Your Questions
Your Questions
Q: Dr. Eppley, Hello, I had a chin burring procedure intraoral approach in November 2020 but when the swelling went down my chin was noticeably long and flatter, my main concern is that the tissues are now drooped and filler has made it less unsightly but still drooped and long, smiling makes it worse. I would like to discuss excision and tightening of the chin pad to help this issue, thank you!
A: Chin reduction by intraoral burring is always a poor treatment choice which creates exactly what you have…a flatter wider chin with soft tissue chin ptosis which is why it looks longer. Why surgeons continue to do this approach to chin reduction when this is an expected outcome is a mystery to me. It can now only be improved by a submental chin pad excision/tuck now.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have untreated plagiocephaly which has caused several asymmetrical features of my face and head And I’ve only started to notice as I got older.
The right side of my face is pushed forward and the left side is pushed back affecting my eyes, cheekbones, ears, jaw and head. The right side of my jaw appears smaller and higher up whereas my left side of my jaw appears larger and further down. My right side eye appears larger and positioned normally whereas my left eye is slightly slanted more and pushed further back making it noticeably asymmetrical. My right side cheekbone is pushed further out compared to my left. The left side of my head is pushed further back and sticks out noticeably looking at me from the front, whereas my right side doesn’t stick out but is flat at the back , my right ear is placed further forward compared to my left. How many of these problems would you be able to fix please and make me look as normal as possible I know if I was to get most of these asymmetrical features fixed it would be a long expensive process but I’m willing to fly over for however long it takes.
A: Every skull and facial shape abnormality that you have described is very typical in plagiocephaly. Potentially every one of them can be treated/improved to varying degrees. The first step is to establish a treatment plan for them based on your priorities. I would make a list of the most to least bothersome of these craniofacial features and then we will match that up with a 3D Craniofacial CT scan to create a surgical approach to your plagiocephaly concerns.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have had a testicular implant since 13. There is a large size disparity between my real testicle and the implant.
I am about to have a urologist insert a larger implant. In researching the Coloplast, the largest size is not even close.
What are my options?
A: The beet approach would be to have a custom ultrasoft silicone testicle implant made that matches the other side in size. Given your statement of ‘the largest size is not even close’ would indicate the need for a custom implant design approach. Since the largest saline testicle implant is 4.5ms and the largest silicone testicle implant is 5.0cms, the need for a custom testicle implant design is obvious.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a botched genioplasty and I am wondering if you could fix it? My doctor said I had to wait 6 months for a revision but 1) I really do not trust him to do the revision and 2) I have seen other people have revisions/reversals before 6 months. Thank you.
A: What type of bony movements were done in the sliding genioplasty and what concerns are there now? This will guide how you would revise your genioplasty. But it can be done anytime before 6 months as what matters is whether you have a clear idea as to the changes you want. The timing is not based on how well healed the bone is.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, i want to know after a surgery like skull reshape how do you feel your head because I’ve had some surgeries and all the zones of the cut feels like electricity and numbness. It is the same for the head?
A: In my experience skull reshaping patients will experience some temporary scalp numbness which fairly quickly returns to normal in a month or two after the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Can The Plates and Screws and Hydroxyapatite Granules Be Removed After A LeFort I Osteotomy Surgery?
Q: Dr. Eppley ,I am writing to you because 3 years ago I had Lefort 1, BSSO and a cheekbone augmentation with hydroxyapatite granules.
Since this year, I have noticed the cheekbone (implant/granules) grew much larger, mainly on the left side. It has been getting bigger still and it protrudes much more from the side. Especially in the last 6 months, it seems like the “implant” is migrating upwards towards my eye; or a new bone layer is growing near and/or around my eye socket. My left eye is closing up as new bone grows, or hydroxyapatite moves underneath and on de outer corner of the eye as well.
Another issue is that my face, especially in my cheek area, has been swelling up slowly over the past year as well. On the upper jaw, the area where the plates and screws were placed, it feels sensitive and is more swollen. I believe this is due to an infection of either the plates or the implant.
Could there be new bone growing on and around the hydroxyapatite implant, years after placement?
Could this be the reason for the possible plate infection?
I am very worried about what is happening in my face, and I was hoping we could have a consultation about the removal or at least reducing of the hydroxyapatite implant and the plates and screws.”
A: The first place to start is to get a 3D CT scan of your face in which all metal hardware as well as the sites of HA implants can be seen. This will then provide a guide for surgical removal. There is no indication that you have any infection as this is not how infections present nor would they occur in such a delayed time period. This is all due to scar tissue buildup and how the body has responded to the HA granules.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, thank you for all your information about skull reshaping surgery that you provide which is very useful for us. I would like to know if it is possible to reduce the width of a human skull by reducing the thickness of the parietal bone by about 3 to 5 mm on each side of the skull knowing that the parietal bone has a thickness of 1.7 cm on average and if so, what are the risks.
A: A parietal bone skull reduction of 3 to 5 mms can be effectively achieved without significant risk…other than the aesthetic compromise of the fine scalp scar line (incision) required to perform it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a sliding genioplasty to advance my chin 6mm forward 7 weeks ago. I know that I am still early in the healing phase but I hate my chin so far and I feel like it’s not so swollen anymore. It makes my face seems a lot longer and narrower. From a 3/4 view, it looks too pointy and doesn’t match my face. I know that with facial cosmetic procedures it can be hard for patients to accept their new faces but I feel like I won’t ever like this chin. I am thinking to reverse it (3-4mm backwards) but I would like to know when is the best time to get it done. Some surgeons say that it’s best done 6-8 weeks after the surgery or that I should get it done between 3 and 6 months while other doctors say that I should wait 6 months for the bone to heal. My surgeon said that a new surgery so early is too risky and that it could end with a bone necrosis. I am ready to wait a few months because I don’t want to take a hasty decision. When is the best time to get it done ? Is 4mm too much? I am 18 years old, I don’t want my skin to sag. Thank you
A: At 7 weeks out you can do it anytime now. The so called risk of bone necrosis is a non-factor in my opinion and experience. Just get it done as soon as you can at this point after surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am very interested in the procedure that I see you are an expert in, forehead augmentation with custom implants.
My question is the following, I have a very backward sloping forehead, and I want to increase considerably in volume that area, I have read that in the case that it is required and the patient wants something much more significant should be implemented an additional procedure (tissue augmentation, extension), I think that would be my case. I want to increase my forehead about 5 cm of volume approximately, with temporary extensions and completely cover the eyebrows.
Will it be possible to augment to that extent? Up to how many centimeters will it be possible?
I attach photos of what my forehead looks like and how I would like to have it.
Best regards, I look forward to your answer!
A: Thank you for your inquiry and sending your pictures. You have made two correct assumptions in regards to your forehead augmentation goals:
1) The desired amount of forehead augmentation is going to require a first stage scalp expansion and
2) When you add that much change in the inclination of the forehead the implant must, to look natural and blend in with the rest of the head shape, wrap around the sides (temporal regions) of the head. In essence this forehead implant design would really involve the entire front half of the skull.
You have made one incorrect assumption, that amount of forehead augmentation is profile is closer to 10 to 15mm of projection not the 50mm or 5 cms which you have stated.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My head is flat on the back and underdeveloped on sagittal and frontal, and it’s been troubling me and cause I h me depression just being aware of it 24/7. I got a few questions about the procedure. 1. Is it bone cement you’ll be using for skull reshaping surgery, or silicone padding? 2. Is possible to go through one anesthesia and have three incisions and reshaping my forehead, back of my head and my sagittal area in one procedure? 3. I’m a trans women. Does skull reshaping surgery count as part of my Facial Feminization surgery, and if so could that be covered by insurance?
A: In answer to your skull augmentation questions:
1) Only a custom made solid silicone skull implant can create effective 3D skull augmentation changes.
2) Yes it is possible in a single surgery to reshape/augment numerous skull surface areas…provided the volumes being added do not exceed the stretch of the scalp to accommodate them. If the scalp’s ability to stretch is questionable or there is absolute certainty that it can’t, then a first stage scalp expansion procedure is needed.
3) We do not accept or process insurance.
