Your Questions
Your Questions
Q: Dr. Eppley, I am a 38 year old male who a few years back as an adult, I underwent reconstructive surgery for a scaphocephalic head shape and frontal bossing which was believes to be do to minor sagittal craniosynostosis. The surgeon burred down the protruding portion of bone in my forehead and did fat grafting to the parasagittal areas to address the somewhat narrowed appearance and give my head a more round and convex shape.
Overall, everything came out very well, my head has a much more proportionate shape, no more frontal bossing and and I am happy with the results. (This was done through a bicoronal incision. The top of the scar healed fine but the sides unfortunately had no hair growth despite it being a trichophytic closure. I had hair transplants put into the scar which you will notice little scabs in one picture as the grafts were taken that same day).
Long story short, despite the shape being much better, there does still seem to be a thickened sagittal ridge on top anterior portion of my head that’s more noticeable when my hair is shorter. You can see in the pictures that the top of my skull is more peaked in the front than in the back where the vertex is.
I was interested in possibly having that corrected within the next year or so and was wondering what your recommendation would be? What is your assessment of the pictures and what do you think I should have done (if anything)?
Since I already had a bicoronal scar which healed pretty wide (except for the top) from the last surgery and I had hair transplants to fix it, I wouldn’t be interested in something that would involve another bicoronal incision, only something that would involve a smaller incision on the top part of my head that could be hidden in my hair since I keep the top a little longer than the sides.
Several pictures are attached of different views of my head wit different lengths of hair.
A: Secondary burring reduction of the anterior sagittal crest can be done using the part of the coronal scalp incision that lies between the two bony temporal lines. (why that was not done in the primary procedure is not clear since it was always there…but that is irrelevant now) But before that is done a 2D CT scan is needed to look at the coronal slices to see the thickness of the desired sagittal ridge reduction. While it is always thicker due to the micro synostosis you have it pays to be prudent and due an evaluation before doing the procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 24-year-old female that got double jaw surgery and a genioplasty a year ago for recessed jaws and a small airway. I have been struggling since the surgery with how my new chin looks. It has never resolved but has seemed to stick out more and more as I have recovered since swelling has decreased everywhere else. I feel like it has taken away the more feminine face that I had before the surgery. I attached some pictures of my profile before the procedure because now that I look back on it, I feel like my chin was not a problem and should have not been touched. My surgeon though recommended me getting the genioplasty for my profile. They moved my chin 7mm forward, which is even more than the original 5mm the surgeon had told me. I was wondering if a genioplasty reversal would be possible? If so, what risks are entailed? I already still have numbness in the middle of my chin where the plate would be and I get very weird dimpling and muscle movements. I also feel like my lower lip is smaller/looks odd compared to before. Would love your feedback. Thanks
A:Thank you for your inquiry and sending your pictures. The question is not whether a sliding genioplasty reversal can be done but by how much is needed. (subtotal vs total) To help make that determination there are two key pieces of information thar are needed/missing: 1) before and after side view pictures of your face and 2) a postop x-ray. All sliding genioplasties can be reversed, it is just a question of how much is needed and any challenges posed by the hardware that was initially used in the initial sliding genioplasty procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in swapping out my Older Style Chin Implant for a Square Terino Style Implant or something similar . My issue with the one I have is I am constantly laying Filler over it to keep the look I like . I enclosed some Pictures as well .All I am after is lil more projection in Chin and where it wraps to Mandible I would like a Lil Squareness not so much round.The Pic of the Guy I enclosed is soo Subltle but I like the Squareness of his look which I prefer .
A:My assumption based on your description and picture is that you are looking for a wider (not necessarily more square chin appearance since that is what fillers can achieve) While I am not a fan of the standard square chin implants, because they are poorly designed if a square chin look is the desired result, they do make the chin wider. In that regard the style 1 square chin implant may suffice. But if a truly more square chin look is desired then a custom chin implant design is needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My face is slightly too wide (around 14.6cm) and I would like to reduce it but not in a drastic way, only by around 1.5mm each side. So basically, a very small reduction. Is it possible to do this without a cheekbone osteotomy (which I would like to avoid) and only by precisely shaving the sides ? I would only like to shave the part of the zygomatic which is I think called the zygomatic process (the part closer to the ear).
 A:What you are looking for is not shaving of the sides (zygomatic arches), which is impossible to do due to lack of access, but a posterior zygomatic process osteotomy dine through a small sideburn incision. That is how you reduce the zygomatic process. Technically this is the posterior osteotome site of complete cheekbone reduction osteotomies which is necessary with the intraoral anterior osteotomy to make the whole cheekbone move in. But it can be done by itself just for the purpose to which you refer.
A:What you are looking for is not shaving of the sides (zygomatic arches), which is impossible to do due to lack of access, but a posterior zygomatic process osteotomy dine through a small sideburn incision. That is how you reduce the zygomatic process. Technically this is the posterior osteotome site of complete cheekbone reduction osteotomies which is necessary with the intraoral anterior osteotomy to make the whole cheekbone move in. But it can be done by itself just for the purpose to which you refer.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My son is 3 years old, unfortunately he has uncured plagiocephaly… We live in Poland, the doctors we went to assured us that the head would take shape as the child grows, but that it is a long process, even 1.5 years, and they left us like that. Do you have any information or is there anyone in Europe who deals with this? We couldn’t find anything on the Internet… Apart from your website and we see that you are doing amazing things here! I understand that now, when my son is still small, we can’t do anything because the skull is constantly growing and so we will probably have to wait until the age of 18 until its growth stops… I am asking you for some information, best regards
A: What I can tell you about your son’s plagiocephaly is:
1) At 3 years of age it would be reasonable to assume he is not going to change the shape of his head by any ongoing growth.
2) For an onlay custom skull implant one needs to have gotten past puberty. Such procedures in teenagers are done around ages 15 or 16.
3) I am not aware of any surgeon performing this surgery in Europe.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have my lower ribs protruding in both sides, and I’m interested in exploring cosmetic surgery options to make them less noticeable without complete removal. Are there procedures available for this?
A: The rib removal surgery that I have performed over the past decade for waistline narrowing is exactly that…subtotal removal of ribs 11 and 12 and sometimes 10 as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I recall originally he was using a single bracket instead of a double to support the clavicle, and I’m wondering if he might again use a single on mine instead on only the back of the clavicle to prevent any chance of the bracket showing through the skin. I know he mentioned this was a possibility and I’d love to minimize the aesthetic risk even if that means longer healing time.
“Scapular Shave” – could this be performed during my clavicle reduction procedure?
A: Clavicle fixation plates are applied to the top (superior) and front (anterior) portion of the clavicle. There is no way to ever place such plates on the back (posterior) part of the clavicle.
Of the superior and anterior plates the superior plate is the most important for structural support. This is also the plate location in which the risk of plate show exists. Thus going to a single plate fixation does not eliminate the risk of plate show.
In consideration of trying to reduce the risk of plate show options include; 1) using a lower profile siuperior plate (3.5 to 2.5mm) on top or 2) only plsce a 3.5mm anterior plate. Neither of these fixation techniques i have yet used so I can not speak as to their long -term, fixation stability in this application. The question is not whether they can be intraoperatively applied and have immediate stability but how do they resist any bone displacement weeks later.
As for scapular spine reduction (aka scapular shave) that can be performed at the same time as clavicle reduction osteotomies.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am looking to fix my severe orbital dystopia among other glaring obvious asymmetries (chin, nose, cheeks, etc.) that make me look unusual, extremely asymmetric/unattractive. I believe that these asymmetries are congenital (it has been suggested that I was born with a mild hemifacial microsomia). I am extremely depressed about my appearance and it is worsening as I am aging. I am working with a surgeon who was going to perform a OBO, but decided that, after virtual surgical planning, the vertical mm’s I would gain weren’t worth the hassle of the surgery. Now, the plan is to appeal with insurance to get an orbital implant placed. I received the “after” morphs of what that could look like and am upset that, even with the implant, there will likely not be much of an improvement on the orbital dystopia (and the medial canthus would remain at the low placement it is currently sitting at). I am hoping to see what you have to say about this situation.
A: The answer to your question in my experience is that you need an OBO. No non-OBO procedure is going to make much of a difference in your case. As a general rule non-OBO VOD procedures are indicated when the VOD is 5mms or less. Any amount greater than 5mms needs an OBO procedure.
Why your surgeon won’t do the procedure I can not say but he likely was trying to do it without a frontal craniotomy…which is not going to work.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have read a lot of articles at your website and I was fascinated! I would like your first opinion , since I live far away. If we agree to a satisfying solution , I am thinking in coming .I send you photos and video as well.
My problem is saggy skin..I am 43 years old , 1.67 cm height and 53 kg weight. I do exercise a lot , but the skin is loose. I have not lost a lot of weight. My skin especially at buttocks is very saggy .
I am interested in buttock lift. I would like you to tell me your professional opinion. Which would be the best decision for me to make ? I understand that he upper lift does a better work at saggy skin but it has extended scars as I have seen and I fo not like that. Also , I have also saggy skin at the banana area below the butt, so I suppose it will not make any difference there. On the other hand , the lower buttock lift maybe combined with an implant could be another option. I am not sure though if that will make a significant difference at the saggy skin at the profile.
Also , I read a lot of future implications about implants – such as malpositions etc – and I am a bit afraid.. Are they safe? I am not interested in BBL , since I have done that 4 years ago. At that period I gained weight in purpose , in order to undergo the operation. I weighted 59 kg then. Now I am 53 and the result of the fat transfer has disappeared. I know that when – and if – I gain weight , my butt will be bigger.
I am so confused. I would like to get rid of saggy skin , to have more round , lifted butt and NOT FLAT butt – due to the lift – I like projection as well – not extreme but more natural to the whole body.
I am looking forward to hearing from you as soon as possible!
A: I think you have largely correctly summarized the options including their advantages and disadvantages. Saggy skin is always a challenge and you can not reduce/excised your way out of it nor can you augment with enough volume to fill your way out out it. It takes a combination approach of which the best choices are lower buttock lift and buttock augmentation with implants. (intramuscular implants don’t have many of the historic complications associated with buttock implants) Whether they should be performed together or separately can be debated, each way has its merits.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a narrow forehead, jaw, and narrow, flat (square) cheekbones. I would like to expand my head. Does this affect my eyes, meaning they appear close together?
A: Logically you would assume it would since as the head gets wider and the eyes stay the same they should look closer together by comparison. But whether that effect is signifincat is the question. Computer imaging of pictures will answer that question.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, if I choose to get a genioplasty. Should I remove the plates and screws? If I don’t remove them would I be able to get fillers or Botox in the future? Would there be a potential risk for infection? In addition, how long after genioplasty would you recommend getting fillers or Botox?
A: In answer to your sliding genioplasty questions:
1) Hardware removal later is optional. Most patients never choose to remove it.
2) There is no infectious concerns with injections into or around the fixation hardware.
3) Allow 3 months after the surgery before doing any injectable treatments.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ll explain more in depth what is going on and what I want to accomplish.
Implant used – implantech terino style II size large
Method – inserted from under the chin
Imaging – whatever a maxillifacial surgeon uses. I don’t know the name
I had the implant placed in October 2020. Haven’t really had any issues with it. I went to a maxillofacial surgeon to discuss my options for issues with my jaw alignment which is causing issues with my molars. Long story short I’ve been told double jaw surgery + sliding genioplasty is the answer. Orthodontists unable to fix the alignment issues.
While doing the scans he incidentally found that I have around 3mm of bone resorption from the implant. Visually it looks no different and I am still quite pleased with the result.
I was told by the doc who did the chin implant that some “settling” is completely normal. He didn’t seem concerned but I am exploring options in the event the erosion worsens.
I saw your reply to a post on Real Self with some more info about what can be done to remedy the erosion. So this is mainly what I am interested in learning more about. If he has a good solution then I would have no issues with getting a revision done with him in 1-2 years if the erosion continues getting worse.
A: This is not bone erosion, it is implant settling…a passive self-limiting process that is not progressive. If you are happy with the chin augmentation results there is not need to treat this radiographic phenomenon.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, what procedure is the best for me? My eyes is too bulgy and flat I want feminine eyes how to achieve that?
A: You have a significant undereye (infraorbital-anterior malar) bone deficiency with excessive scleral show (due to lack of lower eyelid vertical height) This makes your eyes appear bulging but the eye position is actual ly normal. (pseudoproptosis) Infraorbital-malar augmentation with lower eyelid reconstruction (spacer grafts and lateral canthoplasties) is needed for an improved appearance.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there, I’m a 27 year old male, recently gone bald to reveal what seems to me to be a mild case of brachycephaly. It seems like you have treated patients with the same problem to some great results. Looking to discuss possible solutions. I consulted with a craniofacial specialist in the UK and he said he didn’t think there was much he could do, besides shaving down the actual skull, which I wouldn’t do. Hoping there’s a less drastic remedy available.
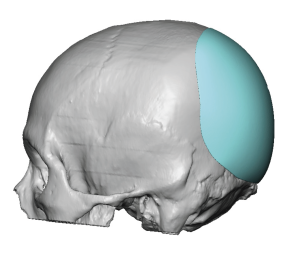 A: Brachycephaly implies a flatness to the back of the head for which augmentation would be the best aesthetic procedure…not shaving the bone which is exactly the opposite of what should be done. A custom skull implant works well for this type of augmentation.
A: Brachycephaly implies a flatness to the back of the head for which augmentation would be the best aesthetic procedure…not shaving the bone which is exactly the opposite of what should be done. A custom skull implant works well for this type of augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am due to have calf augmentation post Achilles tendon repair due to severe fatty atrophy of the soleus muscle. I saw that you have done this surgery before and the patient is in your photo gallery under Body Implants – Patient 21. Dr Eppley used 2 implants in this circumstance and I was wondering what type/brand of implant they are? The surgeon I am booked in with is willing to do the surgery and we only have the Implantech Calf Implants available here. My question is do you think the Implantech implants are the best ones and, if not, can you suggest any other brands?
A: There is a very broad selection of calf implant shapes and sizes offered by Implantech. Your surgeon can surely find implants that will suit your individual needs based on leg measurements.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m considering the removal of a silastic implant that was placed under the chin (6mm anterior projection), what realistic complications are there to expect? It was placed 2ish years ago. It’s hard to know what to expect with ptosis, chin balling, nerve damage, and all sorts of complications being thrown around on forums. Could you maybe explain how the time the implant was in, may affect the chances at returning to post-op appearance?
A: I would say the only significant risk, and I would not call it a complication but an expected outcome, is that of soft tissue chin pad ptosis. The question is not whether you will have it but how significant it will be. There is no returning to 100% of your preop appearance. Whether it will be 75, 85 or 95% can not be predicted beforehand.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Really want a consultation for the back of my neck , you were the only one that seemed available
A: The ‘triple roll ‘neck poses significant challenges in terms of improvement. One approach is a middle roll excision with undermining on the superior and inferior rolls to bring it together creating an overall flatter effect. Another approach is a dual excision along the two deep inverted horizontal lines. Each approach has advantages and disadvantages but the major difference is the location of the scar lines.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a scapha reduction (macrotia surgery) on both ears. I saw a previous reply on your website to someone interested in the same procedure that the helical rim is crucial for this procedure in order to be able to hide the scar. While I do feel that I have a small helical rim, it’s not as prominent as some, so I am wondering if I am even a candidate for this procedure.
 A: The concept in most macrotia reductions is a combined scaphal and earlobe excisions. In the scaphal reduction it is ideal to have a prominent antihelical fold and/or helical rim for optimal scar placement. While yours is smaller than some in those esr features (probably because you are a female) it is not contraindicated for the procedure.
A: The concept in most macrotia reductions is a combined scaphal and earlobe excisions. In the scaphal reduction it is ideal to have a prominent antihelical fold and/or helical rim for optimal scar placement. While yours is smaller than some in those esr features (probably because you are a female) it is not contraindicated for the procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Sustained a cheek fracture last year and hospital did not want to intervene! I notice a big difference in facial symmetry with malar depression. Just looking for help because it has caused emotional pain.
A: This is a classic depressed ZMC fracture. At one year after the injury the depressed cheekbone is now healed into this abnormal position. The options now are either to refracture the bone and try to reposition it back closer to normal (secondary osteotomy) or leave the bone where it is and make a custom cheek implant overlay matching the shape of the other side. Each approach has its advantages and disadvantages. But for either one getting a 3D face CT scan is importsnt to have a clear understanding of the cheekbone’s exact shape. Such an understanding may influence how successful either approach would be, particularly the osteotomy method.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a large head with a dent in the back of my head. I know it’s not possible to make my head smaller, but I want the dent fixed. If I get the dent fixed will it make my head larger?
A: That would depend on the size of the dent and how much volume it would take to fill it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, In determining the best jaw angle width for my custom jawline implant I have read that it is usually better to keep it less side than that of my cheeks. Is that good way to do it?
A: To anatomically understand cheek bone anatomy it has two components which have an anteroposterior orientation, the anterior main zygomatic body and the posterior zygomatic arch. Cheek width is determined by both components of which, in most Caucasians, the lateral zygomatic arch creates the maximum cheek width.
When using cheek width as a determinant of jaw angle width the maxiimum width of the zygomatic arch (lateral cheek width) is what is usually used to help guide its width not the anterior zygomatic body width.
But as you can see it all depends on how one choose to define their cheek width.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am wondering if you could help.My son had ear pinning one year ago. I was not happy with the results straight away, however, the surgeon told me it was impossible to undo the surgery as it would require a rib cartilage to be inserted into my son’s ears and would be too risky.
I would greatly appreciate if you could kindly look at the images attached and advise if there are any procedures that seem to be possible and what the doctor thinks requires to be done esthetically.The top of the ears look like they are glued to the head, the middle is parallel to his head and the bottom part of the ears is very prominent. The ears lack any nice shape.
Would pinning the bottom of the ears correct the overall look of the ears or is it the top part that is required to be corrected to be more prominent?
I am supporting my son and I am telling him how beautiful his ears are after the surgery. He has raised his concerns, but I do not want to book a consultation first as I will prove to him that the surgery did go wrong and that his ears do not look nice. I would like to know first if the doctor believes that there are options to correct the ears, as the last thing I want is to tell him that his ears do need to be corrected and then find it is impossible to do. This would devastate him as he has gone through a lot after the surgery.
I would be very grateful if you could have a look at my son’s photos and advise.
A: The reason his postop ears look like they do is that bottom third of the ear (earlobes) remains unchanged from the surgery. Only the cartilage containing part of the ear (upper 2/3s) has been setback while the earlobes remain protrusive. This is a common surgical oversight. Many otoplasties needs a soft tissue earlobe setback to look harmonious along the helical rim .
This is what I anatomically see. Whether that is his exact concern or whether he is having trouble adjusting to the overall change (missing his old ears) I can obviously not say.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am reaching out to seek advice from you who has a rare expertise in fat grafting and lip surgery. I am 63 years old and underwent a secondary face lift along with lip fat grafting a year and a half ago. Unfortunately, I have been left with a noticeable lump on my upper lip. I understand that such cases are complex and that many surgeons may be reluctant to address them. But I hope that your proficiency in this field could shed light on my condition and offer a potential course of action.
A: Injected fat lumps in the lips always have to be excised, generally through either a vertical vermilion or a vermilion-cutaneous inciosion depending upon its location and size.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, 27 yo female who is unhappy with smile/avoid being in pictures. Desire for upturn of corners of mouth when smiling/more even smile.
A: Smiling is a dynamic facial movement while surgery is a static procedure. Thus at rest the corners must appear more upturned and the mouth wider for a bigger more upturned smile.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have very droopy eyelids and I was wondering if a brow bone implant would raise my eyelids? Because I do want my eyelids reduced sometime in the future and I’m not sure how it would affect it.
A: A brow bone implant is unlikely to improve droopy eyelids to any significant degree.. Its placement would not affect the ability to perform upper blepharoplasty surgery in the future.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m inquiring about the brow bone augmentation. I’ve been trying to find a way to have deep set eyes. I went to a doctor in L.A. and he suggested orbital decompression, which sounds dangerous. So I’ve been searching around the internet and I found of Dr Eppley’s before/after picture of a patient , under “forehead brow bone and temporal contouring” patient 8 and 9, (esp 8), desire for more prominent brow bones and forehead.
I’m thinking of doing fillers first to see if it would do the same effect, even temporary. In this case at least I know if it would look good on me. Maybe it’s a waste of money and just go straight to the implant.
Thank you,
A: In answer to your questions in regard to the pursuit of deep set eyes:
1) Orbital decompression is not a dangerous procedure. It is just the lowering of the anterior bony floor of the orbit which allows the eye to drop back and in a few millimeters. It could be a useful adjunctive procedure to brow bone augmentation. But it is unlikely alone to create deep set eyes…but that depends on what your natural anatomy is.
2) Certainly the reverse approach, augmenting the orbital rims , has a more powerful effect…again based on your natural anatomy.
3) A good way to test #2 is with computer imaging using your pictures to look at brow bone augmentation changes. I will need three pictures to do so. (front, side and ¾ views) The latter two are the most important when looking at any type o forehead and/or brow bone augmentation.
4) Injectable fillers can always be a good test of any facial augmentative change provided the volume of filler approximates the volume of the implant that will be used to create the permanent effect. For example in a brow bone implant typical volume is in the 4 to 6cc range. Fillers come in 1cc syringes. So it is easy to see that the effect between fillers and implants are not similar. Thus fillers are fine to try as long as one recognizes that implants have a far more powerful augmentative effect depending upon the size of the facial area being augmented.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am potentially interested in posterior temporal reduction surgery because I feel that my head is too large. I also feel that I could benefit from anterior temporal reduction surgery because the area from the side of my eye to my hairline is also a bit too large. I attached a photo that shows what I am talking about.
A: Thank you for your inquiry regarding temporal reduction surgery. To better understand such head narrowing surgery I refer you to the following link which explains the important difference between posterior and anterior temporal reduction surgery:
https://exploreplasticsurgery.com/the-anatomy-of-t…or-the-wide-head/
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello there, just a quick question regarding aftercare post surgery from my custom forehead implant. Everywhere else seems to request the patient wears the head bandages after surgery for one week, can I ask why you suggest removal from the next day?
A:I don’t suggest removal of the head dressing the next day, I take it off the next day as the immediate head dressing is very tight and uncomfortable. A new less tight and more comfortable head dressing (Coban) is applied thereafter and should be worn until at least the drains comes out…which is usually 2 to 3 days later.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I previously had iliac crest implant surgery and it has left me with very obvious hip dips/ indents, even after a fat transfer. I am very thin, so I need to gain weight before having another fat transfer. I was wondering it custom hip implants might be a better option than another fat transfer? Is it normal for iliac crest implants to create hip dips? How much would it cost for custom hip implants? Thank you!!
A: While not common creating hip dips can occur when the greater trochanter sticks out much further than the natural iliac crest. Iliac crest implants work best in straighter profile hip-thigh patients as opposed to a more triangular profile shape.
In the spirit of ‘past history predicts future behavior’ why would fat grafting work better the second time than the first…particularly when one has to gain weight to undergo the procedure? The point is…it won’t.
Now that doesn’t make hip dip implants perfect and they have their own issues. But that is the only remaining treatment option.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to have an online consultation in relation to an osseous genioplasty procedure or jaw surgery.
Over the past 3 years I have conducted some personal research, ~5 consultations, and also previously had a chin implant a number of years ago which I had removed after a few months of having the implant.
I would greatly like to have an online consult given Dr Eppley’s significant experience- and that I have found where I live.
Regarding my condition, I have a good bite – but heavily proclined lower teeth. Despite the proclination, my soft tissue profile actually does not make this ‘dental bulge’ so distinct (see images) – rather I have mostly a small/backwards lower jaw. The primary medical aspect I consider is not bite but sleep apnea related – which is quite bad and has become significantly worse over the recent years.
I have a good range of pictures + CBCT scan that I can send through/and also live display on my computer during the consult to assist in understanding the situation virtually.
Please note some points I would hope to raise/discuss to give some more context given my experience with the situation:
1) The 8mm chin implant I had years ago gave nice projection (see image) – and looked genuinely better overall, but significantly deepened the labiomental fold which led to a somewhat uncanny result – as I understand and have seen other cases – this can be controlled by a genioplasty forward + down movement – hence a key reason for my preference in the procedure.
2) I also have researched and done some consultations for jaw surgery. I hope to avoid jaw surgery because the procedure is more invasive – but open to discussion + have some scans from one other jaw surgery consult.
3) I’d like to discuss some genioplasty cases I have seen online that appear similar to mine (backward and short chin). Some ‘major’ ~8-10+mm advancements in these cases gave surprisingly great results – comparable to jaw surgery advancements. In some cases these people were recommended with jaw surgery as the only solution given their profile (whilst having a decent bite) – but opting for genioplasty still led them to a very good result. Hence a key reason I have been quite interested in osseous genioplasty over jaw surgery.
4) I’d like to get an idea of a procedure plan/cost.
Greatly appreciate your time and look forward to hearing from you.
A: Thank you for your inquiry and detaiilng your concerns and chin implant history. There are three things you have had stated that makes the case for jaw surgery not an isolated chin surgery.
1) ‘Bad’ sleep apnea
2) Heavily proclined lower teeth
3) Deepening of the labiomental fold with the chin implant (the same will happen with a sliding genioplasty)
#1 and #3 are the long term issues that need to be heavily considered. Do you really want to live the rest of your life with that degree of sleep apnea? If you took out the chin implant because of the labiomental fold change why would you feel any better about that same effect with a sliding genioplasty?
While I can certainly understand why one would want to avoid jaw surgery if possible but I would question tjhat decision in a young person. I have seen plenty of patients who opt for isolated chin augmentation or aesthetic jaw implant surgery only to reverse those later when they have decided to have jaw surgery…which they should have done so initially.
That being said there is nothing wrong with a sliding genioplasty as long as one has carefully considered the jaw surgery option which does address the fundamental problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon