Your Questions
Your Questions
Q: Dr. Eppley, . thank you for all the great work you’ve done. I read your articles on the midfacial mask implant, and i’d like your opinion on the following surgical plan: (1) first I will get a lefort 4 (monobloc advancement), to move essentially the entire skull forward. I was going to get a lefort 3 done at first but the monobloc will produce a better “hunter eyes effect” as it will move the whole orbital bone forward. Can you recommend me a skilled surgeon for this? I already found a few in the UK, but I would trust your suggestion more. (2) then after I recover from The monobloc I will have you install your midfacial mask implant. I look forward to hearing your opinion.
A: I think you will find it very difficult if not impossible to find any surgeon that would do a LeFort III or mono bloc advancement in an adult for aesthetic purposes. While the surgery may seem like a carpentry project on.a skeletal diagram there are major risks for this type of surgery not to mention the numerous adverse aesthetic sequelae from it.
Dr. Barty Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a fun shaped head. When i was younger i had a soft spot and my mom tried to shape it and made it worse. So im looking to speak to someone about potentially getting it shaped evenly
A: I have seen your pictures and it appears you have an asymmetric skull shape wirh the top right flatter than the left side. This requires a custom skull implant to correct.
Dr. Barty Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, had a tummy tuck/lipo 360 last May and I believe fluid has gathered, not just fat in the pubic area causing it to be enlarged and raised. I have read online you have a treatment for this as an outpatient, and I need a consultation.
A: Chronic untreated seromas can result in a bursa cavity which in a tummy tuck will end up low and in the center. The definitive treatment is to open part of the tummy tuck incision, excise the entire bursa lining and then quilt by suture the excised tissue cavity down with or withoiut a drain.
These are basic plastic surgery principles so I would assume your surgeon can make the diagnosis and perform the necessary surgical intervention.
Dr. Barty Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would love to lengthen the forehead with 2cms and without lifting the brows. Which technique would you use?.
A: Such a big movement would definitely require a 1sst stage tissue expander of the upper forehead and anterior scalp…followed 6 to 8 weeks later with its removal and the expanded forehead flap moved up into the hairline.
Dr. Barty Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I want to get customized implants after a very unlucky surgery done in Korea cheekbone reduction and chin reduction which took my beauty of me I am in a need for a good surgeon who can reverse the suregery within custom implants
A: I have done numerous custom implants for overdone or undesired facial bone reduction results. Chin, jaw and cheek reductions are the most common. Such implant designs are done from a postop 3D CT scan. Do you have one?
Dr. Barty Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, is it possible to see photos difference between the lateral and widening mandible implants from implantech? I am trying to decide which I would to have a consult about.
A: Looking at other patient results is not a good way to determine how any implant will change the patient’s face as everyone’s anatomy and facial shape is different. This is particularly relevant when it comes to the differences in the jaw angles. The most accurate method is to do imaging on your face of the differences between widening and lengthening of the jaw angle patrticularly from the front and ¾ views.
Dr. Barty Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 43 old male who had surgery of my central arch cancer and the entire lower jaw and lip was removed. I got surgery for jaw reconstruction from fibula bone. But after 10 days blood supply was stopped to jaw and fibula bone was removed. At same time skin grafting surgery was done in mouth. I am still unable to eat, drink properly and talk properly. I am keep medical cotton piece in my mouth becouse of a saliva is come out from mouth. Is a titanium jaw implant possible?
A: Any type of jaw implant, regardless of the material, requires good soft tissue coverage to be successful. With the loss of soft tissue from the cancer resection an implant will not work and the fibular bone flap was the correct reconstructive procedure…even if it was not successful. Further flap reconstruction efforts are what is needed not an implant.
Dr. Barty Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi! I was wondering do you do forehead lengthening procedure? I had a forehead reduction in the past. But i think my forehead is too low now.
A:Forehead lengthening can be performed three different ways, direct excision, an epicranial shift and tissue expansion technique, The direct excision works if the lower forehead and brow is lax, can be mobilized and one can tolerate a bit of a browlift result. The epicranial shift is like a reverse endoscopic browlift procedure using wide subperiosteal undermining and shifting the whole scalp backwards. Tissue expansion works by creating more upper forehead skin/scalp so either the direct excision or epicranial shift methods works better. Which technique is best depends on how forehead length you need.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to inquire about mouth reduction surgery. It is very wide when smiling.
A:Two important issues about mouth reduction:
1) The scars for mouth reduction are not good and I would be very cautious about ever doing it as a result. You will likely make the adverse aesthetic tradeoff of a problem you dislike just as much or worse than the problem you are trying to improve,
2) You never do a static operation for a dynamic problem. Any surgery works best when the problem being treated is best seen static (non-smiling) as that is how the surgery is performed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a right pectoralis major tendon tear in last year. My orthopedic surgeon repaired the tendon and I am back to training chest however I have some deformity and am hoping to get xxl pectoral implants. I also have some bilateral nipple deformity from having pierced nipples. I’m wondering if the xxl (largest possible) pectoral implants and nipple augmentation could be completed at the same time. I like large pointy nipples and I’d like mine to look more uniform. Currently as you can see in the pictures they have scars from the piercing that’s almost looks like a 3rd nipple. I’m hoping you can do pectoral implants and nipple correction while increasing the length and size and symmetry of the nipples as well. Thank you!
A:The concept of XXL pectoral implants is open to interpretation as to what that actual implant size is. But what is most relevant is whether the XXL implant is the largest standard (Powerflex Plus, 690ccs) or whether a custom implant must be made. I think you would probably be fine with the off-the-shelf PowerFlex Plus implant. With your height, chest size and thick strong tight pectoral muscles that would be the most implant you could probably get in. It is the ‘big daddy’ of standard pectoral implants made for the male seeking XL or XL size.
While numerous forms of nipple plasty can be performed at the time of pectoral implant placements the combination of a pierced nipple repair and nipple elongation can be problematic. (as nipple elongation usually requires placing a graft)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am 18 year old guy, and it has been pointed out to be that i have a convex profile, this makes my nose look bigger witch i hate. My facial convexity angle is about 159 and i was hoping there was a way i could get it to 165. And i was a permeant solution filler is not an option for me. I wouldn’t mind surgery if i needed it, but i also don’t know weather my sutures are closed. Any advice is appreciated.
A:With a convex facial profile this usually means there is a recessed chin as the primarily culprit. Surgical chin augmentation would be the only effective solution and the options are either a chin implant or a sliding genioplasty procedure. To verify is this is an effective approach as well as how much chin augmentation is needed I would need a side profile picture to do some imaging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am inquiring about the procedures for buried penis and testicular implants. I am 58 years old. Over the years my testicles have shrunk in size to the point where I have one testicle that is about 3.0 cm and the other is about 2.0 cm. The smaller one is sometimes hard to find due to its size. Does this situation sound like I am a good candidate for the displacement procedure? I think I have the required amount of space in the scrotal sac. If it is possible, I am interested in custom 7.5 cm testicle implants pending whether my scrotum has the space for them.
A: While in anatomic proximity and that surgical correction can be done at the same time your two objectives, testicular enhancement and buried penis repair, are very different. You are correct in that with small testicle sizes of 2 and 3 cms the implant displacement method will work very well. Whether your scrotum can accommodate the implant size of 7.5cms can never be known before surgery and we have to accept that inraoperative implant adjustment may be necessary if they don’t.
Buried penis repair can be done by either suprapubic liposuction, penile release and lengthening or both. What is best for you requires a picture assessment as well as an actual examination to make that decision. Since I only do the liposuction and not penile surgery I can only offer combined suprapubic liposuction and custom testicle implants in the same surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,Hi, I had lip lift and corner lip lift 1 year apart. Corner lip lift was done last fall. The extreme corners are downwards and makes me look sad. Is there a solution?
A:You just didn’t get enough lift from the lateral vermilion advancements/corner lifts. That needs to be repeated with a greater lateral arc to the lateral vermilion excision. You got enough initially out of it so that the upper lip vermilion show was balanced with the subnasal lip lift from one mouth corner to the other. It just needs more excision/lift.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, will you be performing the hip augmentation with the metal plates in the future?
 A: As for iliac crest hip augmentation with metal plates, this is a procedure I am currently performing since it has received FDA approval in the Spring of 2024. It is a composite skeletal and soft tissue hip augmentation method using a mental iliac crest plate with a silicone hip implant attached to it.
A: As for iliac crest hip augmentation with metal plates, this is a procedure I am currently performing since it has received FDA approval in the Spring of 2024. It is a composite skeletal and soft tissue hip augmentation method using a mental iliac crest plate with a silicone hip implant attached to it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in jaw implant. The main concern is that the jaw dips in before reaching the chin. My beard conceals it. I think my chin could be wider but it protrudes enough. My perception is that the gonial angle is wide enough though could reach a bit lower. I don’t want sharp angles because of my heritage. Its more about a well proportioned harmoneous fresh face not trying to make it more masculine . Well I mean a bit wider chin, not a square shape.
A: By your description this indicates that there is probably an extended antegonial notch shape of the mandible. A 3D CT scan would conform that descriptive supposition which is needed for a custom implant design. The value of custom implant designs is that they can be made for the exact anatomic defect regardless of what it is.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My concern is my right jaw as it looks shorter and smaller than my left jaw . My orthodontist said the only way to fix it is surgery or implants but he doesn’t recommend it. What about a mandible condylectomy?
A: You don’t violate/injury a functioning joint for an aesthetic jaw asymmetry concern. That would not be prudent medical choice.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,I was wondering if I can get more vertical length with my chin (about 2.5-3cm lower than my current chin) and to get the columella and tip of my nose marginally more parallel to the ground. I am not very good at photoshopping but I have just sent you 2 views. I like your oblique just that the chin has to be lower and the nose tip and columella marginally more parallel to the ground. Can you modify what you had sent me?
A:The key concept to understand about computer imaging is that it is not to show the patient the exact result that will happen as no one can predict that with 100% accuracy. The role of imaginng servesas a visual method to determine the patient’s goals and create an understanding of what can and can not be accomplished. Thus I can make the following comments to your response to my initial imaging.
In regards to vertical chin lengthening due to the restrictions of stretch of the soft tissue chin pad, one can get up to 7mms (0.7cm) of length with an implant and up to 15 -18mms (1.5 – 1.8cms) length with an intraoral vertical lengthening bony genioplasty. Thus getting 2 to 3cms of vertocal chin is never an achievable outcome. That is surgically not possible.
Again due to soft tissue restrictions (nasal trip skin) you can drive down the tip of the nose to a 90 degree nasolabial angle. There simply is not enough skin stretch to do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a septorhinoplasty along with custom facial implants. The primary motivation is correcting my deviated septum, but I’m also interested in the rhinoplasty aspect to reduce the hump and make the nose a little less projecting. Initially, I was planning to look into this procedure after the jaw/cheek procedure as it seemed like a lot to take on for one surgery. But I wanted to get your thoughts/advice if I could.
A:Combining a septorhinoplasty with custom facial implants can be done and it is not uncommon to do so. Whether one should so or not depends on multiple factors which ultimately comes down to the convenience of one surgery and whether the custom facial implants by their effect may preclude the need for any nose reshaping surgery. The question is not a medical one but a personal choice one.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a brow bone reduction surgery in 2014 which has had a few problems since then. Not sure if it was a type I or III. The goal was NOT to feminize my face. I have provided a pic of my brow bone before the surgery at age 35. I had a Liam Neeson brow. I have a depression at the top center incision line and also what appears to be grooves or cracks. I would need to have an open incision from ear to ear again, but the only way to resolve this.
My goals are to improve a more smoother more symmetrical MASCULINE even surface forehead from left to right
1.) take bone fragments pieces from top incision line indentation; reinsert them (bone grafting of my own bone material) to smooth out even to achieve a uniform contour.
2.) bone grafting of extended curved fractures from lower middle of forehead to arched upper outer forehead
3.) smooth out small bump on middle of far left forehead
4.) discuss right orbital add bone grafting technique to upper inner corner only (bone paste or bone cement, human tissue glue or donor bone from rib or hip) My left orbital rim is masculine, please do not change at all. My right orbital rim is feminine. This is due to a childhood trauma injury.
5.) may discuss adding a little bone grafting material to middle (between eyebrows) for a more masculine appearance
These ideas I would like an opportunity to discuss with you to consider your best practice approach and of your recommendations.
A: A needed 3D Ct scan scan will certainly show the bony contours/irregularities/defects that have resulted from a prior brow bone setback surgery. And while knowing those details are important, and all will be seen in surgery once exposed, the fundamental reconstruction decision is how to recontoiur the bone to a smooth and somewhat augmented appearance. While bone grafting is an option, and we are talking about harvesting cranial hone grafts, and its appeal is understandable it is not a great material to use for contouring. Cranial bone grafts are hard pieces of bone, have non-smooth edges, there is no great way to secure them and they will undergo some amount of resorption. (not structurally stable as an onlay graft) Cranial bone grafts are great for large inlay defects but not as a refined forehead contouring material. The far better choice is hydroxyapatite cement (HAC) which works like drywall putty when mixed, can smoothly fill in and augment any bony contour, is structurally stable when hardened (after 10 minutes of application) and the bone will bond to it due to its calcium phosphate mineral composition.
I will always do what the patient wants once when they have been fully informed of their options but in secondary brow bone/forehead contouring HAC is always the better material due to its smooth contouring capabilities.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I had a surgery to undue a lipoma on my head and the surgeon made an error in communication and shaved down my masculine profile slanting my head back and feminizing it day of surgery with electrical burr he called “bony prominences and shaving contouring” which I would of never wanted done again unfortunate miscommunication. I saw a picture of man that Dr Eppley did that gave me hope again a picture that looks like my old profile he did – I was wondering if what was done to me can be fixed I really want my old masculine profile back I would be interested in what the Dr thinks and was wondering if insurance covers this or how much for the bone cement implant to get it how it used to be above eyebrow and mid forehead. Before surgery is grey photo and with hat -and after is ones with black beanie shown Thank you please contact me asap I just want hope this can be fixed I am in California but would travel I really miss my old profile.
A:I am not sure how you go from a lipoma (osteoma??) excision to a complete forehead/brow bone reduction….but that is irrelevant now. In terms of restoration and the technique to do it it depends on the scope (surface area) of involvement and the contour change needed. HA cement works fine IF the needs is small and doesn’t require any contour other than a flat surface augmentation of limited thickness. Otherwise a custom forehead-brow bone implant is needed
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, i had double jaw surgery and custom mid face implants. Unfortunately im dealing with an issue that despite a sizeable infra-orbital implant – 5mm , i have significant depression and hollowness under the implant. My theory is that the ligaments were cut and the soft tissue/periosteum and fat pad sags below the implant, causing two issues 1) the shadows and sagging appearance and 2) lack of projection from the implant. When i pull my skin and fat up and back, the ogee curve is restored and the implant looks quite nice What do you think? Is this implant sagging from the surgeries? Or is my implant not big enough. I feel the lateral size of the implant is plenty large. Also one side is significantly worse than the other.
A: When you have an adverse aesthetic effect from an implant-related surgery it is always due to the same three potential issues….implant design, implant size and implant placement. Sometimes it is just one, two or all three. It is never due to anything else. The release of the osteocutaneous ligaments occurs in every facial implant surgery and a necessary component of bone or implant surgery so that is never the culprit.
I would know immediately the cause looking at your implant design and pictures of your face. The orbital area is an unforgiving area for implants due to the thin overlying soft tissues so it is easy to have design flaws, over/under sizing and/or incorrect or asymmetric placement that will be very visible.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I am interested in a forehead/brow/temple implant and nose hump implant. 4 years ago I had facial feminization surgery and nose hump reduction surgery and would like the reversal by adding more volume to my brow that is on top of my nose and adding a orbital rims and temple augmentation as well thru a scalp incision. I also wish to have my nose hump added without having to have an incision in my nostrils so if possible by adding it from the top of my head as well. Is this possible? And can you provide me with a quote?
A: My interpretation of your needs is the following:
1) Secondary Forehead-Brow Augmentation
2) Primary Temporal Augmentation
3) Secondary Nasal Augmentation. (is it frontonasal or lower at the dorsal hump area….I believe you mean the latter)
I assume from the prior surgery that a long scalp incision already exists.
Based on this general description I can’t yet say how this would be done…meaning is #3 part of #1 implant design or would it be separate? (I suspect it is separate…and probably could not be done from above in a satisfactory manner)
How does the temporal augmentation fit in with the forehead? Is it separate or is it connected to the forehead-brow bone augmentation?
As you can see there a lot of different moving parts here so it would impossible yet to provide any costs associated with these surgeries until I understand better what needs to be done. This requires a picture analysis with imaging done to determine your desired changes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I am a 44 year old male who eight years ago I had Medpor Chin, Jaw and Cheek implants and Rhinoplasty. I was extremely pleased with the result. But I had an infection two years ago and the jaw and chin implants had to be removed. I now wish to re-implant the jaw and chin. My research tells me PEEK may be superior to Medpor as I don’t want to have a repeat of an infection and removal.