4) To accurately provide the cost of #1 or #2 (one vs two stage skull augmentation) I would need to do some computer imaging on your pictures to determine what your precise skull augmentation objectives are.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Does the burring method, which, from what I gathered, removes the outer layer of the skull, result in a weaker, more vulnerable skull which can increase the risk of hurting one’s head and brain (cracking, piercing skull, etc)?
A: Removal of the outer layer of the skull as is done in skull reduction surgery does not make it more susceptible to injury due to the double layer cortical bone that comprises the full thickness of the skull.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about your stance on the ability of infraorbital rim implants to marginally effect scleral show on the lower lids.
I’ve researched this topic quite a lot, and your name always pops up within discussions surrounding it. I’m a bit confused, though, as in some posts — whether it be on your blog or realself.com— you suggest that if orbital implants have enough vertical height, they can help drive up the eyelid slightly and reduce scleral show. However, it seems you also commonly suggest these days that any sort of vertical pushing from beneath is a flawed concept so far as changing lower eyelid position.
Is it the case that sometimes it can work and sometimes it doesn’t? Is it that when it does work, the effect is very marginal and so wouldn’t be very perceptible?
Interested in your insight on this topic. Many thanks!
A: CUSTOM infraorbital rim implants that saddle the rim and add vertical height can have a modest effect on reducing scleral show as there is a relationship between the bony infraorbital rim and the lower eyelid position. If a modest reduction in scleral show is all that is needed (1 to 2mms) then the implant alone may suffice. But in significan sclerla show with rounded lower eyelids and/or downturned outer eye corners, the implant will need to be supplemented with soft tissue management as well (spacer lower eyelid grafts and lateral canthoplasty) to have a very visible and sustained lower eyelid uplifting effect.
It is not a question of whether it sometimes works and sometimes doesn’t. You have to match the anatomic problem the patient has with the correct solution to treat it. All three techniques mentioned are tools to be used of which some lower eyelid reshaping needs only requires one while others requires all three.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a MTF transgender. I wish to reduce my underbust measurement through modifying my rib cage. I just read a post here https://exploreplasticsurgery.com/case-study-transgender-rib-removal-surgery-body-contouring/?doing_wp_cron=1619818519.8208200931549072265625 and I realised it is possible to modify the ribs to reduce waist size. I’d like to ask if it is possible to modify the ribs to reduce my underbust size? Can I also achieve this goal through a corset?
A:The portion of the ribcage to which you refer (underbust) is the fixed portion of he ribcage over the bottom portion of the lungs which can not be surgically reduced. It is also a ribcage area that is unlikely to be modified by corseting due to the fixed nature of the ribs.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have an initial video consultation scheduled with you already. My question is, can all the procedures I am wanting be performed on a single day? Tentatively, I am planning to get infraorbital-malar implants, nasal tip rhinoplasty, buccal lipectomy, and sliding genioplasty (bilateral where applicable). Of course, I won’t finalize plans for any specific procedure until I get your ultimate recommendation at the consultation, but, for scheduling purposes, I am wondering if it is possible to perform all of these in one operation. In particular, I would like to know whether it is safe to be under anesthesia for the duration of these procedures. Thanks, looking forward to speaking with you.
A: It is very common to perform many facial procedures at the same time. So the combination of IOM implants, tip rhinoplasty, buccal lipectomies and sliding genioplasty do not pose any medical risks or any undue physiologic stress on the patient through both the surgery and the healing process.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a few of questions regarding infraorbital implants, which I am considering potentially having (I am right now trying to choose between fillers or implants) and would really appreciate some expertise help choosing.
My first question is, how long do they last, exactly?
I know they are said to be permanent, but is that figuratively or literally? For instance, would it be possible to actually have them your whole life, or would you have to change them eventually? Given that they are after all of silicone, and that you have to change silicone breast implants each ten years, I mean?
2) Would it be possible to insert them from the inside of the lower eyelid, or can they only be inserted from the outside?
3) Finally, I understand that they are attached to the bone with metal screws? Does that mean that if I am passing through the metal detector at an airport that the screws would make the alarm go off?
And in case I would ever for some reason need to do an MRI, how would that affect the screws? Would it pull them out?
A:In regards to your questions about infraorbital rim implants I can provide the following answers:
1) All forms of aesthetic craniofacial implants are of a solid composition so the materials are structurally stable. They can never degrade or breakdown resulting in the need for eventua replacement. Solid silicone facial implants should not be confused with gel-filled breast implants which do have a limited lifespan.
2) While smaller standard infraorbital rim implants can be placed through a transconjunctival approach (inner eyelid), larger custom infraorbital rim implants can not. How this may apply to you I do not yet know.
3) The ultra small titanium screws that I use for most infraorbital rim implants (the same size as the screws in a pair of eyeglasses) are not going to make any metal detector go off and are compatible with MRIs. (titanium is a non–ferrromagnetic metal)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’d just like to say that this case study is incredibly valuable and the results visually look excellent – very natural and impossible to detect that work was done. I think 15mm is ideal in that regard.
I have a question about the method of surgery. When you do clavicle reduction, you obviously have segments of bone that you remove. It is possible to then remove the bone marrow from these/clean it and then use them as exogenous bone grafts for other patients? Would there be any benefit to having an entire piece of bone like this filling the gap of an osteotomy during lengthening, as opposed to doing a sagittal split osteotomy?
Secondly, how do you ensure that the clavicles are lengthened in the correct plane when you pull them apart? ie laterally in line with the existing shape of the clavicle.
A: In answer to your questions:
1) While the clavicle has an inner cancellous space that is not bone marrow.
2) While a fibular bone graft can be used for clavicle lengthening that is going to have the patient recovering from two ‘broken’ shoulders as well as a ‘broken’ leg. That is going to make the recovery process extremely difficult. Not to mention a much longer time of limited arm motion given how long it takes a bone graft to heal vs an osteotomy.
3) When doing a sagittal split the alignment of the bone can be seen as the outer segment slides away from the inner segment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Good Morning! I have a general question. Is it possible to have a shoulder width reduction surgery and rib removal waist line reduction at the same time? Or do they have to be performed separately?
A:It is not uncommon, in the properly qualified patient, to do shoulder and waistline reduction during the same surgery. The properly qualified patient is typically one that brings someone with them to assist in their early recovery phase after they return to the hotel the morning after surgery. This combination body contouring surgery is very difficult to take on alone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I underwent V-line surgery and zygoma reduction surgery nine months ago. But I’m still unhappy with my face width/size. I’m wondering if it’s possible I still have any swelling in my face? I know it’s been 9 months but I’m wondering if it’s possible I still have residual swelling. Maybe not, but I think people experience swelling slightly differently?
I have attached a post op pic of myself. Please let me know what you think,
A:It would be safe to assume that you have 95% (probably more) resolution of any swelling. With your thicker facial tissues you were never at risk of having too narrow or an overly oval shaped face. (overcorrection) Your aesthetic risk of the surgery is exactly what you are experiencing now…a result that is less than the desired amount of change. (undercorrection)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve wanted to decrease the convexity of my forehead for about 15 years, I don’t like the bulk/bulbous look it has. I didn’t know it was possible to do until a few years ago I saw your patient results. I do not want my hairline lowered, and worry if the scar will show if my hairline recedes. I’m currently 28. Thank you in advance for your time, I appreciate any information.
A: Thank you for your inquiry and sending your pictures. The best approach to reducing your forehead convexity is through a small frontal hairline incision. It can also be put behind the hairline but that scar placement requires a much longer scalp incisions as it lies behind the convexity of the forehead.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I am considering having chin burring with buccal and cheek and perioral lipo. My question is isn’t there a danger of damaging the facial retaining ligaments when performing cheek liposuction?
A: Like liposuction anywhere, blood vessels, serves and ligamentous attachments are maintained.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had facial feminization surgery 2 years ago and a type 3 forehead contouring which I regret doing and I’d like to have a bigger brow ridge so I am looking into forehead contouring using bone cement.
A: With a brow bone flap setback technique there is very likely some non-healed areas (bone gaps) along the margins of the flap. While these are not a problem now raising the forehead flap for access will expose them so a bone cement approach is the way to go for any form of brow bone augmentation. But the type of bone cement is critically important which is why HA (hydroxyapatite) is preferred over PMMA (acrylic) HA can tolerate exposure to the frontal sinus since it was originally developed for frontal sinus obliteration. Conversely PMMA does very poorly when exposed to any sinus bacteria and often ends up infected as a a a result.
Since most type III forehead contouring procedures often overlook the tail or outer aspect of the brow bone I will assume that the augmentation needed is mainly over the more central bone flap region
Dr. Barry Eppley
World-Renowned Plastic SurgeonCan I
Q: Dr. Eppley, I would ike hip and butt implants. I have a pretty boxy figure, I work out alot and don’t have enough fat for a BBL and would like curves to feel more womanly.
A: Thank you for your inquiry and sending your pictures. The success of buttock and hip implants is highly dependent on their pocket location and implant size, all of which is dependent on the patient’s goals. (yet to be determined in your case) Intramuscular buttock implants have the lowest rate of complications but that pocket location controls implant size. Hip implants have the highest complication rates of all body implants but can be successful if the implant size stays limited. (relegated to the hip dent areas)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For a long time Ive been thinking about improving the profile of my face by adding some projection to the mandible.
Doctor, you are renowned Plastic Surgeon, I observe your results and you are a surgeon of my choice.
Do you do online consultations based on sent photos and CT-scan?
I’m wondering what would work better for me: chin implant or sliding genioplasty.
A: Thank you for your inquiry and sending all of your pictures. Based on some preliminary imaging (see attached) your chin augmentation needs are in the 8mm range for which both an implant and a sliding genioplasty can accomplish.The key aesthetic difference between these two chin augmentation procedures at this normal range of horizontal augmentation is how they differ in chin width and what your feeling is for that chin shape consideration. A chin implant can make it wider or more square while a sliding genioplasty will either keep its same shape or make a bit more narrow.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,Some 30 years ago I had cheek implants and I always thought they were a little to big for my face. Fast forward to present day and I had Juva \derm Voluma done to fill out some hollows mid cheek. I believe the person that did the injecting did it too high. It was also my bad for not stating up front I had implants. It never crossed my mind this would even be an issue all these years later. Could this have displaced the implant? Same thing was done the other side and its fine. Can you also advise what types of implants were used back then and can they be removed without a lot of hassle and the cost of removal? Answers aren’t readily available because of age of implants. I’d really appreciate any help you can give me.
A:Thank you for your inquiry and sending your picture. Undoubtably your cheek implants are silicone in composition and can be removed by the route in which they were placed. (intraoral) Because deflating the cheeks by implant removal will have a facial changing effect i would leave the filler alone for now and see how it looks afterwards.
Injectable fillers can never displace cheek implants, particularly ones that are as old as yours are. They are very likely surrounded by calcifications which is very common in ‘ancient’ cheek implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am emailing to enquire about reshaping of the skull. This has always been a massive insecurity of mine and it’s become even more prominent in my every day confidence. The back of my head is wider and that is my main concern. I have included a medical letter from a doctor I’ve already seen. I would love to reshape my skull to create an overall more symmetrical appearance. I would appreciate any advice, support or procedure that could be suggested.
A: Thank you for your inquiry and sending your pictures. As your attached letter implies, while parietal eminence reductions scan be done, will it make a significant visible difference externally? In my experience it does because the actual removal involves both bone and a portion of the posterior temporal muscle. Technically what you need is better described as reduction of the posterior temporal lines of the skull. Referring to it as just parietal eminences is a very limited approach and understanding of the actual problem.
A preoperative 2D CT scan to look at the thickness of these tissues in this area would be needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
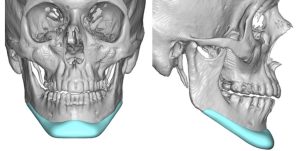 Q: Dr. Eppley, I am currently 26 years old with a standard chin implant in. I am interested in a custom chin implant and I was wondering what the price was.
Q: Dr. Eppley, I am currently 26 years old with a standard chin implant in. I am interested in a custom chin implant and I was wondering what the price was.
I am currently trying to decide between a vertical lengthening sliding genioplasty or a custom vertical lengthening chin implant.
I have included the implant in an attached photo. I want to know if the implant in the photo is considered just a chin implant (though it extends into the lateral mandible) or if it is considered a wraparound implant.
A: You are referring to an extended custom chin implant which costs the same whether the extended wings are there or not.
FYI such an implant design and a vertical lengthening bony genioplasty do not create the same aesthetic effects. While both add vertical length (the bony genioplasty greater than the implant) only the implant adds width to the chin and creates a seamless transition back along the jawline. In other words you are not comparing apples to apples so to speak.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got a sliding genioplasty last year and my bottom lip is still tight. The area under my lip feels stiff and or like its being pulled. My lips close fine, although my bottom lip appears a little smaller now. I have read a lot of your posts and it seems like the intraoral release with fat filler is something that you often recommend for this. I spoke to my surgeon about it and I was told that a V-Y procedure is something that she offers. Is that similar to what you do? Is it as effective? I am worried that this might make it worse. thank you!
A:Tissue tightness indicates scar contracture which ultimately means there is a tissue deficiency. Tissue deficiency issues are improved by a release, creation of a new dead space (tissue expansion) and filled in with a tissue replacement. (aka fat graft) In other words you solve tissue tightness by adding more tissue, not by simply moving what is already deficient around. (e.g., V – Y advancement) You have justifiable concern that a tissue rearrangement approach would not make it better and may make it worse. (more scar)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a custom wraparound jaw implant placed about a year ago. I have some significant asymmetry, with my right side jawline being smaller and not as sharp. What options would I have in regards of symmetry by augmenting the right side without a total replacement. Could I have a goretex strip overlay? Could I just have the right side of a one piece wraparound replaced without damaging the chin and left side?
A: When one has asymmetry of a custom jawline implant the first question is whether this is the result of implant placement, implant design or some differences in the thickness of the soft tissues. Knowing that most custom facial implants are designed with mirroring software, asymmetries due to design are very uncommon. The most common cause of jawline asymmetries, by far, is placement. Even slight asymmetries in position along one side of the jawline can make for a very visible external appearance change between the two sides. Thus you never consider a revision until you know exactly why it looks the way it does with a postop 3D CT scan. Such scans are tremendously revealing and will help make the choice whether it is to adjust the implant position or perform an overly implant for the smaller less defined side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a full jaw implant three years ago by a surgeon in Europe. My jaw wraparound implant got infected a few months ago somehow and formed two fistulas on either corners of chin. I took antibiotics and so far no more problems thank god. But the muscle when I smile looks botched as it curves up then straight down giving me a witches chin as I smile. Are you able to fix the fistula holes and the irregular chin muscle ? My worry is if I try fixing anything the infection may return hence causing me to lose the entire implant.
A: That is certainly unusual to have an infection years later. But the fact that it occurred in a such a delayed fashion and is on both sides of the chin suggests to me that this is where screws may be located and are the source of the fistulas. That aside a fistula represents an area of scar contracture and soft tissue deficiency. Thus they are acting as scar anchors that cause distortion when the chin pad moves. (smiling) They would need to be excised, a dermal-fat graft placed and then closed primarily. What effect that may have on recurrent infection is unknown since we don’t fully understand why it occurred so late after the initial surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Im interested in finding a way to reduce my skull and came across your site. I have a very large, elongated cranium that has bothered me my whole life. It has a circumference of 64,5 cm. Since I guess its not possible to change or replace parts of the cranium itself, maybe the burring approach could help reducing the circumference and the overall appearance. See attached images (I have a full CT scan). In my case I would like to reduce both the back of the head and the front to “shrink” the elongated look and maybe get some headwear to fit. Questions: What is the estimate cost for a procendure like this? I am living in Norway so its a long way. Are there any partners in Europe that offers the same type of surgery? How long do I have to stay away from work?
A:You are correct in that burring reduction is the only approach in an adult to reduce an elongated skull. As a general rule half of the skull’s thickness can be reduced by burring. If we move beyond whether the scar to access these to do the surgery is a potential issue, the question then becomes whether that amount of skull length reduction is worthy of the effort. Ultimately the best way to answer that question is by taking a side view picture and doing some computer imaging of the potential change.
I am not aware of any other surgeons in the world that do this type of surgery although there may be.
I don’t know what type of work you do but it should be no more than 10 days at most.
Dr. Barry Eppley
World-Renowned Plastic Surgeon