Your Questions
Your Questions
Q: Dr. Eppley, “Concerning the implant design process, glad to see previous implants are helpful to anticipate results, would pictures before my implants be helpful also? Its a few years/few pounds back admittedly.
I see 2 design rounds are built into the process, how does someone accurately give feedback on a 3D model knowing its under soft tissue? Is there a way to include corresponding images of my current face and implants so I can toggle between the differences of the new implant and what the new implant improves upon? That would be the best for me to visualize, would be pretty important for me to understand.”
A: In answer to your custom facial implant questions:
1) Pre-design imaging is always done to set the patient’s aesthetic goals. You have to know what you are aiming for when making an implant design.
2) 3D implant designing is not an exact science as no one can accurately predict what will or will not show through the overlying soft tissues. It is NOT done by making a design and then painting the soft tissues over them to see what it will look like as that technology does not yet exist. That would be invaluable if it did exist and would take out all of the guess work and uncertainties of the process.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Came across your site after seeing the mouth widening procedure you perform. I’ve always felt that my smile/lips are very narrow [and small], accentuated by a long face shape.
I’m interested in having this procedure to widen them, as well as additional lip augmentations to improve the overall look and size.
Additionally, I’d be interested in face & jawline lipo.
Would love to hear your opinions on the above
A: Mouth widening procedures are effective but have a high incidence of the need for scar revision as the mouth corners are exquisitely sensitive to surgical manipulation. The rest of the lips far much better when it comes scarring. I don’t like to combine mouth widening with other lip procedure unless it is a lip procedure that does not directly manipulate the lip vermilion.
It would be hard to imagine with your lean face that facial or jawline liposuction would provide much aesthetic benefit.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to remove Medpor jaw angle implants. I would like to know if the masseter muscle is automatically injured and disrupted ? For the aestethic aspect what is the consequence of this disruption ? Bulge around the angle ? Or is it just functional problem ? Thank you
A: In answer to your questions about the removal of Medpor jaw angle implants:
1) There is a real risk of masseter muscle disruption with their removal due to the tissue ingrowth of the muscle. This does not mean that it always happens but it is not an insignificant risk.
2) Masseter muscle dehiscence presents an aesthetic issue (contour deformity) not a functional one.
3) The contour deformity is a triangular soft tissue depression of various sizes based on the amount of lack of muscle coverage over the bony angle.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley I would like to place Medpor implants for customized cheekbones (64x19x7), because I want a significant increase in cheeks, but I am afraid of the risk of infections so I wonder would it be better to choose implants silicone, but I’m afraid that they will move because I lead a very active life. So could you tell me which type of implant is the least likely to become infected over time and which is the least likely to move.
Thank you.
A: The use of standard implants for customized cheek augmentation would not be considered truly custom as they are standard implants. Before considering an implant material the first question is what is the aesthetic cheek augmentation goals and what shape and size of implant can best achieve them. Then and only then does the consideration of implant material become relevant.
With proper technique and screw fixation the risks of migration and infection are not really different between the two materials. What really counts is which material can provide the best chance of a successful aesthetic result… and….how easy or hard is it going to be if a need for revision and/or removal is needed in the future. (which is a 20% to 30% risk in bilateral facial implant surgery)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have just discovered your clinic, I am delighted because I have long wondered if it is possible to have implants on the forehead as well as the skull, in order to have the upper face wider and rounder as women with big forehead often say are more attractive! That’s why I come to you because I’m interested in this intervention. Thank you very much
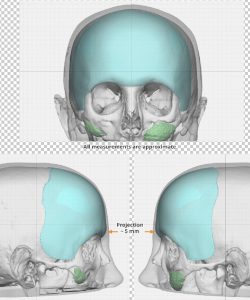 A: Thank you for your inquiry. Let’s start out by first determining what your aesthetic forehead/upper facial third goals by sending some pictures so I can computer imaging of them. I assume by your description that you are referring to the type of female forehead-temporal-skull augmentation as in the attached implant design image from a female who has undergone what you have described as your aesthetic goals.
A: Thank you for your inquiry. Let’s start out by first determining what your aesthetic forehead/upper facial third goals by sending some pictures so I can computer imaging of them. I assume by your description that you are referring to the type of female forehead-temporal-skull augmentation as in the attached implant design image from a female who has undergone what you have described as your aesthetic goals.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi my 14 year old son has a great complex.
He has uncorrected brachiocephaly. The pediatricians told us that it would correct itself but it did not.
At what age could I place the 3D implant?
A: Once past puberty I think it could be done anytime that the patient feels that it is aesthetically bothersome.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Will I need to replace at some point my custom facial implants? How long do they usually last?
A: The only aesthetic facial or body implant that a limited lifespan and would need to be replaced are breast implants which is gel silicone placed into a containment bag whose integrity will be eventually compromised. All other face and body implants are made of solid silicone material that never needs to be replaced due to device failure/breakdown. It only changes physical form at 375 degrees F.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Below are some images taken today of an otoplasty I had last week.
As you can see, the ears have been “corrected” quite strongly, and I would like a more natural look.
(I am aware that with time the ears will distance somewhat from the head but am concerned that they’ve been “over corrected”)
Would it be possible to arrange a consultation at the earliest available opportunity to see if your surgery could partially reverse the overcorrection.
A:Thank you for your inquiry and sending your pictures,. I would not disagree with your concerns and the best time to manage those concerns is early when the otoplasty sutures can be released or redone…which would avoid a graft which is needed later when the cartilage memory has gone. My experience has been that the concerns you see now do not change later as the amount of relaxation is very minimal. I would assume this is something your surgeon would be willing to do now.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am just inquiring around volume reduction/fat removal of the upper mouth region (the mustache area for men). Mine is somewhat protruding/convex and I have had to resort to facial hair in order to reduce the effects of it. In a classic sense, a concave upper mouth is more aesthetically pleasing and enhances the shape of the lips.
Are there any methods in reducing this area such as lipo extraction or surgery?
I noticed your response to this question in realself and thought I would contact you. I have submitted a photo for assessment.
Very much appreciate your thoughts.
A: There is no surgical procedure to reduce fullness in the upper lip/upper mouth area. Fat extraction can be done to the sides of the mouth (perioral region) but not at the upper lip area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions regarding eyebrow lowering through tissue expander. My eyebrows sit naturally too high on my face, which give me a feminine look. I know that Botox can lower them but not to the extent that I want, I think. My questions are:
1. Do you offer this procedure?
2. Will the expander be located right above my eyebrows, in the middle of my forehead or near my hairline?
3. While using the expander, will my appearance be too unsettling, kind of like if I have some sort of tumor?
4. How long would I have to use the expander? I know it’s difficult to say exactly, but do you think it would be longer than one month or longer than two months?
Thanks in advance.
A: The concept of lowering the brow position by tissue expansion is a theoretically sound one but has several caveats to it:
1) Short term tissue expansion will not work as all the expanded tissues will quickly retract from when they came. Short term tissue expansion would only work if a physical block (brow bone implant) was placed to prevent the tissue from shrinking back up.
2) It takes long term tissue expansion (3 to 6 months) to eliminate tissue recoil….which would be socially unsettling/unacceptable to go through.
3) The placement of the tissue expander always work best when it is closest to the tissue site that needs expanding.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I got the opportunity to speak with several of your past patients who were referred me to last week. It was a great experience and I feel confident that I wish to move to the next step. I have two final questions for Dr. Eppley that emerged from these discussions – could you pass them along to him when you get a chance?
1. Since my cheek implants will saddle the lower orbital rims, is it possible that they can be placed intra-orally? Or do you think that these will need to be placed through the eyelid?
2. In Dr. Eppley’s experience, is doing both the jaw implant and cheek implants in a single procedure too large of an endeavor for most patients? After hearing about the extent of the swelling from past patients, I’m trying to decide between the benefits of doing both in a single procedure (cost and shared recovery time) with the enormous amount of swelling that will result from two sets of implants being placed at once. Since this will be my first cosmetic procedure, does you recommend breaking this into two procedures? Or is it common for patients who do elect to receive both jaw and cheek implants to have them placed in a single surgical session?
A: In answer to your questions:
1) When the infraorbital implant saddles the infraorbital rim, it must be placed through a lower eyelid incision. Trying to do so intraorally exponentially increases the risks of infection, implant malposition and permanent infraorbital nerve dysesthesia. I learned long ago that the risk tradeoff is a very poor one. A cheek implant that has a significant infraorbital component is very different than one that doesn’t.
2) It is very common for the male patient to undergo combined jawline and cheek/infraorbital-malar implants. For those that desire both facial areas it actually would be more uncommon for these two surgeries to be separated. In the end, however, one has to do what seems comfortable as after all these are purely elective surgeries as there is no medical basis for whether they should be done in one vs two stages.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello doctor.Am a big fan of yours from The East. I am personally interested in the surgery that you perform as the name of temporal muscle reduction,as I am also not pleased with my wide head width.
Also there are some doctors who perform this surgery in the country where I live,they seem to be more passive about the muscles reduction it self.
Have you performed this surgery on Asian Americans as well?If so,please let me know.
Also,I would like to know what surgery I can take rather from malarplasty,as my facial width is quite wide and I dont like how low my IPD is.A selfie of my midface is attached.
I hope to hear reply from you ASAP. God bless you.
A:The location of the temporal muscle to which you have drawn is the anterior portion of the temporal muscle. Unlike the posterior temporal muscle (the muscle portion above the ears), the anterior temporal muscle can not be reduced by the same technique (total excision) and can only be reduced in a very limited amount, probably not an amount you would consider to be aesthetically effective.
For the zygomatic arch width beneath the anterior temporal muscle there is only the cheekbone reduction procedure (malarplasty) that can effectively reduce facial width.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, In the last few months, my skull has changed : the back of my skull is significantly flatter than before and there is this new bump close to the neck (seems to be like an occipital bun when I google, but I have no clue). It is very painful, difficult to sleep as it hurts when I lay on my pillow. It is the first time that I found something online that is similar to what I’m experiencing. It is driving me crazy because I have constant pain on my skull. I was wondering if you had any ideas what would cause these changes to my skull. Any help would be greatly appreciated!
A:While one would think as an adult the skull shape can not change every now and then I hear from someone, like you, that it can. Why that would happen I can not say. But what I do know is that for the painful occipital bun/knob that can be reduced which does relieve associated symptoms due to the protrusion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have had issues with my coccyx protruding and being prominent my whole life. This is something that has been a very difficult issue for me to discuss with anyone, but I did discuss it with one of my doctors in the past and she did not seem that concerned about it. It does bother me sitting for long periods of time in chairs with no seat padding or when I am trying certain exercises that cause pressure in that area …I.e. sit-ups. I have researched this issue and have not found a lot of information about this until I came across your website. I would like to know if a dermal graft would be an option for me to alleviate this issue. It has also affected my self-esteem as well because it just doesn’t look normal. I know this was very lengthy, but I will conclude now. I am willing to travel for the chance to feel normal in that area and not have any pain. Thank you.
A: When it comes to the treatment of coccydynia, the key question is whether this is primarily due to a prominent coccygeal bony protrusion, a lack of subcutaneous fat cover/thickness (usually due to aging) or a combination of both. In my experience some bony reduction of the coccygeal bone is needed combined with a dermal-fat graft overlay/interface. In other cases a total coccygectomy is needed. A dermal-fat graft rarely is ideal by itself.
I can not speak on an informed basis about your coccygeal anatomy and needs without seeing pictures of it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an orthognathic surgery of both my jaws along with mandibular angle reduction, I am positive that I want to restore my angles with implants, however I had screw removal surgery just now and my surgeon told me to wait for healing before having any other surgery at the same site, though he did not specify any particular time period. I would want to know as to how long I should wait before having implants to restore the angle. Given the covid scenario I’m definitely going to wait 6 months more for now, but should I wait upto one year as repeated surgery at the same site does increase chances of infection, and just to be safe in general. It’d be very helpful if you could tell me how long exactly I should wait, I’m willing to be as patient as necessary, just want to avoid any risks.
Also I’d like to know the price difference between standard and custom made implants (custom made to be the same size as standard ones but more accustomed for slight asymmetry). A rough idea for that would be very helpful.
A: In answer to your jaw angle implant questions:
1) From the standpoint of incisional integrity and healing, six months would be an adequate amount of time from your last surgery.
2) My assistant Camille will pass along the cost differences between standard vs custom jaw angle implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, It is so hard to find a really good facial surgeon. I am 58 years old and in the past year 2 years my face fell! I lost 50 pounds, went through menopause and had way too much sun. My lower face is awful to me. My mental crease is over almost my whole chin and no one locally seems to know what could be done about it.
Any and all advice greatly appreciated.
I feel like my lower face is worse than most 80 year old faces I see? Sigh…the struggle is real.
Thank you for your time!
A: Thank you for your inquiry and sending your pictures. You have to throw out the chronology (age) and just look at the anatomic problem. For all of the reasons you have mentioned, particularly the weight loss, your degree of lax/falling tissues does not match your age. The foundational procedure is a full lower facelift which will make a world of difference. The central chin area, however, is not going to change no matter what is done laterally to it. I believe you are specifically referring to raised mounds under your lower lip but above the labiomental crease. These are subcutaneous fat collections for which microliposuction would be the only effective approach to reducing them. They are not that rare as they probably occur in 1% to 2% of the general population.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m contacting you because I’ve had a complex about the shape of my skull for several years. Indeed, I find that my skull has the shape of an inverted “V” on the posterior saggital part. Consequently, as my hair is fine, flat and without volume, I have a hairstyle that looks like a “triangle” and this is not flattering. Also, when I tilt my head forward, the pointed side of my skull appears and the shape is not that of a harmonious rounding. When I tie my hair, I always pay attention to the elastic band to try to hide the defect of my head but often, the shape is still visible. I have added several photos as attachments so that you can see.
I have several questions if you agree to answer them:
First, I would like to know if you could suggest an aesthetic procedure to improve the shape of this part of my skull, to make it more rounded and harmonious, and if it would have a real aesthetic benefit for the overall beauty of my head (face + skull).
Would injections of my own fat be enough to improve the aesthetic aspect of my skull?
If not, should I consider a custom-made implant?
As I live in Europe, I would like to know if you have a colleague to recommend to me who works like you on cranial contouring.
Finally, could you give me a price range for such an operation?
Thank you in advance for your answer.
Best wishes,
A: Thank you for your inquiry, detailing your head shape concerns and sending your pictures. The definitive treatment for a scaphocephalic head shape is to either reduce the posterior sagittal crest (#1), bilateral parasagittal/temporal line augmentation (#2) or a combination of both. (#3) I will discard #1 and 3 for now and focus on #2 (volume addition) to which I can say the following:
1) While fat injections can be done anywhere, including the head, their volume retention in the tight scalp is precarious at best. But there is certainly no harm in doing so as a first attempt at skull augmentation. But the risk is high for either complete resorption or a minimal augmentation effect.
2) The definite and assured method of skull augmentation is a custom skull implant that is precisely made for your anatomy and aesthetic requirements. This is a common aesthetic skull augmentation procedure in my experience.
3) I am not aware of any European surgeons that perform this type of aesthetic skull reshaping surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was interested in facial implants. I’d like to know the cost of temple and cheek implants. I want a cheek implant that would give only projection and no width since I already have adequate width.
Also, would temple and cheek implant provide a subtle lift in the jaw area? I was considering a facelift but thought the face would look too tight after both the implants and the lift. I need very subtle lift in lower jaw area.
A: In answer to your facial implant questions:
1) To have cheek implants provide only forward projection and no width that may require a custom implant design. It would depend on knowing more about your specific midface augmentation goals.
2) Temple and cheek implants are not going to provide any lift in the jawline area as that is too distant from where the implants have any lifting effects …which is very modest in that regard anyway.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull augmentation. I can’t believe the amazing results you achieve. The shape of my head has bothered me for a long time. I have looked into having surgery here in the UK but my options were to have a very large cut and not like the small incisions you make. The results I would like the achieve are something very similar to the below image. I just have a few questions if possible? I was quoted in the UK with the large incision. Can the implants migrate? Can they cause headaches and can you feel the implants if you were to run your fingers through your hair?
A: In answer to your skull augmentation questions:
1) Onlay skull implants do not migrate regardless of their size.
2) Onlay skull implants have never caused headaches in my experience.
3) Onlay skull implants have a smooth contour and a seamelss edge transition onto the skull bone. Thus you can not feel them if you touch your head or run your fingers through your hair.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, my goal is to reduce the head circumference in the back of the head with the goal to achieve a smaller head because in my opinion my head looks really big with 59 cm head circumference. I will link some pictures so you can see the problem I am talking about. The red marked in the picture is where I would like to reduce the skull size if possible. The ”bump” in the back of the skull so to speak.
And my last question, on an average for people like me who want to do this type of skull reduction in the back of the head, how much skull reduction is normal to expect less than 1 cm or a little bit more? Because I had a hard time finding answers online.
I just wanted to see what you would answer on these questions and after that I might book an online consultation.
Thank you for taking your time
A: In answer to your skull reduction questions:
1) I have imaged what I think is a realistic amount of back of the head skull reduction. As a general rule such skull reductions run in the range of 7mms of bone removed until the diploic space is reached…which is where one has to stop.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Dr. Eppley and his team seem top-notch – highly skilled and experienced. I would request for a consultation, but it is far, unfortunately. May I ask for expert advice and/or referral?
I have a recessed chin and no visible jawline which has bothered me since teenage years. Despite orthodontic treatment in the mid-90s (headgear + braces), my overbite persisted. I am embarrassed to say I still felt ugly, especially when I noticed my side profile in pictures at school. What’s worse, I did not use a retainer judiciously. Fast forward a couple decades and I have an appointment set for next week with a local orthodontist in Memphis, hoping to *finally* fix the overbite and some crowding that occurred over the last 8 years.
I have not seen the orthodontist yet, but I have been online reading a bit more, searching for doctors who have helped patients with similar profile photos as mine, looking at before+after photos. From these, I am reminded that braces alone will not help me with my lacking jawline + recessed chin. I discovered that I need help determining what would be the best approach: a chin implant, sliding genioplasty, or jaw surgery. Seeing that Dr. Eppley has helped so many patients with similar problems and facial features, would Dr. Eppley be able to determine which procedure would be needed? I attached photos of my face if that might help.
I have no jaw pain, my bite seems okay other than the overbite. My face is slightly asymmetric (left cheek? larger than right). Simply put, I don’t think I need jaw surgery but I am unsure. If I only need a chin implant, that’s a relief, but if I need a sliding genioplasty, could I possibly find a surgeon with similar expertise as Dr. Eppley?
Thank you for taking the time to consider my case (photos attached)!
A: Thank you for your inquiry and sending your pictures. Like all chin augmentation patients one always has the option of a chin implant vs sliding genioplasty. While I think you would be best served by the sliding genioplasty long term, there is nothing wrong with a chin implant option…as long as it is the right chin implant style for a female and it is securely positioned on the bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had 9 months ago a ZSO (zygomatic sandwich osteotomy) procedure. I don’t like the outcome. My surgeon used bone marrow from my hip. Is it possible to revise this procedure? Do I assume right, that you would just pull the graft material ( in this case bone marrow) out and push my cheek bones together again?
Is the revision more risky than the former procedure?
A: You can reverse a ZSO (zygomatic sandwich osteotomy) by a wedge resection of the now healed grafted bone and putting it back where it originally was. It has no more risk than the original procedure minus the need for a painful donor site.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, thank you or your understanding and expertise, but I value my frontal face angle more than my side so I don’t mind altering the profile. Like I said I wanted to reduce my cheek size when I smile but you explained that wasn’t possible. How about the soft tissue bulges at the side of my nose when static (as seen in the pictures), can they be fixed with cheek implants/paranasal as I desire a more robust frontal look like the model? Can the cheek implant alone stretch that area so that light hits the malar area instead of my midface or will paranasal be required too. Finally can implants in my face cause my cheeks to pop out more when I smile? If this is possible then I would like to schedule a consultation to discuss more about this.
Thank you
A: While paranasal/midface implants can push the tissues forward along the side of the nose I can not say whether that would be enough to flatten the bulges to which you refer. In theory it should…but that remains an as yet unproven theory in your case.
Whether cheek implants can stretch the soft tissues to change the soft tissue highlights would be heavily dependent on their shape and size. That is another one where that should be possible but not completely predictable.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a body builder who wants some help getting a classic v-taper to my body. I think the hip bone shaving procedure is what I’ve been looking for. But how much volume does this actually remove from the hip area?
Thank you so much!
A: On average the widest part of the iliac crest that can be reduced (hip bone shaving) is in the 1 to 1.5cms range. But for a very active person (aka body builder) this would not bs the type of patient I would be comfortable performing such surgery in because how it may effect the ability to quickly get back to that physical activity and the always unknown issue of potentially chronic discomfort with that very active lifestyle.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m wondering the cost for a nostril reduction/ Alarplasty. I’m not looking to make any changes to my tip or bridge, I’d just like smaller nostrils.
A: Thank you for your inquiry and sending your pictures. The wide flare of your nostrils requires a combined width and height reduction of them which means that a wedge of the nostril is removed. This places a scar line from inside the nostril and around the sides of the alar-facial groove. Whie these scars general do well there is always the chance of some scar visibility particularly when more natural pigment exists in the skin. Thus it is always better to think of this more aggressive form of nostril reduction/narrowing as a two stage procedure with the hope that the second stage (scar revision) is never needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I am transgender, and like many trans women I struggle with feminizing the lower half of my body. I am ectomorpbic body type and would like to maintain a supermodel structure, but I am struggling with my bodies proportions. This may seem strange but I am wondering if there can be customized implants for the iliac crest of the pelvic bone so that it gives me the appearance of a wider and more feminine pelvic bone? I see a lot of hip and butt implants, but I am wanting something that will feminize my body in a skeletal, anatomical way. Thank you.
A: Thank you for your inquiry on what is known as iliac crest implants which would create a wider pelvic bone. That is as concept that I have been working on for the very need to which you speak. This is really a cap applied to the widest part of the rim of the iliac crest. While one could argue it should ideally be made of metal, I have found no orthopedic manufacturer in the U.S. willing do so I am looking at an ultrafirm solid silicone material for the iliac crest implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was just wondering if it would be at all possible to design two testicular implants that would have a total size of 120 cc’s that could be implanted over existing testicles?
A:That is too high a volume if you are speaking of 120ccs per side. If you mean 60ccs per side then that is possible to do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a double chin, recessed chin and no jawline, so I got a chin implant, buccal fat removal (sank one side of my face, I hate it), and now my chin looks too wide and longer. My neck is short and I feel it doesn’t suit my face shape or posture.
I would like a v-shaped chin, but much like my own (since I always felt pretty except in my late 30’s my neck started melting).
The other doctor helped my jawline look at bit better, he said I didn’t need a necklift.
The doctor said a genioplasty won’t stretch my lower face too much. I want to age nicely in my neck, since my family are fat faces, necks, no jaw.
I don’t know what is the best shape for me. Please help! What do you suggest?
A: Thank you for your inquiry and sending your pictures. I am little unclear as to exactly what you are trying to achieve. You have the classic female chin problem where the implant used is too wide due to having wings and is probably positioned too low on the bone…hence making your chin wider and longer. But in trying to get a chin that is horizontally shorter (which I assume is what your natural chin is) that is also more narrow/v-shaped is going to be a problem. Implant removal is going to cause an excessive/lax soft tissue chin pad because it has been stretched out from the implant and will not magically shrink back down.
This leaves you with three options:
1) Get a new chin implant that is v-shaped and sits higher on the bone and live with the exiting horizontal projection,
2) Remove the existing chin implant and replace it with a t-shaped sliding genioplasty, or
3) Through a submental approach remove the existing chin implant and shave down the sides of the chin to a v-shape and tighten the soft tissue chin pad by a submental tuck.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a wide zygoma arch, and I’ve considering a cheekbone reduction for some time. But I’ve not read review of a single person anywhere who was happy with it. In fact I ran into many people who warn against the cheekbone reduction surgery as it causes droopy eyes and sagging skin. People end up getting face lifts and implants after it. I am attaching an image that will give you an idea of what I look like, however the result of the girl after the surgery doesn’t look great, I’m not sure for what reason. It looks bit extreme. I want to reduce just the width at the back, dont want to reduce the prominence of the cheekbone. I hope you’ll be able to provide me some insight, I have read so much on forums and all and can’t seem to understand as to why the result of this surgery are almost never satisfactory. Both my temples and jaw look concave because of my wide zygoma arch. Will the skin be saggy and eyes droopy due to lack of support and overall lack of definition even if I seek to reduce only 4mm or less at back of the cheekbone (only the arch)?
Having done some surgeries already in the past I don’t want to take up a huge risk again, kindly refer to the pic attached and let me know if it will be worth it or not. I appreciate your help, thank you so much.
A: I certainly can not tell you whether you should or should not do cheekbone reduction surgery. All I can do is provide you with my experience with the procedure.
1) It is not my experience that the vast majority of cheekbone reduction surgery patients are unhappy or require secomdary management surgery. There are many satisfied patients from cheekbone reduction surgery but they less frequently are the ones most vocal on the internet. But like all aesthetic surgeries there are risks and tradeoffs. The risks are cheek asymmetries and over/under correction. The tradeoffs are potential soft tissue sagging, often of a relatively minor degree since most patients who undergo the surgery are young with better quality tissues.
2) There are many technical variations of cheekbone reduction surgery but the most important of them is the amount of inward bony movement that is done. It can be from 1mm to 10mms. The amount of inward movement is going to affect the risk of soft tissue sagging…the more inward movement the more likely some soft tissue sag will appear after surgery. Many times this operation is done maximally (in a cookie cutter fashion) and those are the patients most likely to experience postop soft tissue sag. The reality of these statements is that the patient has to make an informed choice before surgety….how aggressive does one want the cheekbone reduction to be vs what risk is one willing to take in altering one’s natural facial bone structure onto which the soft tissues are made to be. For some patients it is often better to compromise…accept some but perhaps not ideal reduction to mitigate the postoperative risks.
3) In aesthetic surgery there is always a completely assured way to avoid the risks…don’t do the surgery. After all this is purely elective and your life will continue onward without doing the surgery. As a general observation patients that have deep seated fears about surgical risks are not good candidates for surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would a brow implant result in a lower and more straight brow ridge? Or does it simply enlarge the brow ridge.
A: Because it is a custom design the brow bone implant can be made to have any shape one wants.
Dr. Barry Eppley
Indianapolis, Indiana