Your Questions
Your Questions
Q: Dr. Eppley, I had two questions regarding clavicle lengthening. 1. How much is achievable for bideltoid width for each shoulder? I’m looking for 1.5-2cm on each shoulder. 2. How many times have you performed this surgery and what was the average amount of actual shoulder width gained per shoulder? Thanks.
A: Thank you for your inquiry. In answer to your clavicle lengthening questions:
1) The aim of each clavicle osteotomy is 2.0 to 2.5cms of lengthening per side.
2) Unlike clavicle reduction osteotomies, which I perform regularly, clavicle lengthening is a new shoulder procedure that has been performed just a few times.
3) Like clavicle reduction and shoulder width reduction, the effects of clavicle bone lengthening are essentially a 1:1 relationship of bone length:bideltoid width increase.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, When i was younger my head wasn’t that wide but with time and some jaw problems my temporal muscles got bigger and bigger because of the jaws. Now i feel like my head is a little bit ”too wide” in the temporalis place. When i press the muscles in with my hands i look way better and my skull looks more natural. I don’t know what to do because there aren’t any surgeons who do these kinds of surgeries where I live. Can you reduce the muscles with botox? and how long do that last?.
A: Botox is always a first place to start for temporal muscle reduction when surgery is not an option. It will not have the same effect as temporal reduction surgery but it will produce some modest temporal reduction effects…albeit of a temporary nature.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m looking to make my eyes a bit more symmetrical but I don’t know what sort of surgery that requires or how it might be possible. Looking for more information and potentially surgery! I’ve attached a photo of my face, front camera, and a photo of my face in selfies ! Would love to look more like the selfie (inverse) photo 🙁
A: As best as I can tell from your picture, you appear to have a left upper eyelid ptosis as the primary reason for your eye asymmetry. Eyelid ptosis surgery therefore would be the appropriate correction. Before any surgery, however, an ophthalmologic evaluation is necessary to determine if there is a medical reason for the ptosis.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,To give you a bit of historyI had hairline reshaping surgery several years ago. (I am a cis gendered female, I just wanted to make a few tweaks to my hairline) The outcome unfortunately was not what I wanted.
My hairline was significantly lower than what was discussed, and the shape given was a prominent widows peak instead of the rounded feminine hairline I wanted. I came to accept it since I thought there was no way I could ever be able to achieve the beautiful high rounded forehead that I wanted. Since then I have been embarrassed of my hairline and just wish I would pull it back into a high ponytail without showing the obvious unnatural widows peak shape. What can be done for it now?
A: While the forehead can be augmented/reshaped, that will not change the shape of the frontal hairline. The hairline can be shaped but then a forehead augmentation can not be done. Forehead augmentation and hairline repositioning are diametric procedures…forehead augmentation needs more skin as well as does trying to bring the hairline back and/or fill in the sides. The only way to concurrently accomplish both is a first stage tissue expander…which takes an ultra motivated patient to consider that staged approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a transwoman who’s looking into hip/buttock/breast augmentation surgery and your practice is one of the ones I’m considering. Your custom hip implants are what convinced me to contact you since I think the way they extend into the thighs may offer a more natural look (they remind me of my padded underwear I use to simulate hips). My goal is to achieve the curves cis-women have, that I was not born with. Can all three hip, buttock, and breast augmentation be done at the same time? If not, can two of them be done at the same time? I see you also do fat grafting and liposuction. Is that something that can be done in conjunction with implants to achieve a better look? I know the specifics of these questions (for example, whether lipo/fat grafting is recommended or not) would only be answered through a virtual consultation with pictures, dimensions, and weight. But I would appreciate if you could answer these questions to the best of your abilities. I sincerely look forward to your response as this is a procedure I’ve been very keen on getting done. Have a wonderful day!
A:Thank you for your inquiry and detailing your concerns and objectives: In answer to your questions:
1) All three implants (breast, buttock and hip) can not be done at the same time due to the recovery challenges that it poses.
2) Two of them can be done at the same time but I would not combined buttock and hips as the two because of the increased rate of complications.
3) It would medically prudent to do breast and buttock implants first for reason #4 below.
4) Despite have developed hip implants over the years they have the highest rate of complications and no alterations in surgical technique have made a substantial lowering of those risks. A s a result I remain very guarded with this surgery both in patient selection and in implant design/size. Because of these risks you want to keep this procedure isolated from others….and may even consider it not a viable option to do given the associated risks.
5) Fat grafting can be done to complement buttock or the hip regions, with or without implants. How this applied to you is not yet known to me.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I was hoping for a little insight on my overhang. I am a mom of four with the most recent two being twins. I am struggling so bad with body image after these two and battling yeast infections off and on (mainly during my monthly cycle when I seem to be way more hot). Clearly I am not in a super healthy weight range and have always struggled with weight but I have never had the overhang to go with it. Just wanted to see what my options were at this point.
Thanks!
A:There are two options for you at this point: 1) do an immediate panniculectomy/tummy tuck to get symptomatic relief and an immediate body shape improvement even though this will not produce the best result at your current weight or 2) lose some weight and then do the surgery which will allow for the best result but also prolongs the your current symptoms. You are really in the gray zone for this choice as if you were at a lower weight you would just go ahead and do the surgery vs if you weighed more you would have to lose some weight first.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I got a saggy butt because of weight loss. I’m a thin male in the upper body and have a saggy skin in my lower body especially my butt. This made me feel so uncomfortable I would like to do a surgery to remove this excess skin and make it look normal. You will find attached photos (naked) in this email. Thank you for the understanding. Best regards.
A:Thank you for your inquiry and sending your pictures. Typically excisional buttock lifts are done for overhangs of the infragluteal fold where the scar ends up along a natural crease or demarcation line. That is not the classic situation that your buttock excess presents. By looking at your own ‘pinch test’ that would place a scar line above the infragluteal fold in which I would question the scar tradeoff in such a more visible location. I can not see how I would get out the tissue excess if the excision was done in the more favorable infragluteal fold location.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What is your opinion on Lefort 2 surgery? For cosmetic purpose most of surgeons perform Lefort 1. However from what I saw Lefort 2 provides better results aesthetically. Do you preform Lefort 2 and would Lefort 1, with paranasal implants give same results as Lefort 2. Also what is down side to Lefort 2? Pic I send you is from a woman that got Lefort 2 and results are impressive to say the least.
A: If you have a malocclusion that justifies a maxillary alveolar movement than it is an option…but it still leaves behind an infraorbital rim deficiency since it can’t provide a vertical elevation to the rim only a horizontal one. That deficiency would be more apparent if she wasn’t smiling in the postop frontal view which artificially elevates the rim/cheek/lid tissues.
It would be more effective to either d a LeFort I osteotomy with implants above it or a total custom midface mask implant and avoid any form of LeFort surgery at all.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to reduce the width of my cheekbones but I don’t want to break the bones to do so. Is there another procedure that make work instead?
A:There is no other procedures to reduce the width of the cheekbones other than zygomatic or cheekbone reduction osteotomies.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was hoping to schedule my jaw implant surgery for the fall however I’ve got another procedure that may conflict.
I’m having an MSE to widen the maxilla with reverse pull headgear to attempt to fix my class 3 underbite. This may be a dumb question but the headgear pushes on the chin, will that mean a no-go for the jaw implant until after?
A: If the headgear will wrap around the chin in any fashion and apply pressure, you are correct in that it would be necessary to wait to do the jawline implant until after the orthodontic treatment is over.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m having an issue after a (second) chin implant revision, and I have an unusual question. Is it possible to design/ fashion a small “lateral” chin implant (similar to the “wing” of an extended chin implant) to support/ fill in an area of tissue loss that resulted when I recently had a medpor implant replaced with a silicone central anatomic implant?
I would compare what is happening to me as similar to what some people who have had a sliding genioplasty experience where they have a loss of tissue on the side of their chin that leaves a noticeable gap.
In my case, to make matters worse, the tissue loss is also on the side of my mandible that already has less bone/width than the other side, and it is positioned in just a way so that when I animate my face/ smile, etc… the skin pulls up and the muscle bends in a really unsightly way. It’s terrible and really bothers me.
HA filler is not hard like bone, so it just isn’t sufficient to hold the skin down when the muscle moves, and it doesn’t augment my jawline as well as an extended wing implant would.
The problem is, I’m a petite female, and so I don’t really want to go back to an implant style that has wings, as that would make my small chin look too boxy again (my first implant was this style).
If I could wave a magic wand, I would just add about a 2-3mm lateral extension piece to the current AC implant I have, but it just doesn’t seem to be possible to create such a tiny implant.
Are there solutions like this that exist, or would I need to have a custom implant made? What would something like that even cost (if you don’t mind sharing)?
Thank you so much for any advice you have!
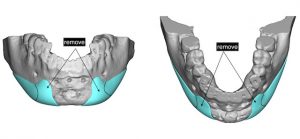 A:I believe you are referring to a lateral chin implant which can be either custom made (see attached) or hand carved from a 2mm thick sheet of ePTFE. (Goretex)
A:I believe you are referring to a lateral chin implant which can be either custom made (see attached) or hand carved from a 2mm thick sheet of ePTFE. (Goretex)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible to get nipple and areola reduction surgery? Also breast implants of my choice like Motiva or any brand I prefer?
Thank you.
A: Certainly nipple reduction can be done at the same time as the placement of breast implants with no adverse effects. One has to be more thoughtful in regards to areolar reduction as the expansion of the breast mound from the implants may place abnormal stretching on the healing areolar reduction incisions and cause wider scars than would otherwise occur.
Motiva breast implants are not currently FDA approved for use in the U.S.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello. So, after blepharoplasty only on the left upper eyelid as you can see my left eye is much more open. I would like to avoid the skin graft for aesthetic reasons. As you can see my left upper eyelid is more hollow and the crease is more higher than my right eyelid. So here is my question. Is it possible “to create more skin” with fillers on the left upper eyelid? So the crease will be lower, i mean we will make bigger the distance between the brow and the crease so, the eye will have more skin and the eye will close and be symmetrical with the right eye. I don’t want to have any skin graft. The thought of that is really devastating bcz it will be visible and i want my eye to be normal. So that is why i thought about fillers. I also thought lowering the brow surgically bcz i have seen that you have performed that surgery.
A: You are referring to whether injectable fillers can create enough stretched skin to avoid the need for a skin graft. I would doubt it but there is one way to find out…have some injectable fillers placed and see what happens. Also I do not think that lowering the eyebrow will be of much help either.
In my opinion the best thing to do is have a small skin graft placed, let it heal and then work out the skin graft later when the tissues are more healed and have relaxed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am reaching out because I have some questions regarding an uncommon procedure that I am seriously considering, and that is shoulder widening. I am a male with noticeably narrow shoulders (even after working out for some time) that measure just barely under 17 inches across which takes a hit to my confidence. Anyways….
1.) Do I qualify for this type of procedure? I am pretty young, turning 20 in a month so I do not know if that plays a factor for such a procedure like shoulder widening. As far I know, I have completely settled and stopped growing.
2.) What is the overall cost of the procedure? I have done some research but I keep getting different answers.
3.) Of these two techniques of shoulder widening, (Bone graft and Split Sagittal Osteotomy) how many inches in total width can one one expect to gain?
4.) Does one technique produce more shoulder width length than the other?
5.) Is one technique more risky than the other?
Thank you so much for taking the time to read this, It would mean so much to me to be able to work with you in the future Dr. Eppley. With all that set and done, what would be the next step in advancing?
A: In answer to your shoulder widening questions:
1) As long as one is 18 years or older shoulder widening surgery can be performed.
2) My assistant Camille will pass along the cost of the surgery to you.
3) As a general rule one inch per shoulder is achieved with either technique.
 4) Both clavicle lengthening procedures produce similar results…but differ greatly in recovery. (bone graft harvest is longer)
4) Both clavicle lengthening procedures produce similar results…but differ greatly in recovery. (bone graft harvest is longer)
5) I don’t think the two techniques differ greatly in risks. But one involves three surgical sites while the other one has only two.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is the jaw angle flare on this gentlemen achievable with an implant? I suspect he has had work done, his canthal tilt is sublime, my guess is orbital rim/cheek and jaw angle and chin combo. it is extremely rare to have a jaw angle wider than one’s head, Brad Pitt is perhaps the only other person I have seen this on.
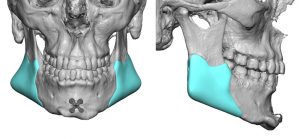 Years ago, I went to another surgeon who said he would shave my mid jaw area before attaching the posterior mandible angle porex to achieve the flared out Y look I desire. I really have no interest in shaving down my jaw angle in case of complications etc. A picture of my current jaw is below enhanced by Radiesse, One injection point to the posterior mandible down to bone. Any lower and it rounds out my face, too high on the jaw bone and it blends in with the malar I think and defeats the purpose. Attached is a custom implant from your website where I imagine mine would have to be shorter, not extending past the mid mandible and also not as tall, really hugging the edge of the jawline. Ive read about cryogels potentially being the future of filler and facial implants, but that’s not getting approved anytime soon. I grow tired of my confidence being based on the status of my jaw angle. Please advise.
Years ago, I went to another surgeon who said he would shave my mid jaw area before attaching the posterior mandible angle porex to achieve the flared out Y look I desire. I really have no interest in shaving down my jaw angle in case of complications etc. A picture of my current jaw is below enhanced by Radiesse, One injection point to the posterior mandible down to bone. Any lower and it rounds out my face, too high on the jaw bone and it blends in with the malar I think and defeats the purpose. Attached is a custom implant from your website where I imagine mine would have to be shorter, not extending past the mid mandible and also not as tall, really hugging the edge of the jawline. Ive read about cryogels potentially being the future of filler and facial implants, but that’s not getting approved anytime soon. I grow tired of my confidence being based on the status of my jaw angle. Please advise.
A: Most certainly he has had jaw angle implants as no one can look that way naturally. (we recognize that he is also biting down causing the masseter muscles to bulge) The implants would be of the widening style probably in the 15mm range if not more. They are also positioned very high on the bone almost abnormally so. Your conjecture about the jaw angle design sounds correct to me. I don’t have any idea about ‘jaw angle shaving’ combined with an implant to achieve that look which makes no sense to me.
Dr. Barry Eppley
Indianapolis, Indiana
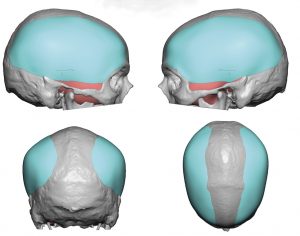
Q: Dr. Eppley, How long do skull implants last and are there any long-term side effects? And how much big cut is needed for a complete head augmentation?
A:Skull implants last a lifetime and never need to be replaced due to device failure as they are solid and do not degrade over time. Their effects are aesthetic in nature and they are not associated with any other side effects other than those that are associated implants placed anywhere in the body. The concept of ‘complete head augmentation’ can have different meanings but I will assume it is an implant that covers the majority of the skull in which case a near complete coronal scalp incision would be needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hope you are doing well! I was just curious, when you perform Adam’s apple augmentation, does the grafted cartilage heal and become one with the preexisting Adam’s apple? And just in case you’re able to answer this as well, is the cartilage is only grafted from the rib area? Thank you so much for all you do!
 A:When performing Adam’s apple augmentation there are two techniques to do so….rib cartilage (which is the only donor source that provides enough harvest material) and an implant material. (Medpor sheet) Since you asked about rib cartilage it is important to understand how rib cartilage (as well as all cartilage grafts) heal as it is very different than bone grafting from a biologic standpoint. Cartilage is an acellullar and inert tissue. Thus when it is grafted it is largely non-dynamic…meaning it just sits there. It becomes encased in scar but does not really blend in and become part of the natural cartilage bed on which it lies. Unlike bone it does not got through a process of breakdown and incorporation. Its remains fixed onto the site in which it is implanted but never becomes truly integrated into the recipient site tissues.
A:When performing Adam’s apple augmentation there are two techniques to do so….rib cartilage (which is the only donor source that provides enough harvest material) and an implant material. (Medpor sheet) Since you asked about rib cartilage it is important to understand how rib cartilage (as well as all cartilage grafts) heal as it is very different than bone grafting from a biologic standpoint. Cartilage is an acellullar and inert tissue. Thus when it is grafted it is largely non-dynamic…meaning it just sits there. It becomes encased in scar but does not really blend in and become part of the natural cartilage bed on which it lies. Unlike bone it does not got through a process of breakdown and incorporation. Its remains fixed onto the site in which it is implanted but never becomes truly integrated into the recipient site tissues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am experiencing some jowling in my lower face and my cheeks are slightly sunken. I still look okay, but tired some days. My face can seem drawn down with the mild aging. I am 51 and am trying to figure out the best solution. I am trying to decide among the following: Sculptra for my cheeks, Fat transfer to face (mainly cheeks), or a mini face lift just for the jowls. Cost is a factor, but I will consider financing. Attached is a fairly recent picture. Would you please help me with this decision. Anything you can provide information/estimate of costs would be appreciated. Thank you.
A:Thank you for your inquiry and sending your picture. You have mentioned two main areas, cheeks and jowls/jawline. In looking at the best ROE (return on effort) there is no question that the jowl tuckup procedure (aka mini facelift) would provide the greatest aesthetic benefit. This is what is creating the heaviness and drawn down appearance. You only consider Sculpra for the cheeks if surgery is not going to be an option. Fat injections is still a surgical procedure and would be done during a minim facelift so fat injections done alone seems the least likely of the options you have mentioned.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, As a male I would like to increase the length of the skin of my upper lip as I find it too short. How could this be done?
A:You can not increase the actual external skin length of the philtrum. What you can do is roll out the internal mucosa of the upper lip (V-Y mucosal advancement) which can effectively bring down the central part of the upper lip smile line. This could also be combined with a lowering vestibuloplasty, all of which is designed to bring down the inner portion of the upper lip to cover tooth show at rest.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Hello, I got a buccal fat removal and I am not happy with the results my cheeks look hollow and I would like to see if there’s something I can do about it?
A: Since fat removal is the source of your now hollow cheeks, fat replacement would be the logical treatment choice. The debate for this type of far grafting is whether it should be done by injection vs an intraoral enbloc solid fat graft placement. There are advantages and disadvantages with either approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a couple questions regarding style 2 custom cheek implants. I am scheduled to have a rhinoplasty in November 2021 and hope to perhaps pursue cheek implants in 2022.
1. How long post-rhinoplasty do you recommend patients wait before getting custom cheek implant surgery?
2. In addition, can you provide an approximate estimate for the cost of style 2 custom cheek implants? Does cost vary depending on the size of the custom implants?
3. Can style 2 custom cheek implants also augment the cheeks, or are they limited to the infraorbital rim and zygomatic arch?
Thank you!
A:In answer to your custom cheek implant questions:
1) I would allow three months after a rhinoplasty to get any form of facial augmentation surgery.
2) The cost of style 2 custom cheek implants is the same regardless of their size or surface area coverage.
3) By definition a style 2 custom cheek implant is an infraorbital-malar implant style that augments the cheeks.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, how much shoulder width reduction s possible to reduce on a man? Just 1 inch or is it more? I work as a Speleologist/Spelunker and I would like my shoulders narrower for obvious reasons.
A: Shoulder reduction surgery reduces each side by 1.0 to 1.2 inches based on the patient’s height. This is the same for men and women.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to ask you just a very quick question about brow bone reduction surgery. I have seen all articles on your website related to this – brow reduction, contouring, augmentation etc. In my case it has to be definitely just brow bone reduction (like on the first picture you send me) But would you take a look at my picture again and tell me which method could work best for me. If it´s with a complete bone flap or without complete bone flap replacement, or even if in my case 2 mm endoscoping shaving can´t be enough. I don´t know, tell me which method you think could be best for me,,, and then we can set the conversation and plan the surgery, because I´m from Europe so it´s little complicated these times.
A: The brow bones are caused by an over expansion/aeration of the underlying frontal sinus cavity…thus much of the central brow bone is ‘air’ and only a thin covering of bone exists over it. Thus only 1 to 2mms of bone can be removed by shaving since one will thereafter create a large bone defect. Shaving would only be effective in your case if you were willing to accept half or less of the current imaged result. This is why the bone flap technique is almost always the best for men.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I have done extensive research and have discovered the genius Dr Eppley! I am very impressed with his work and also the army of positive reviews online about him.
Upon research, I also discovered he is an expert in custom jaw/chin + forehead implants- both which I am very interested in. Would it be possible for Dr Eppley to find a way to enlarge and round my forehead with a custom implant?
I have been getting filler in my chin and jaw for the last few years and have LOVED IT. Now I am looking for a more permanent solution with a possible custom jaw wrap if appropriate.
 A: Thank you for your inquiry, sending your pictures and detailing your surgical history and goals. From a jaw augmentation standpoint you are correct in that a custom wrap around implant would be the ideal way to go. For females these are often more ‘petite’ type designs as one would imagine. The use of 4ccs of soft tissue filler is a good guide which translates to about 50% more volume when it is added down at the bone level and not into the soft tissue.
A: Thank you for your inquiry, sending your pictures and detailing your surgical history and goals. From a jaw augmentation standpoint you are correct in that a custom wrap around implant would be the ideal way to go. For females these are often more ‘petite’ type designs as one would imagine. The use of 4ccs of soft tissue filler is a good guide which translates to about 50% more volume when it is added down at the bone level and not into the soft tissue.
Dr. Barry Eppley
Indianapolis, Indiana
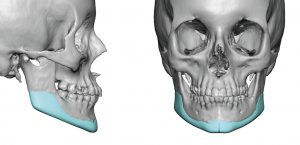
Q: Dr. Eppley, I was interested in the total head widening procedure that you perform as I have a very rounded narrow forehead and browmridge and would like for them to be widened and advanced using implants.
More specifically, I was interested in this specific model shown on the website. What would the pricing of this type of implant be? Also, is there a threshold for the amount of implant that can be squeezed in? I would require a fair bit of advancement so I’d like to know what the limits of such an implant are.
 A: The limits of any skull implant is based on its volumetric expansion. As a general rule scalp stretch can accommodate up to 125 to 150ccs in most people. The specific forehead implant to which you refer is 104cccc with a maximum thickness of 6mms.
A: The limits of any skull implant is based on its volumetric expansion. As a general rule scalp stretch can accommodate up to 125 to 150ccs in most people. The specific forehead implant to which you refer is 104cccc with a maximum thickness of 6mms.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m so impressed of your work to enlarge mouth, and I really want to do it for my mouth to make it wider (maybe 1″ would be the best).
As you can see in the picture, I have a ratio between nose and mouth around 1:1, which is not good and I can’t have a good looking smile.
A: There are two factors you need to consider in mouth widening surgery:
1) The maximum amount per side done is 7mms.
2) Scars at the mouth corners are unpredictable and there is a relatively high rate of revision of them.
Dr. Barry Eppley
Indianapolis, Indiana
Q:Dr. Eppley, For context, I am a healthy man in his early 30‘s who wants mild-to-moderate enhancement of the chin as well as the jaw angles in the lateral dimension. I am going for a strong but natural jaw appearance.
Regarding sliding genioplasty, what is the rate at which additional surgery is required, either due to functional problems (e.g. issues with talking or chewing, etc.) or inadequate cosmetic goal? Also, is it true that sliding genioplasty will yield a more natural look than a chin implant?
Regarding custom jaw angle implants, I am again curious about the success rate for the procedure. What is the rate at which they require additional surgery for any reason (e.g. needing to be taken out perhaps due to infection, revision surgery due to inadequate cosmetic goal, etc.)?
Thanks for the time you spend answering these questions. I am planning to make use of your services in the future.
A: Thank you for your inquiry and sending your pictures to which I can say the following:
1) Your chin augmentation would be best served by a sliding genioplasty because you need a combination of both horizontal and verticial dimensional increases…not because it looks more natural than a chin implant but because that is the safest method to do so with a small and tight overlying soft tissue chin pad.
2) The sliding genioplasty has a very low complication/revision rate in my experience. I have never functional issues like talking or chewing concerns as you have mentioned.
3) As for jaw angle implants the key question is whether standard or custom implants are needed and that would depend on one’s aesthetic goals which are yet to be determined. Unlike the autologous slidiing genioplasty operation jaw angle implants have a much rate of infections/asymmetries which is in the 10% range.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I am very interested in your iliac crest reduction procedure, and was simply wondering: when you shave down the hip bone what happens to the muscle attachments that connect to it? Hope this isn’t an impossible question! Thank you so much.
A:What is released when you do iliac crest reduction, which is done only in the central wing of the bone, is some the TFL fascial attachments laterally and some fibers of the external abdominal oblique muscle medially. Once the bone is reduced, these two attachments are put back together to provide some additional soft tissue coverage over the reduced bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have scheduled an appointment for rhinoplasty with you in the fall. Not sure if this is a question I should send to you but you told me to reach out with any questions.
I just want to ask if this procedure would not only improve the tip appearance but the overall nose (nostrils etc.) my primary concern is the drooping and bulbous tip but I just want to make sure I understand.
A: Most nose tip reshaping changes do affect the nostril shape, usually favorably, particularly when a droopy and bulbous tip is reshaped.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My lower lip is slightly behind my upper lip maybe 2mm, I’ve had double jaw surgery in the past and it’s definitely better than it was, but it still bugs me and I find myself biting my lips a lot because of it. I know the only way too truly fix that is with a BSSO which I will get again in the future to fully correct it. In the meantime though I’m curious would filler be able too push it out a bit too meet the upper lip?
A: I would think it would as that is how injectable filler works…volumetric expansion of the injected tissues.
Dr. Barry Eppley
Indianapolis, Indiana