A: PEEK is a fine facial implant material with its own advantages and disadvantages. Whether PEEK is superior to Medpor in terms of a lower risk of infection has never been scientifically validated.But in theory being non-porous it may be. But an implant is an implant is an implant no matter what the material is so the risk of infection can never be completely eliminated.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have facial asymmetry. Could custom implants improve my facial asymmetry? My right mandible is longer, and my cheekbone is farther back. The left side mandible is shorter, and the left cheekbone is more forward.
A: These are classic findings in facial asymmetry for which custom implant designs have great utility. But there are numerous augmentative and reductive approaches in facial asymmetry correction as well as unilateral and bilateral techniques But the first place to start is to get some face pictures for imaging followed by a 3D CT scan for further analysis and treatment planning.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I just had a sliding genio done last week. I had no idea it would make such a drastic difference on the appearance of my face from the front. I can’t recognize myself in the mirror anymore – my jaw is too rounded and my lips are smaller. I don’t love the side profile either, I feel like the surgeon advanced a bit too much. I think it was only 5mm unless he changed mid-procedure, and I’m hoping that’s a small enough movement to make reversal somewhat uncomplicated. My question is, how likely is it that I can get my old face back? I want to fully reverse. I’m 22 so I’m hoping my skin is elastic enough to look mostly the same after reversal. Also, I’m aware it’s still swollen, but I’m realizing far too late that I won’t like it regardless, because my face will be different from the front. Thank you so much.
A: The first concept to grasp is that at just one week after the surgery you are far removed from what the final result will be. There is a large amount of swelling at this point which will enlarge and distortt the entire chin area. Many sliding genioplasty patients at just one week after surgery do not feel that different than you do. Proper pre-surgical education would have informed you that you will feel that you have made a wrong decision up until 2 to 3 weeks after surgery win the swelling has gone down enough that you may be convinced a good result is possible. This is a classic postoperative phenomenon in many forms of facial structure or surgery. As a result I don’t recommend that patients try to reverse a procedure like a sliding genioplasty until at least six weeks after surgery when they have a better feel for what the result actually is. If still unsatisfied then a better decision can be made about whether a complete or subtotal reversal is best. It is important to remember that you did the procedure for a reason and this is why many patients that do not like their sliding genioplasty result usually opt for a subtotal reversal as opposed to a complete one.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I unfortunately inherited my mom’s sharper wider hips. It is in the actual bone structure and I have always hated it. Is there a way you can help me identify exactly what part of my hips are wide and also let me know if anything can be done? Thank you
A: These pictures show that that the ‘hip width’ concern is at the level of the greater trochanter of the femur (way below the iliac crest) which can not be surgically reduced without serious functional issues.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Wrap Around Implants – is it an option? The actual size impacts my self esteem and something I am searching about. How is it done?
A: Wraparound testicle implants are designed based on: 1) The patient’s desired size (external diameter) and 2) the patient’s natural size. (internal diameter of the hollow chamber) That is determined by a preoperative ultrasound for testicular size measurements.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Could you place implants behind the head to augment head volume please?
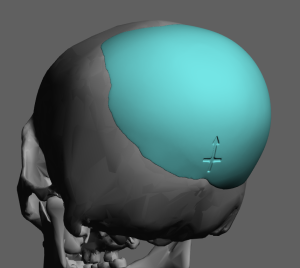 A: Custom back of the head skull implants is a procedure that I do all the time. The only question is how much volume is needed/desired and whether this can be done with an immediate implant placement or requires a 1st stage scalp expansion.
A: Custom back of the head skull implants is a procedure that I do all the time. The only question is how much volume is needed/desired and whether this can be done with an immediate implant placement or requires a 1st stage scalp expansion.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have two forehead bumps protruding I was wondering if my ct scan can be looked at and see if we can do anything about it thank you.
A: These are likely forehead horns since they are paired. (two of them) The qiestion is not whether they can undergo reduction but whether the bone is thick enough to allow complete reduction. Your 2D scan would provide that information with the slices that go through the forehead bump areas.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to remove potentially in the future around 2.5 mm of tissue around the nose to create a way slimmer nose that would create a more feminine/nose look how is the limit for tissue removed.
A: The only area of the nose will tissues can be externally excised is the nostrils or nasal base for nostril narrowing. But for the rest of the nose no such excisions can be performed without severe scarring.
Dr. Barry Eppley
World Renowned Plastic Surgeon