Your Questions
Your Questions
Q: Dr. Eppley, I did a chin implant recently and I chose EAC L, which doesn’t seem sufficient – things look smaller and thinner still and not tall enough. Flowers Glove offers 1.75 cm of height and significant mass, but people’s chin looks like a potato or golf ball and is not as athletic afterwards. I think my next move is a custom implant. To do this right, I need imaging (not 3D, on my real picture), to see what the custom implant will roughly do. My current surgeon does not offer such imaging – do you? Attached pics are from now, which is 2 months after surgery.
A:Thank you for your inquiry and sending your pictures. The fundamental dimensional problem of your current chin implant result is that it lacks vertical height. Vertical height refers to an extension of the inferior border of the bone. No standard implant really does that satisfactorily. You simply have had a chin implant which has been placed with no real consideration of the need for vertical lengthening in which you have always had a vertically short chin.
When it comes to imaging it is important to understand that its purpose is to determine the patients goals not to show a result that will actually happen as no one knows that for certain. Imaging determines the target which serves as the type of surgery that the surgeon thinks is most likely to come closest to achieving. In that regard I have attached an image in which I am demonstrating some increased vertical height to the chin augmentation results you already have which appears to be adequate from the standpoint of horizontal projection.
Ultimately you will need a 3-D CT scan so we can understand what your current implant is actually doing based upon the way it is positioned on the bone. Whether such an imaged change can be achieved by a custom implant or whether it may require a vertical lengthening bony genioplasty remains to be determined of which the 3-D scan will provide invaluable information on that decision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about mandible implant width size. To create an angular apearence on my jaw, would 5mm width do it? I have read thats very small when it comes to mandible implants. What size is needed?
A:To make the determination as to how much width may be necessary in the jaw angle area it really takes imaging of the patient’s pictures to determine the result you were seeking from which an estimate can then be provided as to what that width number may be. As I don’t know what you look like I can only make a general statement of which it would be fair to say a 5 mm jaw angle width in most men is unlikely to create an angular jaw angle appearance. But every patient is different and must be evaluated on their own.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about testicular enhancement. I would like to get this done as I’m not happy with my size and want them to be larger. I have had a prior vasectomy and I do not ever want children. I also have a family history of prostate cancer too. I read somewhere removing testicles could help reduce risk. I really don’t want to get cancer ever. Would it be possible to remove mine and then replace them with much bigger implants? I wouldn’t want the side by side technique because I don’t want to have 4 balls in scrotum. I also don’t know about the wrap around thing. I think that would be harder to detect testicular cancer and I’m nervous I wouldn’t be able to tell if it was inside an implant. I wouldn’t be able to feel anything abnormal I think. Would it be possible for removal for my goal of 100% sterilization and hopefully reduce cancer risk and also make room for the implants? I don’t mind taking a little bit of testosterone on the side to have some level of that. My levels are low anyway.
Thank you very much. I appreciate it.
A:Thank you for your inquiry. In answer to your questions you certainly can have existing testicles removed and immediately replaced with implants that are larger than that of the natural testicles. That would achieve two of the three goals you have mentioned including assurance of 100% sterilization and to make room for implants. While removing the testicles will certainly eliminate any chance of testicular cancer I would not think that that would similarly reduce the risk of prostate cancer given that emanates from a different anatomic structure. There may be a correlation in terms of cancer reduction but I am not aware of it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I received a bilateral iliac crest reduction about 1.5 years ago and love the result! The reduction was approximately 1cm from each crest and the recovery was very speedy. I am highly interested in another reduction of both crests, but I do understand there are limitations of how much bone can be removed. My aesthetic ideal would be an additional 1cm removed, but is this feasible? If not 1cm, what is the feasible amount of bone an aggressive approach could remove? Thank you for your time!
A:Thank you for the long term follow-up and I am glad to hear that the initial iliac crest reduction was satisfactory. In regards to a second iliac crest reduction I can only speculate as to its feasibility since I have never yet done it. I think the question is not whether some more iliac crest bone can be taken but how much and can as much as an additional 1 cm be done. My conjecture would be…maybe. But I don’ t think one could every know exactly how much more bone can be taken until one is actually doing it in surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had jaw augmentation done by you several years ago (bony genioplasty and custom jawline implant). a I’m happy with the added volume of the mandibular implants, but I’d like a sharper jawline, especially when viewed from the side, as the jaw–neck transition still feels a bit soft. I wanted to know:
* What options might help improve jawline definition while keeping the implants?
* Could a neck/ lower face lift meaningfully help in my case?What challenges would a neck/lower face lift present given my existing mandibular implants, which I would prefer to keep?
A:Thank you for the long term follow-up. I would need to see some current pictures of your face to better answer your question. However I would suspect that you have maximized the effectiveness of jaw augmentation. While increasing the size of your current jaw augmentation does stretch out the skin and would improve definition there is a point where the jaw augmentation becomes disproportionately large…not to mention it is not a prudent choice with a surgical result that is working well and has had an uncomplicated course.
Therefore I can certainly understand your focus on soft tissue management and we know you have thick overlying soft tissues. The question is not whether you can have a lower facelift, as jaw augmentation does not preclude any overlying soft tissue management. The real question is how effective would it be and are the auricular scars required to do the procedure worth the trade-off for the benefits. That requires some careful consideration.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a sliding genioplasty two years ago and have tightness in the area. Original surgeon said it could be the plate and wanted to do removal but from my research it seems I have a soft tissue deficiency which is causing the tightness and a ball like appearance.
A:While I don’t know what you looked like before the chin procedure and I don’t know the amount that your chin bone was moved but the two concerns you have concern have different etiologies. The tightness may be related to a soft tissue deficiency because of contracture into the bonus step off if the advancement was significant enough. The ball appearance of the chin is simply the natural shape of the soft tissue chin pad being exaggerated due to the central increased projection of the bone underneath it. There’s not really a solution for this concern.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have had two prior submental chin pad reduction procedures, which provided improvement, but I sought more. I made the mistake of going to a different surgeon who I was going to for a different procedure, and mentioned I was still unhappy with soft tissue in my chin. He told me he would bring my bone forward just so the soft tissue would have support. He was adamant there wouldn’t be any significant projection to my side profile, if any. However, he not only projected my chin significantly from the side, but it now is longer than it was previously. I am so unhappy with how I look now and obviously regret choosing a surgeon who told me projecting my chin would help me. My question is, would it be possible to at least somewhat reverse what he did to me? Clearly I will not be going back to him, and I was hoping you may have some advice. I have attached my operative report. I went to a consultation with another surgeon recently and he told me that I was still very swollen since my surgery. But he only does chin shaving, Also, I don’t think any decrease in swelling would do anything substantial to the shape of my chin now. I would appreciate any suggestions or thoughts from you. Thank you.
A:The logic of how you could move the chin bone forward by any amount and not change the side profile it Is a bit of a mystery to me. Your chin bone was advanced 4 mm forward and 2 mm vertically. Together that would certainly make a noticeable difference in projection even though that is a not large bony movement as bony genioplasties go. Since the surgery was done almost a year ago there really is no residual swelling. So whatever you see now is a direct effect of the bony chin movement. The options now are to either reversed the bony genioplasty by intraoral osteotomy or take advantage of the existing submental scar and do a bone shaving of the amount of movement that was done as well as perhaps remove some additional soft tissue chin pad.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing about chin and neck surgery but I have a few questions. I have been doing a lot of research about what procedure I should get done exactly. ]I am not sure if I need a sliding genioplasty, liposuction, or both. Please let me know what would be the best route for me with my chin situation.
A:I don’t think there is any question with your horizontally and vertically short chin that you can’t accomplish anything with your neck if you don’t do a bony chin movement. For your neck you likely only need liposuction, and at worst, a submentoplasty. The key is the horizontal and vertical advancement of your chin which is going to help out your neck by the attached muscle pull as the chin bone moves forward.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,My question for Dr. Eppley is whether or not penoscrotal web repair/scrotoplasty is available for a patient (myself) with a small varicocele as this affliction is causing increasingly painful intercourse along with toilet submerges/constant discomfort while I am unable to locate a local provider familiar with the procedure
A: Until I see some actual pictures of your penoscrotal webbing/Loose scrotal tissues I would assume that addressing these issues as possible as they would be for almost anybody. As it relates to the varicocele this is not a condition that I treat so if this is a a significant contributor to your discomfort that should be addressed first by a Urologist who is much more familiar with treating it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a genioplasty in S. Korea to shorten my chin and reduce my lower facial thirds two months ago, since it was too long in my opinion. While the Dr was able to successfully reduce my chin vertically to a length that I desire, I am not happy with my 45 degree profile and side profile, since my chin was shaved inwards, and now looks recessed and gives me the appearance of a double chin. I have contemplated fillers vs an implant vs sliding genio. I concluded that I cannot get a sliding genio since my chin now doesn’t have enough bone, and I also do not want fillers since their is risk of migration and touch-ups which can be expensive. I am thinking of getting an implant, but that however also runs the risk bone re-asorbtion, the implant moving, etc. I actually already have titanium implants in my jawline six months ago as well and they have adapted to jaw angles quite well, so is that a sign that bone re-asorbtion is less of a risk for me? Am I an ideal candidate for a chin implant, and if so at what stage can I get it post-op; is it better to get it asap or later on? What material is best recommended for me? Attached are my CT scans pre-op and post-op from this procedure.
A.:How to augment a chin that is has had a prior mini V line surgery can be done in one of two ways. First you do have enough bone to do a secondary genioplasty to move it forward. This would be the correct procedure if the patient is opposed to an implant or has any implant– related concerns. It may be the more invasive procedure to do but your 3-D CT scan shows that it can be successfully done. The less invasive non-bone cutting procedure of course would be an implant of which I have no concerns about implant migration or any significant implant settling (the term bone erosion is a biologically flawed) this approach offers not only not repeating the bone cut but with a custom implant design control of every implant dimension.
I think the secondary chin augmentation choice comes down to your emotional preference as well as how much augmentation do you really need in terms of millimeters of advancement. Most likely and having done many female cases like yours it probably is a function in the 2 to 4 mm range at most.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I would like to get information about post-surgery recovery time and possible post-surgery complications about head widening surgery. I want to improve my narrow head shape from the forehead along the sides.
 A:Thank you for your inquiry and sending her pictures. Given your head shape and your augmentation goals you have selected the type of custom forehead – temporal implant that is best suited to treated. Having performed many of this type of head widening implants I can answer your questions as follows:
A:Thank you for your inquiry and sending her pictures. Given your head shape and your augmentation goals you have selected the type of custom forehead – temporal implant that is best suited to treated. Having performed many of this type of head widening implants I can answer your questions as follows:
1) the two main potential complications with this surgery is 1) short tern fluid collections, which is why drains are initially used for the first week after surgery and 2) more pertinently the potential for implant edge show where it ends on the forehead. It is the ladder that is a major emphasis for prevention not only in implant design but it as well for surgical placement.
2) Depending on how one chooses to define recovery there are two phases. The first phase is when will you be able to go out in public and look more normal and nonsurgical in nature and that will be in the 10 to 14 day time period. The second phase is when will you know everything about the outcome in terms of the true final results and that will be at the three month mark.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
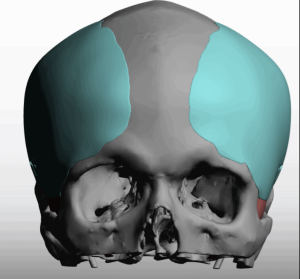
Q: Dr. Eppley, I noted my occipital bone pops out a bit and I realized that I have a bone popping out behind my ear just wanted to know if it’s doable to fix this.
A: When you refer to the bone popping out behind your ear you likely are referring to the mastoid process which I have highlighted in the picture with the yellow arrow. This protrusion is due to the enlargement of the air cells that exist in the mastoid bone. Due to the air cells in the bone it would be important to know how much of that protrusion is bone and how close is the underlying air cells before attempting any reduction. This would require a CT scan to answer that important question.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, You mention that a second genioplasty has identical risks to the first, would a third revision be the same or more risky? Will there be significant soft tissue changes and scarring by then? Especially with a bit of existing chin tightness already. Is this something you have performed before?
A:Since I don’t know what type of bone movements have been done in the first and second procedure nor what may be considered for the third I can’t really answer the question as to whether the risk are or more. However I do think it’s fair to say,mthat no matter what the tertiary bone movement may be you are not going to improve the tightness by whatever bony positional change is done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a young male, reaching out to inquire about Dr. Eppley! I’m a big fan of his work and believe his aesthetic eye matches my express transformational goals of a contoured, chiseled, slim face, jawline and neck. For context, I have a genetic chipmunk face and neck, despite being an athlete with <10% body fat. After doing diligent reading and studying, I am interested specifically in the following: 1. Aggressive cheek, jaw, jowls and submental liposuction 2. Deep plane neck lift / sub-platysmal work 3. Chin augmentation (Custom 3D-printed implant) 4. Buccal fat removal I had Orthognathic surgery with Sliding Genioplasty, I’ve attached photos for the Dr. in case they are helpful! Thank you so much for your help and consideration.
A:Thank you for your inquiry and sending your picture. With your type of facial shape and degree of lipodystrophy it is challenging to create defined facial shapes. As you have correctly surmised it is going to take a combination of skeletal augmentations and fat reductions to make the best possible improvement. I think, however, the ratio of the distributions between augmentation and defatting is a bit imbalanced in the plan you have propose. The key to remember is you cannot reduce a face for great definition. You have to have good definition to start or create it so that the reductions can more fully show the underlying structure. Well it is true that you need significant fat reductions via a submentoplasty, buccal lipectomies, perioral/lateral facial liposuction, and buccinator myectomies but these are really ancillary procedures to try to reveal more of what lies underneath. This is why you really need a wraparound jawline implant to more clearly separate the face from the neck and not just a chin augmentation alone. Beach and augmentation would certainly be beneficial but it only affects the project import of the chin I’m is not going to help anything with the structure behind.
The role of the deep plane facelift is very dubious in your case. I see a lot of young people believe that procedure is going to create create better facial definition when in fact it really won’t. It follows the basic principle that you cannot soft tissue reduce your way into better facial definition, you have to have it to start with. It is also important to remember that facelift surgery is based on having loose tissues which can be mobilized, relocvated and resuspended . In young people however that is rarely the case and the degree of improvement from it is far less. In other words it’s a lot of effort for a very limited benefit. That is a procedure that I would put as secondary and have all of the other things done first and then judge whether there’s some benefit to the procedure. The question is not whether hey deep playing facelift can be done but whether that degree of effort is worth it
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is there such thing as iliac pelvic shaving/reduction for aesthetic reasons ?
A:Iliac crest reduction and augmentation are viable aesthetic procedures that I have performed many times.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I did some filler injections to my jaw angles but am now considering a jaw angle implants for more definition, rather than injecting any more fillers. I’m interested in a conservative vertical jaw angle implant that increases drop, not width. I do not want lateral flare. But I do like more definition and a sharper angle.
A:Thank you for your inquiry and sending your pictures. By definition while you can have vertical jaw angle lengthening you cannot do so without adding some width. You simply cannot hang an implant off of the bottom edge of the ajw angle area. It must have a flange of a certain width that engages the bone above it to be able to be secured to it.
That being said are you a good candidate for such a jawline goal procedure??…. That may be questionable given your very thick tissues but I don’t think I can give a fair answer looking at two pictures in which you are smiling and they don’t really show your jaw angle area in its native state. It would really take seeing some nonsmiling pictures in the front and side view.
What I do know is that, while you can achieve vertical jaw angle lengthening, does the trade-off of adding a little bit of with make that worthwhile or does it just cause another aesthetic concern. In your case there is a very precarious balance between trying to achieve vertical lengthening but without adding significant width that you may interpret as undesirable. My experience has been in in these delicate aesthetic balances there’s a 50% chance it is acceptable and an equal 50% chance that it is undesired.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a bald hairstyle, as I started balding quite young. I have noticed however that my side profile has quite a sloped look from the top of my forehead to the crown, and that it goes up into a peak. I feel this gives a bit of a pointy look, and the peak removes any nice rounded transition to the back.
A:I believe you are referring to a high crown area as per the attached picture. That cab usually be reduced provided the bone is thick enough to do so. That is determined by getting a 3D CT scan of the skull and performing bone thickness color mapping. This will answer the question of whether the procedure can be done safely and successfully.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am currently looking for an experienced surgeon and medical center specializing in custom implants. My main request concerns the reconstruction of the back of my skull. I have a flat occipital area, and I would like to place a custom-made implant in order to achieve a more rounded and harmonious head shape. Additionally, I am also interested in custom implants for my jawline, including the mandibular angles and the chin, to create a stronger and more structured facial contour.
I have already undergone a chin implant surgery in the past; however, the implant used was a standard, universal implant and does not match the proportions of my face. For this reason, I am specifically interested in fully custom-made implants designed according to my facial anatomy.
I would like to know:
• Whether these procedures are possible at your clinic
• How the process works (consultation, 3D planning, scans, surgery, recovery)
• Estimated costs and timelines
• Required length of stay in your country
A:Thank you for your inquiry, sending your pictures and detailing your specific aesthetic objectives. I have done over 1500 custom skull and facial implants with many of them jawline and for augmentation of the back of the head. In answer to your specific questions:
1) Such custom implants are made from a 3-D CT skull scan which I can see that you already have. I would just need the disc upon which the scanner information is on sent to me to do the implant designing.
2) The implant design process from the time I get the scan and have the implants ready for surgery would be a three-month time.
3) Both custom back of the head and jawline implants could be placed during the same surgery.
4) The cost of the surgery will be passed along to you later today.
5) if both procedures were performed together I would estimate that you be able to go home within one week after the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in facial balancing, particularly the midface area. I would like to address pronounced nasolabial folds and a flat midface.
A:Thank you for your inquiry and sending your pictures. There are numerous factors that go into the appearance of nasolabial folds any young person of which one of them is a flatter central midface projection. Lower pyriform aperture (premaxillary– paranasal) augmentation can be helpful in reducing the appearance of nasolabial folds although they will not completely eliminate them. A debate can be had as to whether such implants should be custom made or to use standard implants but that is a discussion for a later date.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, DomI need chin augmentation? Apparently, I am borderline. I mainly just want better definition not increased size.
A:There is nothing borderline about whether you have a weak projecting chin as it is deficient in both horizontally and vertically. The only thing borderline about it is from an aesthetic standpoint of how much chin augmentation you can accept if any. It is impossible to achieve better chin definition without an increase in size. Increased definition of any body part is always going to involve some change in the dimensions of its size.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Generally curious what procedures you would recommend given my complaint. I don’t like the ratio of my narrower and recessed forehead to my cheekbones and jaw width resulting in a big lower face. Not sure where to add or subtract from. I sometimes feel like my jaw is very wide but not sure if that is because my chin is a bit short and under projected for my face. I really don’t know if I would benefit from jaw shaving + chin implant versus a jaw implant that adds length to my face. Another question is cheekbone narrowing – would this give the results I want? I know it is common amongst asian people but I’m pretty wary of taking away what seems to hold up you whole face. It does seem to look good in photos. I don’t mind the anterior projection of my forehead, but hate how flat it looks at the 3/4 angle. At the same time not happy with the loose skin under my chin. Would a chin or jaw implant fill that loose skin and take care of the jowls? or would I need a neck lift in conjunction with the implant.
A: Thank you for your inquiry and sending your pictures. My initial reaction is that your needs are more reductive in nature rather than augmentation. My speculation is that what bothers you is the natural facial structural shape that is consistent with your ethnicity…. meaning the lower two thirds of your face is wider and more square. Thus while you can augment your forehead, in and of itself, that just takes your base concerns and magnifies them making the entire face broader. The focus is on your mid and lower face of which you have a flat mandibular plane angle which makes for a broader lower jaw and naturally wider cheeks.. While n there may be a role for some vertical chin lengthening cheek and jaw angle reductions are the methods to narrow your lower face.
To summarize my initial reactions are: 1) cheek and jawline goal reductions, 2) vertical chin lengthening and 3) moderate forehead augmentation to correct the shape and the three-quarter view. This will certainly help the submental and jowl areas in regards to loose soft tissue.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, it’s great stumbling on your website. I do have a similar horizontal indentation on the top of my head and I wonder if your plastic surgery would not only fix the aesthetic concern but headaches, and migraines like symptoms (sensitivity to light, sound and smell) that appear to be exacerbated by the indentation. I will sincerely appreciate your feedback
A:This is the classic indentation across across the coronal suture line on the top of the head between the bony temporal lines. This is an aesthetic skull deformity that is not known to be associated with any functional issues. Thus fixing the skull contour defect by a custom skull implant would not be expected to cause any change in your headaches or other symptoms.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I wanted to ask a question about facial asymmetry and possible procedures to address it. On one side of my face, my eye sits lower, along with the eyebrow, eyelid, and cheekbone. I was wondering which procedure would be best to correct this. I’ve read about combining an orbital rim implant with a cheek implant. However, I’m concerned that if the eye is raised with an orbital rim implant, the eyebrow and eyelid—since they are already lower—might appear more covered. In that case, I understand that an eyebrow lift might also be needed to bring the eyebrow and eyelid to the same level as the other side. This approach could make the eye and cheekbone more symmetrical, but the eyebrows might still be uneven. That led me to wonder whether fat transfer to the opposite eyebrow and eyelid could be an option. By adding volume to that side, it might lower the eyebrow slightly and help both eyebrows and eyelids sit at the same level. Is that something that would be possible?
A:What you are describing is classic vertical orbital dystopia, which means the entire orbital box in all of the soft tissues around it are low. As you have correctly surmised correcting the orbital floor, rim and cheek bone positioning by a custom-made implant is not the total solution to the problem. In fact that alone will likely make it look more apparent because you have to change all the soft tissues around it including the upper and lower eyelids as well as the eyebrow. to look right with the implant induced changes. Thus most cases of vertical orbital dystopia surgery must be comprehensive of which the implant is but one part of it.
Fat grafting of the opposite eyelid is not going to make it lower. It will merely make it look fuller. As a general rule for almost all cases of any type of facial asymmetry you do not usually try to improve it by changing the good side. That being said this is a general guideline of which how about exactly replies to you is unknown since I’ve never seen a picture of your eye asymmetry.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am scheduled (this upcoming week) to have a mid-facelift with a fat transfer and buccal fat removal. During the initialconsultation, the surgeon mentioned that based on the look and projection I’m looking to achieve, facial implants might be needed. He also advised to have the implant procedure done a few months after the mid-facelift and fat transfer, so we can better determine more accurately the implant specifications once the swelling and fat transfer have subsided. The implant and placement that I’m interested in is a thin, elongated implant to be placed right under the temple and extend on the high point of the cheeks.
Here are my questions:
- Is there a benefit to having 2 separate procedures, one for the facelift and the other for the implants? (I prefer to have one procedure to prevent another anesthesia)
- Is there a possibility to not need a fat transfer at all if implants are used?
- Where will the incision be for the implant? Through the hairline, mouth, or inner lower eyelid?
- Is there an option to use Porous polyethylene instead of silicone?
A:Thank you for your inquiry and sending your pictures. The first and most important question is what exactly are you trying to achieve. I could probably guess based on the procedures that are being considered as well as your young age and your pictures. However I really don’t want to guess and I need for you to tell me specifically what that is.
But some of the answers to your questions without knowing your goals I can say the following:
1) it is likely what is meant by that you may need facial implants is that if the first procedures aren’t effective for your goals then implants will need to be done later. That’s the question is not whether these procedures should be combined or separated but based upon your goals what is going to be the most effective approach. Until I know your exact goals it is impossible to say whether such procedures should be done together, separate, or whether only one of them should ever be done.
2) One of the basic reasons for implants as to avoid the use of fat or filler injections later… Provided the area of augmentation needed is in the zone where the implants are placed.
3) Since I don’t know what your goals are for the type of implant that is being considered here I cannot yet say what would be the access to place it.
4) While porous polyethylene is always an option in any type of facial implant augmentation it generally it’s not a good choice in my experience because of its extreme difficulty in secondary modification or removal. And although everybody thinks they would never be the patient who would need their implants revised the reality is there is a 40% risk of that occurring which makes it not rare. In addition if one is having implants in the mid facial area due to the thin tissues porous polyethylene does not have feather edging by virtue of the way it is manufactured which means means there will be a palpable and sometimes visible edge to them. Tissue ingrowth into an implant material always sounds good provided the implant positioning, shape and size is perfect and you never have to touch them again for as long as you live. But when any secondary changes are needed tissue ingrowth becomes a major liability and no longer an asset.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, When you say 50% chance of success, meaning 50% chance of other complications left with more/other problems worse than before? Have you had patients left worse than before? Any successful cases you could share pictures or is it all confidential? How does the recovery process looks like?
A:The 50% success rate in mentalis resuspension refers to that in those with an unfavorable outcome they relapse back the where they started…. never worst just not any better.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My current atrophied testicles are quite small.My testicles have atrophied a lot. They are very small. About 10 years ago I had some type of inhjectabole filler placed into the skin of the scrotum. I was never told exactly what the filler was but it was allegedly a filler that promotes collagen growth. As a result my scrotum skin has remained quite thick.
I would like to increase my testicle size. Considering the current size of my testicles and my desired implant size, is the wraparound method even possible?
I like the idea of this method but my concerns / questions about this method are:
If I come off TRT and get my natural testosterone levels back up with the help of HCG (or whatever else I need to take), I fear my testicles either not being able to grow, or getting crushed as they grow, and it just being uncomfortable. Is this fear justified?
I fear not being able to feel for testicular cancer… am I correct that this would make it impossible? Are there any other ways to check for testicular cancer? Would I have to get an MRI or x-ray if I wanted.
A:Thank you for your testicular size information. Testicles of that small size would not be a candidate for the wraparound implant method as they are at a high risk of slipping out of the implant encasement. In addition if there is any chance that the testicle size could go up or down based on hormone therapy that is another contraindication for the wraparound augmentation method. Only the testicular implant displacement method would be appropriate in your case
I don’t know exactly what injectable material was placed into or around your scrotal skin but when you use the term micro injections you are likely referring to silicone oil. This is substantiated by the fact that the scrotal skin has remained thick due to the persistence of injected material and the surrounding fibrous capsule that is created by it. The relevancy of having silicon in the scrotal skin is when you intervene with surgery the risk of infection is increased because of the silicone oil. While most of the silicon oil is encased away from the incision there undoubtably is some where the incision would be made.
As for the detection of testicular cancer any implants placed in the scrotum definitely has some negative effect on the ability to detect it. How significant that may be is not known. The implant displacement method is better in that regard as the natural testicles still remain ‘free’ and potentially palpable. The implants do bot interfere with the ability to do any diagnostic imaging such as ultrasound or MRIs/
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if I could get a quick opinion on the tragus and a SMAS facelift? Is it typical for a surgeon to cut off the top of the tragus during a facelift? Mine did and I’m not sure why? Photos attached. (Before pics are with yellow lines.) Wondering what your thoughts are. Thank you!
A:The goal of any facelift technique where a retrotragal incision is used is to preserve the tragal cartilage and shape. That obviously did not happen in your case. The why of it is a question for your surgeon to answer.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, would it be possible to add such a ‘mini’ implant to my under-eye area to address the hollowness? Right now honestly, the under-eyes are the one aspect of my face I find to be considerably deficient aesthetically even after IOM implants/fat transfers (i.e. the chin is not that bad all things considered). Fat transfers always leave a bit of hollowness after months.later so I was wondering if some smaller implants stacked on top of the existing IOMs could help with this in the same fashion as you discussed for the chin?
A:The residual undereye hollowing lies above the bone/implant level in the soft tissue area between the augmentation and the lashline of the lower lid which is what I believe to which you are referring. This is not an area in which hard structural augmentation is effective without causing potential lower eyelid mobility issues.. It requires soft tissue augmentation which is why you see fat injections some commonly used (abeit usually not effective) The alternative and more effective soft tissue augmentation methods include laying in a leager thicker Alloderm sheet or a thin dermal-fat graft across the entire lower eyelid.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a question regarding chin tightness after a revision chin reduction following an initial sliding genioplasty. As I have read your previous answers mentioning a lack of soft tissue causing the tightness, would a potential chin narrowing and height reduction procedure alleviate this symptom due to the reduced surface area that the soft tissue has to be stretched to cover – effectively mimicking having more soft tissue in the area? Or can this only be addressed with a fat graft? Thank you!
A:It’s a soft tissue deficiency/scar problem not a bone excess problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if it would be possible (and if so what the main issues would be) to make a low osteotomy on the iliac crest and then rotate it inwards as a mean to achieve a greater hip reduction than it’s currently offered with the iliac crest resection method. In the attached file there’s the visual representation of what I mean. At the right is the unmodified hip and at the left the modified hip where I show two versions of the same idea, one (left) where the osteotomy goes above the ASIS process and the other (right) where the osteotomy does not go through the ASIS but below it and above the AIIS. The right one is probably the better option as it would allow for a bigger reduction and it would not mess with the process destined to support the TFL, sartorius muscle and the inguinal ligament. I’m also wondering if the gluteus muscles like the gluteus medius and the iliacus muscle on the iliac fossa would be a problem. Also, maybe rehabilitation would be harder because of the stretching of the muscles and ligaments. Thanks for your time.
A:Thank you for your thoughtful inquiry in regards to the iliac crest osteotomy. I would not disagree with you from a conceptual standpoint and clearly the one where the osteotomy line leaves the ASIS intact would be the more effective one in terms of inward movement and it is obviously prudent to leave the inguinal ligament attachment intact. Technically this would be more of a bone cut and tilting the iliac crest inward with the placement of inter-positional grafts (cadaveric bone chips) in the opening wedge that is created. I could see some issues trying to just push the iliac crest inward because of what lies on inner surface of the pelvis. But, quite frankly until you actually do it it’s hard to say which bony movement can actually be done with greater ease. This obviously would require some plate fixation.
I see only two potential issues with this approach really crest reduction. The first is you would have to strip off all of the TFL fascial attachments along the crest to expose the bone for the osteotomy cut. Whether they could be put back by suture suspension to the crest is unknown, and if not, what does that mean for postoperative ambulation. Secondly, how much greater benefit comes from moving the bony crest inward as opposed to shaving reduction. Theoretically you would think you would but I would not be so certain. A fair amount of bone can be shaved off laterally that easily exceeds one cm. On the 3-D model you have to actually simulate both of them and see how much different it really is. In other words is the greater effort involved in the iliac crest osteotomy worth the additional improvements that provides over that are shaving. Like all aesthetic procedures the risk to benefit ratio must be very carefully calculated. And in iliac crest shaving reduction there have never been any significant aesthetic or functional issues.
Dr. Barry Eppley
World-Renowned Plastic Surgeon