Your Questions
Your Questions
Q: Dr,. Eppley, I am a transgender man (FtM) and I am interested in your iliac crest reduction surgery. I have a slightly wide-set pelvis that bothers me quite a lot. And because I am already a low body fat there isn’t really anything I can do to change the shape of my hips with fat transfer. After doing some research online, it seems you are the only surgeon that performs this surgery. I am interested and have questions about the recovery of the procedure, such as what kind of scaring I am going to receive (as I’ve been told by others that have had reconstructive surgery on their pelvis that the scaring is invasive) and would I have the same mobility I did prior to surgery? I am an athlete and long term I want to retain my conditioning so I don’t want this surgery to impede my conditioning long term.
A: Iliac Crest reduction removes a portion of the outer portion of the most lateral wing off the ilium. (aka iliac crest) This does not detach ant significant part of the TFL or gluteus medialis fascia. As a result there is no long term limitation in mobility or function.
The important question is whether this amount of bone removal will result in enough bony hip reduction for you. To help make that assessment I would need to see some pictures of your hips.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, . I would appreciate if you would reply to this question by email. Attached are two photos. The first photo, unedited, is how I look now. The second photo, marked up, is roughly about how I would like to look after surgery. I’m sure certain factors make it so that you aren’t fully able to tell, but do you think my marked up photo is a possible expectation to have for my face to look after surgery if I scheduled a genioplasty with you? Your time and response means so much to me.
A: You are showing an unobtainable chin reduction result by any method. At best you could only achieve about ½ of that result. Chin reduction poses surgical and anatomic challenges that do not exist in chin augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, , I am 22 year old girl with chubby face that contains a lot of fat on face which eventually led to perioral mounds over my lower cheeks and fat deposition on my lips corners and even extended till upper lips . The fat deposition on upper lips led to slowly sinking my uper towards inward and I am really concern about it . How this will be reduced . Does after liposuction I have to maintain healthy weight or it will come back after weight gain and once I removed my perioral mound will it develop into marionette lines in future.
A: In my experience with perioral/cheek liposuction recurrence of the fat deposits has not been reported to me. But maintaining a good weight in any location of liposuction would be prudent. I am also not aware that such facial liposuction creates marionette lines or nasolabial folds.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a chin implant removal about more than 2 months ago. It was a small button chin implant, placed intraorally for 8 years. It is also worth noting that my button implant rested a little higher than usual, close to the lips. The removal would be my 3rd intraoral chin surgery. I went to a new surgeon and he kept convincing me to remove the implant because it was making me look “masculine” rather than “feminine”. However, I regret removing the implant because of the following:
1. I actually prefer how I look with the implant as it gives me more definition and structure especially at the side view. In fact, since the removal the shape looks broader and longer, and retracted which makes me look more masculine which is the opposite intended effect.
2. My lips (particularly the lower lip) has gone backwards and inwards. It is significantly thinner. My original lips have always been full and everted. I can’t find much information on this online. I also feel like the lip angle has changed. Right now I have to use effort to close my lips and it keeps making a “pursing” mouth effect. I also have lower teeth which were not present before. Also, it’s strange but somehow my top lip also looks thinner and droop downwards (probably to reach my bottom lip) which is elongating my philtrum and I hate this effect as it makes me look so aged and sunken. Is my philtrum already permanently stretched? Or will it be back to normal once the bottom lip is restored, but how will it be restored?
3. Overall lower face looks sunken because the chin and lips went backwards and now I look so much older and less youthful. I prefer my lips rolled forward and chin to be forward as well.
4. My labiomental fold used to be deep (which I like actually, despite many people preferring a shallow one). Now it became more shallow which is strange to me because from what I read in your articles online, the labiomental fold cannot be changed and is a fixed structure
Anyway, the point is, I brought these issues up to my surgeon but he insists I 100% do not have chin and lip ptosis, despite me feeling that the symptoms are evident. He also attributed these to the botox he put in my chin 1 week after the removal, as a precautionary measure to not overwork the mentalis muscle while it is healing. So he is saying the botox is contributing to my lip problems. I am unsure of this and feel it is likely a ptosis or mentalis issue.
Right now, what I really want is to revert back to how I looked before the chin implant removal. I want the same implant back, and the same fullness and eversion of lips back. I want a more forward looking face rather than a sunken one. Somehow this chin implant removal has caused a slight “facial collapse” effect on me.
A: You can certainly have your original chin implant style/size put back and the new chin implant removed. That is not the question and is undoubtably what you need to do based on your comments. How close you would return to how you looked before can not be accurately predicted but, even if it is not 100% the same, you will feel better about it than you do now.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am an 18-year-old male student living in South Korea. I have a wide facial width and am considering skull surgery. I have some questions:
Is it possible to perform surgery that involves cutting both sides of the skull vertically and reattaching them to reduce facial width?
How long will I need to stay in the hospital for recovery after the surgery?
How much can the facial width be reduced?
What is the total cost for the entire procedure?
Have you performed this type of surgery before?
A: I believe when you say facial width you mean the width of the side of your head??? (aka temporal width) If so that is a common procedure that I perform. It is done under general anesthesia usually with an over nite stay in the facility. But to be clear on this issue I would need to see a front view picture of your face/head to fully understand what you mean by excessive facial width.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Big fan here. I read lots of stories about you and know many people who have consulted with you in the Looksmax community.
I wanted to ask what the price for small Supraorbital Silicone Implants are. As far as I know the surgery would be next to minimally invasive which made me think of you and Silicone instead of other materials like Peek/Titanium. I have had a jaw surgery just last year and got a really good result but I would rather not undergo another big surgery.
A: Supraorbital or brow bone implants have to be made custom since there is no such standard implant for that facial area They are usually placed through an endoscopic approach with small scalp and upper eyelid incisions.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, . I have a rather short and wide face and my jaw and cheekbones are visibly asymmetrical. One side of face is ”lower” than the other and the skin is not as tight as on the more developed side. I would also like to do rhinoplasty since I’ve been unhappy with the tip and slight hump on my nose for a long time.
I’m wondering if it would be possible to schedule a virtual consultation where we could discuss the treatment options and I could address some other concerns that I have about my face.
A: What you have is classic right-sided facial asymmetry. It can be seen that the right side of the face from the position of the eye down to the jawline is vertically shorter or compressed…fortunately only to a modest degree. The three most affected structures are the eyeball, cheek and jawline…all of which can be managed by custom implant designs for asymmetry correction during the same surgery. A rhinoplasty can also be concurrently done.
I would need to see some facial pictures from different angles to do an imaging analysis.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m proceeding to have orthognathic surgery next month (BSSO, Lefort 1 and genioplasty) to fix skeletal jaw issues and a 8mm overbite. I currently have a full silicone wrap around jaw implant. The surgeon is going to attempt to maintain the posterior portion of the the implant (jaw angles) and just remove the anterior portion and chin in order to execute BSSO and genioplasty. My surgeon has admittedly never tried to salvage existing jaw implants. My question is, do you foresee any issue with the surgeon cutting through and removing only a portion of the implant while attempting to keep the jaw angles intact? Thank you!
A: It makes little sense to try and keep any portion of your existing jawline implant. The risks of infection of it dramatically increases and it makes it harder to do the BSSO.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I have micro pigmentation on my scalp if I have a skull implant?
A: Yes you can. The skull implant is down at the bone level under the 5th layer of the scalp. Micropigmentation is placed into 1st layer of the scalp wet;l away from the skull implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about vertical chin reduction:
1) Is the 5mm to 7mm range limited by safety or aesthetic factors? Would there be any chance to get a reduction of 1 cm?
2) Would you recommend wearing a compression chin strap after surgery?
3) Lastly, when can I start playing contact sports after surgery?
A: Answers:
1) The level of the inferior alveolar nerve and the tooth roots are all factors that control the amount of vertical bone height that can be removed.
2) A compression chin strap would be important.
3) 6 to 8 weeks after surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there. I’m trying to find out what this might be. I noticed it about 3 years ago when I started to shave my head. It’s bony and feels like part of the skull. No symptoms or issues. Thanks.
A: Based on this one picture this lump appears to be a benign osteoma…which are very common on the skull. It can be removed under local anesthesia.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am enquiring about having my cheekbones decreased in width. I would like them to be less wide and was wondering if there was a procedure for this. Thank you.
A: The procedure is known as cheekbone reduction osteotomies in which the entire cheekbone throughout its length is moved inward by a front cut (intraoral) and a back cut through the posterior arch. (small external side burn incision)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, A question I have in response is that from researching the website about sliding genioplasty, one possible aesthetic concern especially as a male is a narrower chin from the frontal view. I was wondering if this would be overcome by adding a small pre-jowl implant in front of the osteotomy as mentioned on the website or if this likely wouldn’t be needed in my case. Thank you.
A: I could not say n your case since I have not seen a front view picture. But suffice it to say that the risk of looking a bit more narrow is possible since you would need an 8 to 10mm forward bony movement. If the patient was concerned about that risk an implant as you have indicated would be the appropriate mitigation of that risk.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, To whom this may concern. I was wondering if the surgeon is able to a large restructuring to a patient’s skull that has sagittal crainosynosis? Thanks!
A: In adult scaphocephalic head shapes the typical approach is bony reduction of the AP length as well as thge sagittal crest (as the bone thickness permits) along with augmentation of the sides of the head with custom skull implants. How this problem is approached in adults is very different from that in infants and young children.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in a beard transplant and would want to get that done before doing a jaw implant. However, I’m still very much interested in getting the jaw implant done with Dr. Eppley in the near future. I do have one question for Dr. Eppley regarding the beard transplant however, if you would be so kind as to relay it to him: “Given that I currently have a chin implant, and infection is a possibility, I’m wondering what sort of risk having hair transplanted to the chin area would pose for the implant? You have spoken about needles penetrating facial implants when people undergo filler injections, and that being a cause of infection in certain cases. I’m sure you’re aware of the process of extraction and implantation for hair transplants (the same process applies to beard transplants). A small needle (much smaller than a filler needle) would be poked into the chin area to create the holes needed for graft implantation. What are your thoughts on this? Could this process potentially cause an infection to the implant? Or is there no cause for concern in your opinion? Any time you could take to answer that question would be greatly appreciated.
A: I see no concerns doing a beard transplant over an existing chin implant. The soft tissue chin pad is very thick so it is a long way from the depth of the hair follicles to the implant capsule.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, At this point I don’t know where to turn too. I removed four healthy wisdom teeth. Ever since then I’ve developed a range of health issues. However, I noticed a lot of facial changes such as a loss of forward growth, loss of cheekbones, less defined angle of jaw, less defined jaw, narrow midface and jaw. I’m wondering if I could potentially show you an image of my face before removal and you try your best to recreate that image. No surgery or implant is too invasive nor too expensive. The phone of me in the red is before extraction. Please let me know. Thanks
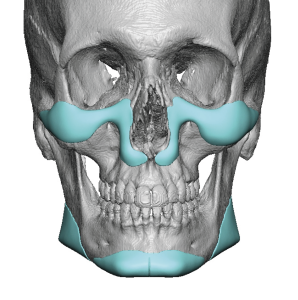
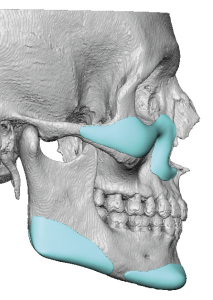 A:Removal of wisdom (3rd molar) teeth would certainly be a rare predicate for developing any health issues including facial shape changes. Regardless of the origin the pertinent question is what could be done for your facial restoration. This is a dimensional question of which you have already provided that answer by you description of ‘ loss of forward growth, loss of cheekbones, less defined angle of jaw, less defined jaw, narrow midface and jaw.’ This speaks to augmentation of the cheeks/midface and jawline to some degree. The discussion then turns to whether it should be done by standard or custom implants and what surface areas need to be covered. Ironically I just did a young male patient yesterday with similar subtle augmentation needs where no augmented area was larger than 2 to 3mms in thickness. (see attached) I am not saying this is exactly what you need but it is just a concept of subtle larger surface area midface and jawline augmentation effects. What you are describing is more of a global effect a rather than an isolated ‘spot’ issue.
A:Removal of wisdom (3rd molar) teeth would certainly be a rare predicate for developing any health issues including facial shape changes. Regardless of the origin the pertinent question is what could be done for your facial restoration. This is a dimensional question of which you have already provided that answer by you description of ‘ loss of forward growth, loss of cheekbones, less defined angle of jaw, less defined jaw, narrow midface and jaw.’ This speaks to augmentation of the cheeks/midface and jawline to some degree. The discussion then turns to whether it should be done by standard or custom implants and what surface areas need to be covered. Ironically I just did a young male patient yesterday with similar subtle augmentation needs where no augmented area was larger than 2 to 3mms in thickness. (see attached) I am not saying this is exactly what you need but it is just a concept of subtle larger surface area midface and jawline augmentation effects. What you are describing is more of a global effect a rather than an isolated ‘spot’ issue.
Dr. Barry Eppley
World-Renowned Plastic Surge
Q: Dr. Eppley, I found your page when searching for testicle enlargement. I’ve been on testosterone for about a year and have noted a significant decrease in the size of both of my testicles during that time.
I have heard of two possible procedures and would like to get information on both.
First is an implant that wraps around the testicle and is filled with silicone.
The second is testicle removal and replacement with an artificial testicle. I realize that this will eliminate my body’s production of T but my level was nearly at the bottom of the scale before I started T replacement therapy. Since I’m doing that already I don’t have any problems with this option.
At this point I’m leaning more toward the second option since the end result is similar and it just seems more reliable over the long term to me.
Just some background information. I’m 67 years old in good health. I have HBP and high cholesterol and take amlodipine, metoprolol tartrate, and simvastatin which control both well.
A:At age 67 there is no question that a solid testicle implant is what you would best suit your situation. The only question is whether testicle removal is really necessary with the placement of the implants. That would be driven by what size testicle implants you desire. In most acses of older men with testicla atrophy the testicles are left in place and larger implants are placed which naturally pushes the testicle out of visibility. (displacement effect) If there is not a big difference between the size of the implant and the testicles then testicle removal would be needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q:Dr. Eppley,as I recall, he mentioned that it’s possible to contour the body further through liposuction. In this context, I have a question: Is it possible to define the midline of the abdomen more prominently using liposuction? Or to make the abdomen appear more contoured overall through liposuction? Please find three reference images attached, including a recent photo of myself.
A:You are specifically referring to abdominal etching, a liposuction technique where lines are placed through linear fat removal. Since you mentioned the ‘midline of the abdomen’ this means midline vertical linear liposuction to make a vertical indentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have been at a stable weight for years and I don’t smoke. I lift weights 4 times a week. I had 5 children at 10 to 11 pounds each. I grew up not wearing sunscreen so age, pregnancy, weight loss, and sun damage caused me to have loose skin. I’ve been told I can’t have a BBL because there is not enough fat.
Would you be able to help me? Not sure if I need a lower buttock lift only or if implants are necessary. I look okay in photos- which is why I sent them- but definitely not in a bikini or naked. I was excited to find you online because you are exactly whom I was looking for- your skills fit what I’m wanting.
I am willing to travel if you think I am a candidate for your expertise. I look forward to hearing from you.
A:The key to understanding buttock reshaping procedures is what areas they affect. Per the diagram implants affect only the top ½ or 2/3s of the buttocks while lifts/tucks affect only the bottom third of the buttocks.
That being said when you look at your buttocks, while they are a bit flatter in projection, there is significant ptosis or sag at their lower pole and I would view that as the bigger of the two issues. Thus lower buttock lifts are more indicated for you and you do that first and then see what you thinl about implant augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have been experimenting with eye area aesthetics lately and have thought about what you said last time, that you do not need to have “true ptosis” to have ptosis correction surgery on the upper eyelids. I believe an optimal correction for my case would be to raise my upper eyelids to show 0.5-1 mm more of my iris. I would like to know the following:
1. Is the type of ptosis correction shown in the morphs below reasonable to expect for my case? This is slightly less than 1 mm.
2. What is the anatomic limit to how far the eyelids can be raised? If the Levator muscle is already tight, Can it still be tightened more?
3. Would I be a candidate for the Y-V lacrimal advancement you suggested to extend the lacrimal lake towards the nose?
A:In answer to your questions:
1) It is hard to appreciate in your morphs the upper eyelid change that a 1mm elevation would create. But suffice it to say that such modest upper eyelid lifting in a normal eyelid should be possible.
2) The anatomic limits of upper eyelid lifting in normal eyes is not known since it is rarely done. But modest amounts would certainly be within the anatomic limits.
3) Y-V inner eyelid lengthening can really be done in anyone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would you mind letting me know if it’s possible To reduce height of the top of my head ? It’s high in height sort of cone shape and I want it reduced and more rounded. I have attached an edited photo to illustrate is this much seem doable? Left side is my current shape right is edit.
A:Such an amount of head height reduction is possible provided the skull bone is thick enough to do so. It would take a preoperative 2D CT scan to make provide a definitive answer to that question.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to inquire about a potential reconstructive surgery to reposition soft tissue and fat on my face, which has become displaced following cheek implant removal.
To provide some context, I previously had cheek implants, which involved creating pockets that required the dissection of the attachments to my soft tissue and fat from the bone. When the implants were removed six months later in 2016, the tissues were not sutured or reattached, leading to significant sliding, sagging and displacement of my facial soft tissue and fat. I went on to have a mid-face lift with another surgeon in 2019, who recommended remedying this. I loved the result (I no longer need or wish for implants). The procedure worked wonderfully to give me a side projection in my profile. It, however, did little to address the heavy nasio-labial folds or any of the soft tissue descent in the front of my face. I accepted these changes and moved on while secretly hoping one day I could put my soft tissue back where it slid from. I came across your blog and read about soft tissue resuspension, and I am very interested! I’m crossing my fingers that you can provide this. There is very little info or doctors who understand or offer this reconstructive need. I am grateful I came across your page and hopeful that you may be able to help me resolve this after so many years.
Thank you very much for your time, and I look forward to hearing from you
A:I think after having a midface lift you have maximized whatever amount of soft tissue reposiitioning that can be achieved. The change in the nasolabial folds is not really reversible and, in theory, was also what a midface lift was designed to effect. (which it really can’t) There is no otehr procedure that can.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For a little over a year now I’ve had what I believe to be enlarged temporal arteries on both sides. I’ve had no headaches, tenderness, or any vision problems.
They fluctuate in size, if the temperature is hot, if I’m being active, or anxious they become very noticeable. On the other hand if I’m at home in the AC they can become almost unnoticeable. So I’m reaching out to see if temporal artery ligation would be an option for me.
A:Your temporal artery presentation and history is classic. The only variation in temporal artery ligation in your case is the level or number of ligation points that may be needed because of your shaved head. How far they go up into the scalp is more apparent in your case.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, 13 years ago I got a chin implant made from mersilene mesh. I got an resorption (about 13 mm long). I do not have big symptons and it was an accidental discovery. I spoke with two maxillofacial surgeons but they do not have experience taking off mersilene implants and the plastic surgeon that put the implant in first place, I spoke with him and he does not know how to take that off. Is there any chance that the doctor will analyze my case?
A:Mersilene mesh chin implants can be removed, I have removed many, I would remove your mesh and fill in the bone defects with cadaveric bone chips for ‘reconstruction’.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, After my cheek implant removal I had a midface lift to help with the cheek sagging. While the mid-face lift did help reposition the deeper layers of my face, the more superficial soft tissue and fat remains significantly lower than the deeper layers of muscle on my face.
I’ve been using PDO thread lifts a couple of times a year to temporarily lift this tissue, and while I love the results and it perfectly addresses my concerns, it doesn’t last and isn’t cost effective long term.
I’m wondering if an intraoral incision with the use of an Endotine or sutures could reposition and secure the soft tissue to the SMAS for a more lasting result. I believe it was this layer that was not addressed during my mid face lift and it was this layer that got disconnected when pockets for the implants were created in my face.
A:The Temporal Endotine Midface Lifting technique is like any deep plane facelift approach…it elevates the deeper tissues as its effect are at the subperiosteal plane level. Your PDO threads have been effective because they are at a superficial tissue level which the Endotine device will not affect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve been just super insecure about my lips for awhile they’re just not wide and I feel like it just throws my face off. My questions are how much is pricing typically and is this a life long thing or will it go away after awhile. Thanks
A:You are undoubtably referring to mouth widening surgery. I would need to see a front view picture of your face to do imaging to see how much mouth width can be added. Mouth widening surgery creates permanent results but also some small permanent scars as a result. Thus the quetsion is not about the permanency of the increased mouth width but whether the permanent scars to do so are a good aesthetic tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in a sliding genioplasty. My occlusion or bite is fine( as far as I know and have been told.My chin has never been operated on or i.e. a virgin chin that I think needs only minimal to moderate changes in order to harmonize and balance my face.
Having said that;I think I have a mild to moderate short face syndrome as evidenced by these pics taken by max surgeon on Sep 2024. He claims I have no vertical deficiency at all based on his software but he agrees that I have about a 4 to 5 mm horizontal deficiency.
It’s confusing and frustrating because about 9 years ago another max surgeon did no cephalic study but just eyeballed me during the consultation and confidently proclaimed 4mm to 5mm horizontally but about 8mm to 10 mm on the vertical but he also said he would back the estimate it with a study.
What do you think? I’m just trying to be logical, prudent and practical here.
A:Like all aesthetic issues it is what the patient perceives, not what numbers/measurements or a doctor says is so. From that perspective I like to dive into imaging and see how the patient responds to some changes. (see attached chin augmentation changes which includes vertical lengthening) One can debate about about how much vertical lengthening is desired and how to do it…but that is not initially relevant. The first step is to determine if any amount of vertical chin lengthening is desirable from your perspective.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I have a webbed neck and would like to learn more about the surgical procedure. I have not been diagnosed with Turner’s Syndrome, however I was also never tested. I am very self-conscious about it and would love to improve the look and functionality of my neck.
A: First, webbed neck surgery is done to improve the appearance of the webs. It does not, however, improve the function of the neck. (e.g., range of motion)
Thank you for sending your pictures. Non-syndromic webbed necks, also known as mosiacs, usually have stiffer or non-flexible tissues. Thus, even though the smaller neck webs would seem to be the most improvable, they usually are the most resistant. That is my general experience based on your pictures alone. But the effectiveness of webbed neck surgery ultimately depends on how mobile the posterior neck tissues are which obviously can’t be assessed in pictures.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My goal is to do this surgery. I hope you can help me to get red of rejection among people . Honestly I live hard live because of my skull shape. I wonder could you fix all this destruction on my skull. How much the possibility to have a good shape after surgery?
A: What you have is classic plagiocephaly with a left craniocoliosis rotation in which the left back side of the head is flatter and the left temporal and forehead is more protrusive/pushed forward. For the back of the head a custom skull implant it out is the standard approach. For the front of the head there are two options: 1) reduce the left forehead or 2) build up the right forehead. That choice is based on what the patient sees as the best aesthetic appearance.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I had maxillofacial surgery twice to increase size of chin. There is something that is missing on the jawline. I was thinking that an implant may help
A:I believe what you are saying is that you have had two bony genioplasties to increase your chin projection. In so doing what often happens is that a bony stepoff develops at the back end of the osteotomy cut from the advanced bone. Such a bony stepoff becomes more evident the larger the chin advancement becomes. You are correct in that the management of the bony stepoffs requires implant coverage. The only question is how best to make an implant for both to do so. A custom implant design is always the most accurate way to do it. But before any treatment option is considered a 3D CT scan of your chin should be done to have a complete visual understanding of the jawline defects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon