch. can we get it shorter?
A: While skull height reduction can be done within the limitations of outer cortical table skull removal (7mms) I don’t think I would call that ‘significant’ when head height is defined in inches.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am looking into crown implants for a flat head and to increase my cranial top. I was just wondering if anyone knew if these implants “smoosh” your brain or add too much weight on the top of your head leading to increased inter cranial pressure.
Also, do those who have gotten this surgery feel the implant pressing on their skull?
Thank you!
A: In answer to your skull implant augmentation guestions:
1) Custom skull implants when placed on the bone will feel just like bone.
2) Such implants are placed on top of the skull bone and, thus, have no impact on the brain which lies on the other side of the skull bone.
3) Custom skull implants are light weight, most weighing between 100 and 150 grams. (1/3 of a pound) Even very large skull implants, which require a first stage scalp expansion, weigh only between 200 and 250 grams. (1/2 a pound)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am inquiring about head widening My skull is a bit narrow when I shave my hair. I read about implants you can use to make the skull look wider. Can you tell me more about it.
 A: The best approach to widening the head in a ‘scarless’manner is with submuscular temporal implants placed an incision in the crease of the back of the hears. Such implants are usually 5 to 7mm in maximum thickness centered above the ear.
A: The best approach to widening the head in a ‘scarless’manner is with submuscular temporal implants placed an incision in the crease of the back of the hears. Such implants are usually 5 to 7mm in maximum thickness centered above the ear.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would you also be able to do a genioplasty with a large horizontal movements, but with a split in the middle, so that the chin will not become narrower?
A:These large bony movements work because it is a single solid bone segment. Splitting introduces the risk of instability and limits the amount of projection that is possible. In essence splitting the chin is a recipe for problems.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
A: Dr. Eppley, hi I was wondering about the iliac crest reduction surgery. what is the amount of length the hip is reduced by, is it doable on men, and does it harm or remove any muscles.
A:It is 1 cm reduction per side at the widest part of the iliac crest. There is minimal disruption of the gluteus medius muscle whose central part of the muscle lies underneath the reduced crestal area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 3o year old male with a flared lower left rib. I would be interested in getting it repositioned, or removed if necessary. It is not affecting my quality of life; it is purely cosmetic. Would you be available for a virtual consultation to discuss treatment options/financing/recovery times? Thank you very much for your time.
A:You have a flared or winged right subcostal rib margin. This is probably rib #9 by looking at this picture but palpation would confirm that more accurately. A 3D CT scan would absolutely provide the best visualization and tell us if this is a just a single rib involvement. The surgical debate is between shaving/removal vs repositioning, each with its own advantages and disadvantages. Removal = assured permanent result, more incisional length, ‘longer recovery’ vs Repositioning = need for postoperative banding, risk of relapse, minimal incisions, quicker recovery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, can you do a surgery where you realign the zygomatic bone? Like say if one person cheek is smaller than the other, the zygomatic bone is pressed in or angled badly, could you bring the cheek bone thats pressed in, outwards or straighten it to help with asymmetry?
A:Whether the more inward cheekbone one can be satisfactorily expanded/brought back out depends its current shape and how much movement is needed to do so. This would require a 3D CT face scan to make that accurate determination. However the 3D CT scan you have is of poor quality and I have only seen a front view picture of it. It takes a submental view to get a better assessment of the cheekbones.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 28-year-old male with a protruding occipital bone (I don’t know what caused it, maybe it was caused by my sleeping position when I was born?). This caused me some troubles. I consulted online at a hospital in China, and the doctor’s answer was that surgery was not recommended because it was too dangerous. So I found your organization on Google and saw that you have many surgical cases for reducing large occipital masses, so I would like to get your advice. I don’t know if the consultation is charged, and I hope to get your reply. Thank you
A: You have what appears to be either a large occipital knob or a small occipital bun skull deformity. It can safely be significantly reduced as the thickness of the skull bone in this area is usually sufficient to do so. (see attached image) I also check a lateral skull film first to be sure the bone is thick enough to do so but to date it always has been. What is interesting is that in the many hundreds of all forms of occipital reductions that I have done I don’t recall ever having an Asian patient. I think this is because the genetic tendency in most Asian skulls is one of occipital flattening as opposed to a protrusion. But regardless of its less comon occurrence in the Asian skull its successful reduction can still be achieved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in genioplasty for both horizontal and vertical lengthening.My local surgeon can achieve 12 mm horizontally and 5 mm vertically but will not do more horizontal advancement due to limited bone contact at the lateral wings.
I’ve seen that you’ve performed 14-16 mm advancements. Is that always possible, or does it depend on factors like chin thickness?
Thank you.
A:A 12mm forward movement with 5mms vertical is a pretty good movement. But at 14 to 16mms the wings would still have some bony contact which isn’t that important since it would be grafted with either allogeneic bone chips or a bone block anyway. The real question is not about the bone contact but whether the bony chin will permit such a forward movement to be done. The stretch of the attached soft tissues to the chin bone segment may or may not allow for such a movement to be done. That can never be known for certain until it is actually attempted.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I have a question for the doctor. I had an implant put in on the front and back of head. I was curious what kind of damage could be done to implants if I decided to do boxing. Is there a low or high for damage to implant?
 A: Good to hear from you as we just passed our 2 year mark from your skull implant surgery. Your question is a common one and the answer is no such problems have ever been seen or reported. The implants can not be physically damaged by any type of traumatic forces. So think of them a bit like bone which is how they feel. They also have a low probability of being displaced…so low that it is about as close to zero as can be.
A: Good to hear from you as we just passed our 2 year mark from your skull implant surgery. Your question is a common one and the answer is no such problems have ever been seen or reported. The implants can not be physically damaged by any type of traumatic forces. So think of them a bit like bone which is how they feel. They also have a low probability of being displaced…so low that it is about as close to zero as can be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am also interested in having my eyebrows set lower to my eyes and reshaped.. would this procedure cover that?
A:Lowering of the eyebrows is always a hard change to make because the brow tissues on the lower forehead are tight and don’t stretch easily. But the subperiosteal tissue dissection and brow release with the placement of the implant pushing down usually provides some modest improvement in the brow position.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What about iliac crest reduction for us hip dip girlies? Is that an option?
A: It is an option but probably the iliac crest reduction would not get rid of the hip dips completely. I see that having value when combined with fat injections to the hips or even a very small implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I read that mandibular angle implants are at most 6mm in width but I am trying to figure out if it is possible to achieve more than that e.g. 12mm per side would be 2 implants per side of 6mm so a total of 24mm added to bigonial distance. Would love to hear if this is possible or if there’s another way to get more than just 6mm on each side. Thank you so much
A:I am not sure where you are getting your implant information. But standard jaw angle implants come in widths up to 11mms and custom ones can have any amount of width.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
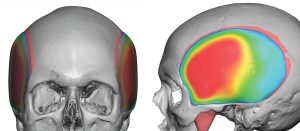
Q: Dr. Eppley, My forehead sticks out more making me lower face looked pushed back so if some slope could be added so that the farthest my forehead goes is my browline, that would be amazing.
Here are the pictures of my forehead, you can see that the middle part sticks out and widens and elongates the forehead. While also having this bone lump, my hairline is far back and so are the sides. I was wondering if it would be possible to push in the sides while also lowering the hairline( I inserted a picture to show what I hope it would look like, forehead shape and everything
A: Let me make sure I understand what you are asking…
If I compare your forehead to that of what you consider to be a more desirous shape in profile you have more of a protrusion and not a smooth forehead slope. This would indicate that a bony reduction is needed in the middle protruding part.
In regards to the hairline the frontal hairline can be advanced to help shorten the forehead but the sides (temporal hairline) can not be changed/moved without major visible scarring.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I think I have what is referred to as frontal bossing and/or frontal horns. My forehead also appears asymmetrical.I’ve just always known that I had an unusually large forehead, which has been a source of insecurity throughout my life. I am contacting your office to see if anything can be done to address the aforementioned issues, with minimal risk and without significant scarring. justtso you know I am 45 years old. As you will see from the pics, I am also bald, which raises an issue as to whether any needed incision(s) could be readily hidden.
A:In forehead reshaping surgery in a bald patient there is no good place to put an incision. For the very highly motivated patient (one who is willing to accept some visible scarring) I would use two small mid-forehead incisions placed in the existing horizontal wrinkle lines and would not even connect them across the middle. (see attached picture) This gives the incisions the best chance to heal in a location which already has a natural wrinkle and is parallel to the RSTL (relaxed skin tension lines) of the forehead.
That being said, in the end it comes down to the choice between which aesthetic problem does the patient prefer…the present forehead shape with no scar or a reduced forehead with some slight scarring. Every patient will view that choice differently.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, has there been any developments to the wrap around testicle implant procedure or does the doctor still not recommend it as a viable long lasting option?
A: I remain less than optimistic about it. The only ‘technical advancement’ has been to get a preop ultrasound to determine the exact size of the testicles and then custom design the inner chamber of the implants to match it
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I’m considering genioplasty and jaw implants. As a professional bodybuilder, I’m concerned about how long I’ll be unable to train after the procedure and the potential complications that could arise from resuming too soon. How quickly can I safely return to the gym after having both genioplasty and jaw implants?
Also what is the risk of masseter dehiscence if I go for an implant that mostly augment the width and not so much vertically?
And my last question; when can I return to normal daily life, without people noticing I had surgery?
A: In answer to your jaw augmentation questions:
1) You return to the gym when you feel comfortable doing so. Working out will not hurt the surgery so it is a question of soon you feel compelled to do so.
2) The risk of masseter muscle dehiscence decreases significantly when a width only angle implant augmentation is done
3) Most jaw augmentation patients start to look more non-surgical in 10- to 14 days after the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would it be possible to view predictive imaging for my right profile for frontal bossing reduction The left side looks good I just want to see what it looks like in the right.
A: That can be done but the concept of imaging is not to show the patient the exact result they are going to get….as no one knows that with absolute certainty. Its purpose is to convey in this type of surgery how much bony reduction can realistically be expected as the frontal bone is not that thick. Your goal is to look at it on a general basis and determine either a) if I can at least get that amount of change then the surgery will be worth it, or b) it doesn’t look like enough or I am uncertain if it is…then you shouldn’t have the surgery.
The point being…imaging is a concept about what the surgery may do and not an exact detailed prediction of the reductive change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon