Your Questions
Your Questions
Q: Dr. Eppley, Hope all is well. Attached is a zip file of some new photos for the upcoming appointment. I’ve also added the DICOM file that came with my CT scan cd. If you’re unable to view the CT photos or would prefer this sent a different way please let me know.
Also, just a quick description of what I’m considering (in order of priority):
1) Removal of some height from sagittal region. There is also a ‘bump’ at the front. Looking at posts online it could be similar to (https://exploreplasticsurgery.com/case-study-anterior-sagittal-ridge-skull-reduction/?doing_wp_cron=1647296504.2379939556121826171875
2
4) Plastic Surgery Case Study – Anterior Sagittal Ridge Skull Reduction – Explore Plastic Surgery
The anterior sagittal ridge skull deformity can be reduced by a bone burring technique.
exploreplasticsurgery.com
5) Overall the height removal would not be significant but the ridge seems to extend nearly the full length (front to back). My concerns would be surgery of that volume and scarring/placement. Additionally, I have a metopic ridge and I’m not sure if that’s a factor to consider.
6) I’m still hesitant on the thought of implants but I’m not sure if height removal would be enough and may actually make things look ‘weirder’ if some width isn’t added as well. I have a fairly thin head and I’m worried about the possibility of an implant ‘sticking out’ or not transitioning with the skull due to the amount of space available. The right side would be the priority but if the left/back is feasible I would consider it. In the zip file is an example photo, turning off the layer gives an idea of what I’d be looking for.
7) There’s a slight dip in the back that can be seen best in the third top photo (left side). This is not a huge priority but if it’s feasible with the above then I would consider.
My main concerns are scarring (location, size, healing), final appearance, whether a scalp expander is needed, if it would take numerous surgeries to accomplish, and available options if an issue occurred (i.e. implant crack). I plan to go over this during the meeting but since it’s only 30 minutes I figured a general summary may be helpful.
Thank you,
A: Thank you for sending all of your skull reshaping information to which I can say the following:
1) Your pictures show the classic aesthetic skull shape deformity which is a combination of an excess and deficiency in which there is a sagittal ridge (minor) with more significant parasagittal-parietal (upper back of the head) deficiency. Understanding this aesthetic head shape problem will allow one to have great insight into what the effects of any correction will be.
2) You have correctly assumed that any sagittal ridge reduction will have a very modest effect
3) More significant head shape changes come from either a combination of sagittal ridge reduction and parasagittal-parietal augmentation or parasagittal-parietal augmentation alone.
4) When you look at the options as detailed in #3 what becomes apparent is that you can’t have everything you want exactly the way you want it. Less surgery without an implant produces modest head shape changes. More surgery with an implant makes a much better head shape change but requires an implant to do so. Like in any other aesthetic surgery where an ideal option does not exist and it comes down to a compromise…it is all about what how much effort does one want to put into it for what type of change. It is my task to educate you as to what those changes would potentially look like as this requires computer imaging. (that will not be done until next week)
5) In the interim a diagrammatic change for both procedures is attached. The incision location for both is the same.
6) A 3D CT skull scan provides the information necessary to perform the procedures but it does not tell which procedures are the best aesthetic choice for you. That is the role of preoperative computer imaging.
7) DICOM CT scan data without a viewer program to see it in 3D is not useful.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The maxillary advancement is the original reason why I consulted with you. My plastic surgeon in Beverly Hills told me he’s the go-to guy for this and it’s what I need. Does he believe I would benefit from it? I do not mind putting off cheeks/midface augmentation until this decision is made.
A: The key questions about the potential benefits of a maxillary advancement are based on the following insights:
1) The two lower midfacial areas in which a LeFort I advancement would benefit, provided the forward movement is significant is: a) increased upper lip projection and 2) increased paranasal/premaxillary (nasal base) projection. Any midfacial area north of the osteotomy line would have no benefit and, in the long run, would end up more deficient as they are ‘left behind’. That is not an issue in you as you already recognize these upper midfacial areas would need to be augmented.
2) Whether a maxillary advancement would be worth it depends on whether its movement would be significant. (more than 1 or 2mms) That is a determination that ultimately needs an orthodontic evaluation to provide an absolute definitive determinatio as the position of the upper teeth relative to the lower teeth needs to have orthodontic tooth movement done in preparation for the surgery. (dental decompensations removed) This would worsen your current bite relationship which is typical for orthognathic surgery as this would then allow for maximal maxillary bone advancement. I can only estimate such a potential maxlllary movement which I would guess is not more than 3 or 4mms at best….seems like a lot of effort for q very modest lower midface augmentation effect…unless your bite and lower lip position is a major aesthetic issue for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in forehead reduction by hairline advancement. Would I be able to get a hair transplant in the future sometime after the surgery if my forehead is not lowered enough?
A: My concerns remain, as probably stated previously, that in a thin Caucasian female the scalp is usually quite tight with limited ability to stretch. When this is combined with a high M-shaped hairline, the concerns about how much movement will be obtained is magnified by how well the scar will turn out.
You will probably improve the M-shape but how much forward movement you will get is probably limited to 10mms or less.
This is why the ideal approach for a high hairline like yours is best treated by a first stage scalp expansion which helps overcome the previously described limitations.
But regardless of the outcome, hair transplantation can always be done secondarily. Although using hair transplants to lower a frontal hairline is frequently met with disappointing results due to inadequate density. It is better used for scar camouflage and/or filling in the recessed temporal regions.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can someone do MMA, boxing etc. after a sliding genioplasty? Is it strong enough to withstand those forces – or is it more susceptible to fracturing? Or is it relative to how much the bone was moved? i.e. 8 to 10 mm would be weaker long-term and a 4 to 6 mm movement would be stronger long-term?
Thank you for the insight!
A: When it is fully healed it will have the force resistance just like normal bone. The amount of advancement will influence how long it takes to reach the fully healed (bone consolidation) status.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I am interested in facial reshaping. I have had one consult already, but after looking at your photos, I am blown away! I now think there may be other options, better options, than what has previously been presented to me. I’m definitely interested in a rhinoplasty to correct the hump on my nose bridge and open my airway. Maybe see if you can correct my snoring? Long shot, I know, but it’s worth the ask…I have a slender face with chubby cheeks that hide my cheek bones and swallow up my jaw line. I was offered a rhinoplasty with chin implant and mini neck lift. However, I believe with your expert eyes, we could actually fix my nose, open my airways, give me cheek bones and a jaw line. I’m not sure if I need a chin implant or if having a jawline would suffice. Maybe I just need cheek lipo and not a face lift at age 39? My goal is a more symmetrical face with a flatter functional nose so my mouth isn’t open and I don’t look like I have a wattle and/or 3 chins when I see a candid photo of myself from the side. Do you think you could help me?
Thank you for your time and expertise!
A: Thank you for your inquiry and sending your pictures. The first step in any form of facial reshaping surgery, even an isolated rhinoplasty, is computer imaging. This is a critical step in helping the patient determine what type of facial changes may be beneficial. Besides identifying what facial areas may benefit by change it also allows the patient to determine the flavor of change they want. If this was not done in your prior consultation then the surgeon is merely saying what they think looks best or what they know how to do or the procedures of which they are aware.
To begin the process of computer imaging I need 3 non-smiling pictures… front, side and three quarter views. Once the imaging is sent back to you you need to interpret them by my philosophy of facial computer imaging:
The purpose of computer imaging is frequently misunderstood by patients. Computer imaging is done to help determine what the patient’s aesthetic goals are. It is a method of visual communication to help your surgeon understand what your specific goals are. It is not necessarily an accurate predictor of the final outcome. It establishes goals to aim for which may or may not be completely achievable based on human tissue responses to surgical intervention that lie beyond that of computer software can account.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I would simply like to know what would be best in fixing my deep labiomental crease (and thus reducing my chin protrusion). Im leaning towards an implant but Im worried if the implant shifts, because my main goal is to get a less noticeable chin, but I don’t want to undergo surgery so im thinking fixing the deep fold will be enough. However, I was also thinking of a fat graft to the area but from my research I’ve found that to be more expensive and unpredictable than an implant. So what do you think would be best? I looked into fillers too but I really want permanent results as this is a pretty big insecurity of mine.
A: Thank you for your inquiry and sending your pictures. Essentially what you are asking is which is better….a chin reduction (not an implant as that makes the chin bigger not smaller) which treats the actual source of your aesthetic concern or a labiomental fold augmentation to try and camouflage the protruding chin. (see attached illustrations)
If the goal is effectiveness then the chin reduction approach provides a much better result long term. If the goal is the lowest cost and degree of invasiveness then fat grafting to the labiomental fold would be the choice. Unlike chin reduction you can actually test the labiomental fold augmentation by injectable fillers and get an immediate answer to that approach that is non-surgical and completely reversible.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a few questions about your approach to genioplasty. I sent your assistant my picture and question about having genioplasty plus implant. She sent me your reply with a morphed picture, along with your assertion that a geneoplasty alone should be enough considering all I should need would be 12mm or so of advancement. I also posted a similar question about my chin with the same picture on Real Self, to which you also replied explaining a bit more about the geneoplasty plus implant procedure.
As far as I can tell, you are the only doctor offering genioplasty movements of above 12mm. Most surgeons consider 8-10mm the maximum, with a handful suggesting 12mm may be possible:
1. Why is there such a disparity between what the numbers of 14-16mm you have achieved, and the vast majority of surgeons which seem decidedly reluctant to perform such a large movement? Is there anything different about your specific method that others don’t perform? I understand the degree of possible projection being due the thickness of the bone.
2. When considering the addition of a chin implant to further augment the projection, what are the limits?: As I understand it from what I’ve read in your articles, there’s a limit to the amount the soft tissue can stretch horizontally in a single operation — how much projection can you achieve in one go with genioplasty + chin implant? Additionally, is there similarly a projection limit if you were to instead consider adding an implant once the genioplasty had healed? (For example, could you have a 15mm genioplasty and then 6 months later [or however long it takes to heal] add a large implant like the Terino Square Style Chin 1 at 11mm?)
Given your initial email response and then what I read as somewhat of a conflicting one on RealSelf, I’m unsure of what the recommendation would be for my case. I have attempted to measure my degree of deficiency with a ruler — angling a small ruler along my jawline and measuring from the base of my chin to just slightly behind my lower lip — and deduce from that that I would need a horizontal advancement of about 2.5cm: a figure widely off from your recommendation of around 12mm, so I presume my rudimentary attempts at measuring myself are inaccurate. I have attached my picture again below.
Many thanks for your time.
A: In answer to your sliding genioplasty questions:
1) I can only speak from my own sliding genioplasty experience and techniques. I suspect that most surgeons view how much forward movement is possible based on the need for extensive bone contact between the two chin segments. That may have merit if one is using non-bone grafting techniques. I learned long ago that all sliding genioplasties create an unnatural shape to the chin (step off) and making the effort to graft these created defects using tissue bank chips or block bone grafts is a useful technique. It is important to understand that the more the chin bone is moved forward the greater these bone defects will be and the more these types of bone grafts are needed.
2) When it comes to the need for very large chin movements, it is important to make the bone to most of the work in achieving it. These can take two basic approaches; 1) lessen the sliding genioplasty amount (10mms) and immediately place an implant overlay, or 2) maximum the chin bone movement forward (14 to 20mms) and plan a second stage implant overlay later if needed. (6 months or more) Whether this is using a standard or custom design chin implant remains to be determined. The key to an immediate or delayed chin implant overlay is that the implant can not exceed 1/3 in horizontal projection over what the bone movement has achieved due to the limits of soft tissue stretch.
Each patient’s case must be assessed by computer imaging to determine which approach is best and how much horizontal projection is really needed.
What I do know is that your description of adding an 11mm chin implant secondarily, regardless of the amount of chin bone movement, is neither possible nor advised.
Lastly I assume your ideal location of chin projection is the often quoted vertical line dropped down from the lips. I would question whether 25mms would be the correct number to achieve that but what I do know is the following and I will assume for the sale of discission that 25mms of projection is the goal:
1) A 25mm custom chin implant would never fit.
2) A 25mm sliding genioplasty is not possible either…both due to the limits of soft tissue chin pad stretch.
3) Therefore the best approach is maximum whatever the chin bone can be moved and then evaluate later whether any more projection is really needed. What usually fits after such efforts is probably a 5mm implant on the end of the bone placed through a submental approach. Custom implant design is best since the goals would be to widen the chin, cover over any residual step-offs and provide a square shape per your description.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can I use skull bone grafts for midface retrusion augmentation. I know you are a renowned surgeon to use midface implants but I want to avoid synthetic material because I am very sensitive and want to avoid any risk of infection.
You can use a lot of bone grafts from the cranium to augment the complete middle face including: malar, premaxillary, infraortital, lateral orbital rim, and front of zygoma ..so complete front of midface. Any information about the procedure possibility please
Many thanks
A: Split thickness skull bone grafts can certainly be done for most of the midface areas. The infraorbital area is the tricky one due to thin eyelid tissue and the high risk of palpable or visible contour irregularities. Also the key is making sure the donor sites get ‘reconstructed’ with some form of cement so you don’t have a lot of skull irregularities as this will result from harvesting split thickness harvests on the top of the skull behind the hairline.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thank you for your detailed answers to my questions regarding sliding genioplasty; I am now much clearer on the process.
I am also considering two other procedures: something to solve my excessive scleral show and also a lip lift. Similarly to with the chin surgery, I had a couple of preliminary questions prior to scheduling my consultation with you (just so that I am informed on the procedures so I can discuss them with you and make the most of the consultation).
Regarding the lip lift: It would only be a very slight change I wanted — about 3mm to shorten my philtrum a bit to put my upper and lower lip in better proportion (philtrum to upper lip is currently about 1.8cm).
Firstly, is there much risk of my nose nostrils dropping down? I have heard this deformity can occur.
Secondly, is there a risk that my lips would remain permanently parted at rest (showing my teeth)?
As far as I can tell, the aforementioned issues most often occur when a large amount of tissue is excised from the philtrum. I have again attached my beardless side profile so you can see my philtrum.
Regarding the scleral show: I understand this to be a complex issue to solve, potentially involving both orbital rim implants (I have attached a couple of images (front and side) — I’m unsure whether I have negative orbital vector) and what I assume is either a canthopexy or canthoplasty plasty.
I have read your article specifically on canthopexy, and the results you displayed on the lady in the picture did indeed seem to have reduced scleral show — but you and most other reputable surgeons seem to say neither canthopexy or canthoplasty is enough to rectify the problem. What is the true solution to scleral show? Can canthopexy or orbital rim implants ever be enough on their own?
A: In answer to your questions:
1) A subnasal lip lift of 3mms will cause neither upper lip incompetence or nostril deformations.
2) You do have a marginal negative orbital vector which would also explain why your scleral show is very minimal by comparison to many other scleral show males. If the modest infrarorbital rim deficiency or if you have no desire for a higher cheekbone look, then a lateral canthoplasty with lower eyelid space grafts should suffice.
Dr. Barry Eppley
Indianapois, Indiana
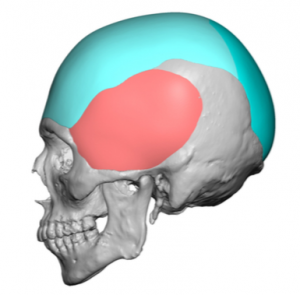
Q: Dr. Eppley, I got my custom skull implant for the beck of my head last December and you did tell me after a while that my swelling would go down. I’ve definitely noticed some things, and wanted to know if he did anything for the more bottom part of the back of the head! I made some marks as to kinda where I want it. Thank you kindly:)
 A: Thanks for the longer term followup. The diagram you have shown illustrates a common misconception of where the occipital bone actually ends on the back of the head. The bottom end of the skull on the back of the head is actually at the same level as the brow bones are on the front of the skull. This places the end of the bone at the same level of the top of the ear…much higher than most people think. (see attached diagram)
A: Thanks for the longer term followup. The diagram you have shown illustrates a common misconception of where the occipital bone actually ends on the back of the head. The bottom end of the skull on the back of the head is actually at the same level as the brow bones are on the front of the skull. This places the end of the bone at the same level of the top of the ear…much higher than most people think. (see attached diagram)
At the end of the occipital skull bone attaches the neck muscles. So if a skull implant design extends below the bone unto the surface of the muscle, which can be done, there is always the risk of potentially causing some discomfort when one extends their head backwards. I suspect this risk would be reduced/obviated if the skull implant had a softer edge. (lower durometer implant material)
Looking at your current skull implant design at 125ccs, much of its volume was desired at the very flat upper back of the head, and it has done a good job of solving that issue. Even if we had wanted to augment the bottom part of the skull, including below the bone edge, we would not have been able to do so originally as that total implant volume would have been in the range of 175cc to 200ccs…a volume beyond what your scalp stretch could initially accommodate.
With an indwelling skull implant it acts as a scalp tissue expander which now would permit a new skull implant design that could provide coverage/volume in your desired areas.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I am looking to get facial masculinization surgery. The aspects I dislike the most are how “flat” my face looks from the side and that I don’t have a very broad brow from the front which imo makes me seem like my face has a very “open” and “feminine” look. I also dislike that my chin is weak and narrow. Looking extensively around your website I feel as though I look like the “after” for the “facial feminization” and need the reverse.
A: Thank you for your inquiry and sending your pictures. I have done some imaging looking at potential changes to the brow bone, cheek and chin/anterior jaw area. The brow bone and cheek augmentation are fairly straightforward using custom brow bone and infraorbital-malar implants. The chin and lower jaw has more challenges/options to it because the primary problem is the lack of vertical height and width. (with some slight need for horizontal projection) A custom chin implant would provide some height and good width but the soft tissue chin pad is only going to permit so much lengthening to be done as its ability to stretch over an implant is limited. Conversely a vertical lengthening sliding genioplasty allows much greater length to be created because the soft tissue chin pad remains attached to it as it is brought down. However it has no ability to add width unless implants are added to the sides of it. As you can see there are several options for your chin each with their own advantages and disadvantages.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, is there a way for a custom implant to reduce back flatness of head and frontal flatness. I could benefit from a little convexity. Is there also a way minor changes could be made to reduce flatness? I just want a lil bit of change in appearance. Thanks
 A: Thank you for your inquiry. I believe what you are asking is whether a back of head implant can be combined with a front of the head (forehead) implant. That answer would be yes. The question then becomes would this be a connected implant from front to back or a two piece implant leaving the central area on the top of the head uncovered. That question is yet to be determined.
A: Thank you for your inquiry. I believe what you are asking is whether a back of head implant can be combined with a front of the head (forehead) implant. That answer would be yes. The question then becomes would this be a connected implant from front to back or a two piece implant leaving the central area on the top of the head uncovered. That question is yet to be determined.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, i had a LeFort 1 with maxilla impaction and slightly advancement. Now Im left with a potruding mouth area, a more upturned nose and a longer upper lip. My biggest concerns are the upper lip inclination(more convex and straight) and the more upturned nose. Can a rhinoplasty with tip derotation influence the inclination of the upper lip, so its more concave after? What procedure do you recommend based on the picture for a better upper lip – nose relationship?
Thank you very much and best regards.
A: The anatomic cause of some your midface concerns is that the caudal septum and anterior nasal spine is more forward than it was which can push the base of the nose forward (opening the nasolabial angle) and the tip of the nose upward. The degloving of all the soft tissue attachments to the bone, which is necessary to do the surgery, and the movement of the maxilla forward creates a long upper lip and contributes partially to the mouth protrusion.
In improving the nose-lip relationship, the anterior nasal spine and base of the pyriform aperture bone must be reduced through an intraoral approach. This will decrease the open nasolabial angle. The tip of the nose, however, will not just automatically derotate. Infralobular onlay grafts or an interpositional cartilage graft between the dome and the caudal septum are needed to push the tip of the nose back down.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been looking up on your clavicle lengthening procedure online and am seriously considering it. I am a 22 year old man with very short clavicles and your procedure is the only hope I have left regarding my shoulders. I am have been working out for many years and my narrow chest always disheartened me. I had a couple questions regarding the procedure.
1) Is is possible to undergo non-bone graft clavicle lengthening and lengthen the clavicle by >= 2 cm? I read from your blog that with the diagonal cut pattern the max is 1.8 cm but with the modified sagittal split it is possible to get more.
2) If the bone-grafting technique is chosen and when the donor bone extracted from the leg, how long does it take for the leg to heal? Also, how big is the chunk of bone taken from the leg? Is the leg bone completely split into two?
3) How long after the surgery are patients allowed to go home? How long after the surgery can the patients perform activities like raising the arm, etc.
4) I want to take the plates out in the future after the recovery is complete. However, I am unsure if I will be in the united states at the time. Is it safe to go to other orthopedic doctors to remove the plates?
5) How much do you expect the surgery would cost. Around $50,000? Around 100,000? More? I am hoping to save up for this and wanted to know how long it would take for me to be able to afford it.
Thank you so much for taking your time to read this. It would mean so much for me to finally be able to work with you in the future regarding this procedure.
A: In answer to your shoulder widening/clavicle lengthening surgery questions:
1) My current method of shoulder widening is a lengthening osteotomy of the clavicle which doesn’t use a bone graft.
2) While a bone graft is not used as described in #1, taking a 5 cm long segment of the fibula does not require it to heal by regenerating bone. The fibula bone does not need to be intact for walking or running.
3) One can go home after the surgery when they are physically able to travel. That is influenced by a variety of factors including are they here by themselves, how are they getting home, where is home etc. But as a general rule 5 to 7 days is typical.
4) An orthopedic surgeon would be able to remove the hardware secondarily.
5) My assistant Camille will provide the cost of the surgery to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve been looking at your Iliac crest implants for pelvic plasty, and wanted to get some details. Firstly, how much would the surgery and implant cost? Where is the surgery done?
A: In answer to your iliac crest implant questions:
1) Titanium iliac crest implants can currently only be done in South Korea. They are not yet approved by the FDA for use in the U.S. That cost is $20,000.
2) In the U.S. I am currently working on ultrahard solid silicone implant equivalents which is capable of being placed due to it being a custom made implant for each patient. To date I am waiting to do the first such patient. Such surgery is done in a surgery center with an overnite stay.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a flat (and somewhat asymmetrical) back of the head since infancy. I would like a custom implant to correct this. I would also be interested in procedures to reduce the width of my head if possible.
A: The back of the head can certainly be augmented with a custom skull implant. While the sides of the head can be reduced that requires vertical scalp incisions along the posterior temporal line. Thus the options are:
#1 Custom Back of Head Skull Implant placed through the traditional low horizontal scalp incision with NO side of the head reduction
#2 #1 with Bilateral Side Of The Head Reduction done through paired vertical scalp incisions. (no horizontal scalp incision needed)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, First off I’d like you to know I was born a female as I think I would benefit from brow bossing reduction. After having rhinoplasty I noticed my brow bone more prominent because my nose was now more feminine it stood out more. Also I’m considering sub mental and possibly corner lip flip and not sure If you do packages because I may want a brow lift or some type of lift as well since incision already for brow bossing. Liposuction neck and jaw only if it tightens skin, Vaser lipo or plasma I believe. I’m 38 years old so I will be getting procedures in about a year or so from now, I’m hoping to not have to go out of the country. I may want to add more procedures if package is reasonable. Thank you for your time! The last picture is with botox and threads and trying to make skin better.
A: Thank you for your inquiry and sending your picture. If I understand your desires correctly, you are interested in the following procedures:
Brow Bone Reduction
Browlift
Neck and Jawline Liposuction
Corner Lip Lift (Flip)
To which I can make the following comments:
1) All of these procedures can be performed concurrently
2) A browlift can be performed at the same time as that of brow bone reduction without any increase in the forehead length if it is done through a hairline incision. Any incision behind the hairline will result in a vertical forehead length increase…which may be an aesthetic disadvantage based on your current forehead length which I can not determine based on the current picture which has cut off the face at the eyebrow level.
3) Whether any form of liposuction provides adequate skin tightening depends on how much skin tightening is desired. The fact that you have had a threadlift already suggests that more skin tightening is needed than what most forms of liposuction can provide.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, for people who already had a masseter muscle retraction after jaw angle implant removal, can they have a new jaw angle implant placed even with a retracted masseter muscle?
A: Masseter muscle dehiscence does not preclude secondary jaw angle implant placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Do you do calf implants? I was hoping to add 2-3 inches.
A: Double calf implants (inner and outer heads) can have a significant lower leg augmentation effect. But I would be cautious about trying to put a specific circumferential number increase on it as that is not completely predictable and depends on a number of factors including the thickness of the muscle/soft tissues, the size of the implants and the stretch of the soft tissues to accommodate the size of the calf implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an indented scar on my left upper buttocks. I’m thinking of having a BBL. Can a BBL make it look better. I also notice anytime I press on it it’s painful. I have had this on me for more than 10 years.
A: With an indented scar that is adhered (fixed to the underlying tissues), you can have BBL surgery but it will not make the indented scar disappear. It may make it look even more indented or may soften it a bit but the pronounced indentation will remain. To really improve the indentation it should be treated before a BBL by excision of the indented scar and the placement of solid fat graft underneath it. This is the only way to remove the buttock indentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, I’m a 23 year old female and have a very masculine and odd-shaped forehead. My forehead is bumpy (horns), uneven, my brow bone sticks out, and my hairline is further back than it should be. I was wondering if you could perform both forehead reconstruction/contouring and hairline lowering/hair transplants. Thank you!
A: I can perform simultaneous bony forehead bone contouring and a vertical forehead reduction by frontal hairline advancement. (but not by hair transplants)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’d like to learn more about the trapezius reduction surgery. I have never seen this surgery offered anywhere else. My questions are as follows:
1. Why are there so few surgeons offering it? Is it high risk?
2. I have seen Botox offered much more frequently. Have you found Botox to be ineffective in some patients? If yes, could you elaborate as to why it may not work ? Or does Botox work but there are patients that want something more permanent? I just had my first round of Botox for trapezius reduction. I was told it usually takes 2 or 3 sessions to see an aesthetic change. What are your thoughts?
3. Is general or twilight anesthesia needed?
A: In answer to your trapezius muscle reduction surgery questions:
1) It is a very rarely requested procedure. Thus there is no reason he vast majority of plastic surgeons would consider doing it. It is not a high risk procedure.
2) Like any muscle Botox injections, if enough units are given and done enough times, will have some reductive effect…albeit only temporary. But it is a good place to start.
3) The surgery is done under general anesthesia.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, we had discussed about my skull augmentation project a few months ago. I am coming back to you because I would like to make my project a reality.
During our last exchanges, you indicated that I would need a scalp expander operation first and once this step is completed, the custom skull implant could be placed. I have several questions about this:
What would be your available dates to do this first procedure for me?
Can I swim in the pool and in the sea with the scalp expander device?
Is the device visible? Is it compelling to fill it every day?
Do you have pictures of the device installed on someone?


 A: i believe the basic concept was that in order to assure that you could achieve the amount of augmentation that you have shown on your one pictures a first stage scalp expansion is necessary. The scalp expander and its indwelling port are under the scalp so activities such as swimming await the healing of the small incision used to place it but can be done with it in place.
A: i believe the basic concept was that in order to assure that you could achieve the amount of augmentation that you have shown on your one pictures a first stage scalp expansion is necessary. The scalp expander and its indwelling port are under the scalp so activities such as swimming await the healing of the small incision used to place it but can be done with it in place.
The 3D CT skull scan is exactly what is needed to eventually fabricate a custom skull implant. The scan by itself does not tell us how to make the implant design but is the foundation on which it is designed. The frequency of inflation is usually every 2 to 3 days it that depends on the time between its placement and the date chosen as well as how much inflation volume is needed. The presence of the scalp expander is not usually detectable until its later stages of fill but also depends on one’s hair style as well. The goal of scalp expansion is to create the same volume as that needed of the designed skull implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Was wondering about the “Hip Widening By Iliac Crest Bone Implant Augmentation” procedure. I’ve been following the procedures approval process in South Korea for a few years now and was wondering how you feel about the results of your patients that you’ve performed this procedure on.
My worry is that it would make my hips “top-heavy” so to speak, by make the top part of the hips wide without also widening the bottom part.
Was wondering your thoughts on that, especially for a patient that is transgender like myself.
Thank you!
 A:The key to iliac crest implants, or any aesthetic surgery, is to determine BEFORE surgery what the effects they may create and see if it provides improvements, creates an unappealing change or just creates another problem. There is a fine line between augmenting the outer pelvic rim (the very top of the hip region) and the more well known soft tissue hip region below it. This is why computer imaging always needs to be done on each patient looking at augmentation of the iliac crest region alone, augmentation of the hips below or a combination of both. This is simple enough to do using front and back pictures of the torso.
A:The key to iliac crest implants, or any aesthetic surgery, is to determine BEFORE surgery what the effects they may create and see if it provides improvements, creates an unappealing change or just creates another problem. There is a fine line between augmenting the outer pelvic rim (the very top of the hip region) and the more well known soft tissue hip region below it. This is why computer imaging always needs to be done on each patient looking at augmentation of the iliac crest region alone, augmentation of the hips below or a combination of both. This is simple enough to do using front and back pictures of the torso.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering issues regarding lip incompetence and other facial features.
I think I got lip incompetence due to allergies or maybe dust mites?
I want to fix my lip incompetence because I have breathing problems and I cannot breathe through my nose, only through my mouth.
I also wanted to know if there’s any procedures to reduce one’s philtrum length? Is it scar-free?
I sent you a front and side profile to examine.
Thank you so much for your assistance.
A:Thank you for your inquiry and sending your pictures to which I can make the following comments:
1) Your lip incompetence is caused by your lower jaw and chin. There is no enough bone support for the lower lip. It has nothing to do with allergies, it is an anatomic problem. The only way to effectively treat it is with either a major lower jaw advancement procedure or an isolated sliding genioplasty procedure. (see attached imaging)
2) The distance between the base of the nose and the upper lip can be reduced by the well known subnasal lip lift procedure. This results in a very well concealed scar line under the base of the nose. While not scar-free the more important tradeoff to consider from this procedure is whether the increased fullness of the upper lip would be acceptable. (see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am desiring a Brow Bone Reduction. Based on my x-rays which brow bone reduction technique is best for me?
 A: Your lateral brow bone x-ray shows clearly that any effort at brow bone reduction can only produce meaningful results with a bone flap setback technique. Only a few millimeters of reduction can be obtained by burring alone.
A: Your lateral brow bone x-ray shows clearly that any effort at brow bone reduction can only produce meaningful results with a bone flap setback technique. Only a few millimeters of reduction can be obtained by burring alone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have significant facial asymmetry whereby my mandible is less developed on the right than on the left. This causes the left side of my face to look “empty” and flat, with my chin pointing off to the left. I am hopeful that this can be improved with a jaw implant. The problem bothers me a lot, and makes me camera shy. Improving my facial balance would mean a lot to me, and I would be very grateful for a chat with you about this.
A: Thank you for your inquiry and sending your pictures. In mild cases of jaw asymmetry (5mms or less from chin midline) a total jaw implant can be a very effective procedure to correct the asymmetry as both sides of the jawline and chin are built out differently to make the chin/jaw symmetric from the front view. But when the jaw asymmetry is more significant with the chin shifted more than 5mms from the midline as in your case the build out between the two sides can make the chin and jawline too wide for your face to achieve symmetry. Thus in your case you use a sliding genioplasty to shift the chin back to the midline and concurrently place custom jawline implants to build up the two sides which merge into the repositioned chin bone by preoperative computer design.
These recommendations are based on a picture analysis. But ultimately review of a 3D CT scan and looking at various chin bone changes and implant designs will determine the best treatment plan for your face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, After you put a temporal implant on the muscle, will I feel discomfort when chewing?
A: Placing a temporal implant under the fascia and on top of the muscle will not cause any long-term discomfort with mastication. Most patients will experience some tightness on mouth opening right after the surgery due to the muscle trauma but this is temporary. The best way to get over the tightness is to stretch and eat and chew normally.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have had some minor openings of my armpit incisions after getting pectoral implants. Is this normal?
A: This is perfectly normal with axillary fold incisions and is not rare after pectoral implant surgery. They are located in a tough spot to heal and often will develop some varying amounts of incisional edge separation which begin to appear 2 to 3 weeks after surgery. The proper strategy is to let them go on to heal secondarily. (from the inside out) No oral antibiotics are needed and trying to reclose these will fail 100% of the time. The body will naturally heal these up in 2 to 3 weeks. I would continue to shower and don’t worry about getting them wet. They may develop a little bleeding from time to time which is very normal as granulation tissue fills up the wound openings. Once the granulation tissue develops up to the wound edges the incision will close over it very rapidly. Your current wound care strategy is perfectly fine. This is just a very minor bump along the recovery process.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a custom occipital skull implant. My questions are:
Who will perform the procedure?
What could go wrong?
What is the chance of having to repeat the procedure?
Are the sutures self absorbing? How long does it take to heal?
Can one place ones head on a pillow where the sutures are?
Can one bathe and comb hair?
What are the chances of infection?
Do I need to come back for a follow up?
Would there be any facial swelling?
How soon can I return to my work/daily activities?
Is it safe for radiography?
Is it visible in an x-ray?
A:In answer to your custom occipital skull implant questions:
1) I perform the procedure exclusively.
2) When you say going wrong what you mean is what are the known risks and complications of the procedure which in skull implants is always infection, asymmetry, visible edging and size. (too big or too small)
3) All skin sutures used are resorbable which takes 2 to 3 weeks to go completely away.
4) There are no restrictions are head positioning after the surgery.
5) One can shower the next after surgery and shoer and wash their hair 48 hours after surgery.
6) I have never yet seen a custom skull implant infection.
7) All followups are done in a virtual manner.
8) Some patients may experience facial swelling in the temples and eye area which resolves in 7 to 10 days after the surgery.
9) There are no physical activity restrictions after the surgery. You do what feels comfortable.
10) All skull implants are safe for any form of postoperative imaging.
11) Custom skull implants are invisible in a plain x-ray, seen as a radiopaque layer in 2D and MRI scans and will be seen as an actual implant in 3D CT scans.
Dr. Barry Eppley
Indianapolis, Indiana