Your Questions
Your Questions
Q: Dr. Eppley, One side of my face (left side) is more developed and right side is a bit inward. So it has made asymmetry in my face. And it can be seen that, due to this my jaw are also uneven. How can this be improved?
A:You have classic right-sided facial hypoplasia of an inferior basis which means the lower drawl is the most severely affected and in the face it becomes much less so. Like all facial asymmetries one has to prioritize the most significant area for change and that is clearly your lower jaw. The most accurate and successful correction of moderate lower jaw asymmetry, provided the occlusion is acceptable, is a custom jawline implant made from the patient’s 3-D CT scan.
Dr. Barry Eppley
Q: Dr. Eppley, I have my surgical notes it says 10ml each was injected into the cheekbones eyebrow and under eye. Pre op my cheekbones were quite sharp and I had a sub malar oallow (not sure if that’s helpful for dr Eppley to evaluate where the fat could be) my tear trough was very prominent also. It feels like the fat is hanging and puffy at the front of apple of cheeks which hopefully you can see in these photos.
A:Thank you for sending all of your information. The cheek areas where it is located is virtually impossible, or at the least ill-advised, to attempt any form of extraction which can only be done by micro-liposuction. Besides not being particularly effective there is a significant risk of irregularities from trying to do so…an aesthetic tradeoff you may not see as a good one.
Dr. Barry Eppley
Q: Dr. Eppley, ı wanna learn about this iliac crest reduction.I got wide hips and ı wanna change that.
A:On the basis of your pictures it looks like you are referring to the whole of the iliac crest, both anterior and posterior portions. Iliac crest reductions are typically done on the widest anterior portion of the crest as the posterior portion is not usually visible and is harder to access (see attached image) I suspect in a thinner patient where the posterior portion may be more prominent/visible it could be reduced as well…but I have never yet done it.
Dr. Barry Eppley
Q: Dr. Eppley, What kind of exam is done to detect facial fillers and implants that I already have? Because I had a CT scan and it didn’t show up my hyaluronic acid fillers and not even my porous polyethylene jaw angle implant
Regarding hyaluronic acid fillers, is there a specific setting for them to show up on CT scans? Because I have them in my cheekbones, and they didn’t show up either.
A:HA fillers can never be seen on a CT or any other scan. Only Radiesse filler can be seen on scans.
Porous polyethylene implants can be seen on a 3D CT scan but it takes special software to extract the data to make them visible.
Dr. Barry Eppley
Q: Dr. Eppley, Hello, I’ve had a consultation with a surgeon in Beverly Hills about my chin implant revision who recommended I see Dr Eppley for a genioplasty instead.
I have had two chin implant surgeries over 10 years After the first surgery I woke up and the implant on the right side had slipped up quite high. You couldn’t see this but I had some numbness on that side for a while which eventually returned. Several years ago, I had a revision as I wanted to fix the implant not being straight and the revision actually made things much worse, as the left side now sticks out and you can see it.
My surgeon said I had some bone resorption & bone wasn’t straight under the implant so he tried to file down the left side so the implant would sit in line but couldn’t make it sit straight. The right side is now fine/in line, so aesthetically I like the right side of my face/side profile but not my left.
I have had 3 consultations since with different people about doing a implant revision & all have said I should do a sliding genioplasty instead, the last recommended you (Dr Eppley) so I’m hoping you can help!
A: When treating any facial implant malposition, chin implants included, there are several basic principles to create the greatest opportunity for success:
1) A preoperative 3D CT scan is needed to truly understand the actual implant position and how to best correct it. You can not rely on intraoperative ‘eyeballing’ alone as the incisional access does not provide full visual assessment of the implant and bone. As a result incomplete correction usually occurs and implant and bone manipulations are done that may never have really been needed.
2) Wherever the implant is positioned it needs screw fixation otherwise it is going to shift/move as soon as the incision is closed. Suture fixation never works in as established implant pocket for secure positioning.
Neither of these were done in your chin implant revision.
Converting to a sliding genioplasty in your situation is bit like trying to get rid of a mouse with a shotgun (imbalance between the solution and the problem). It may be appropriate if you didn’t like anything about the implant result or have simply decided you do not want an implant at all…which is not the impression I am getting. Sliding genioplasties have their own potential issues and you only make such a radical chin augmentation change when the problem justifies it.
Dr. Barry Eppley
Q: Dr. Eppley, My big boobs are saggy and feel deflated on top. What procedure is best for long term success for me?
A: When you have large breast with a significant amount of sag there is going to be no way to get around for the need for a full breast lift. This is the basic procedure to get the breast tissues back up further on the chest with a better nipple position. Whether you would ultimately require an implant or fat injections for persistent upper pole fullness is an issue to be determined when the breast lift has settled out into its final shape 3 to 6 months later . While no one can accurately predict in advance whether that secondary augmentation will be needed my suspicion is that it will more likely be needed than not.
The issue with breast lifting is always the same and that is the resultant inverted t-shaped scarf pattern. Ultimately the need for a breast lift requires one to assess which problem they would prefer to have, meaning do I want ta better breast shape and position of the breasts on my chest with scars or is it better to have no scars and the breast shape that I now have. Each patient will view that preference differently.
Dr. Barry Eppley
Q: Dr. Eppley, Hi, I am interested in chin reduction. I would like to decrease the vertical height of my chin only, without changing its projection or my jawline shape. Thanks!
A:Thank you for your inquiry and sending your picture. I can certainly see the basis of your inquiry. The first thing to determine in consideration of chin reduction is what is the cause of the excess. Is it an isolated bony excess, soft tissue chin pad excess or a combination of both. To make that assessment I need front and side view pictures smiling and non-smiling as well as an x-ray of the bone. I can see that you have sent a nonsmiling front view Picture but that alone is not enough to make a proper assessment. X-ray analysis could include a front and lateral cephalometric film or a 3-D CT scan of your face which is the most ideal.
Dr. Barry Eppley
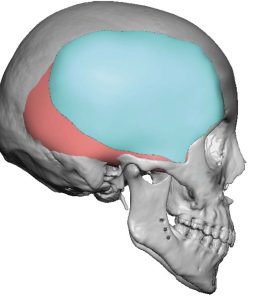
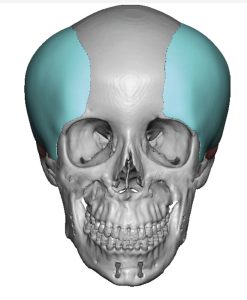
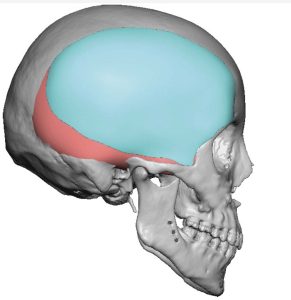
Q: Dr. Eppley, I am interested in the occipital augmentation procedure. I have put 2 pictures of my head shape along with a version of what i would lkek it to look like post surgery. i want PMMA bone cement procedure.
A:Thank you for your inquiry and sending your pictures. In evaluating your ideal surface area of skull augmentation I have provided some realistic limitations of what can be done as seen in the attached picture. Most people believe that the occipital bone goes down much further down into the neck than it actually does. Furthermore the use of PMMA one cement is a very limited skull augmentation method that could never accomplish this type of surface area coverage. That is an historic skull augmentation material which has been completely replaced by the far superior custom skull implant design approach based on the patient’s 3-D CT scan.
Dr. Barry Eppley
Q: Dr. Eppley, I would like to understand if I’m a suitable candidate for iliac crest reduction. I’m a tall male and have always had wide hips relative to my ribcage. The height and width of my hip bone cause a feminine curvature to my torso, where I’d like the shape from my waist to my legs to be a smooth line as is typical for males. Please view the attached pictures for the front and back view. I would appreciate it if you could provide me a quote for the approximate cost of this procedure and an estimate of how common the long-term complications are, understanding that this appears to be a quite rare operation.
A: Thank you for your inquiry and sending your pictures. I can certainly appreciate your issue with a wider/more flared pelvic wing. I think you are a good candidate for iliac crest reduction and I have attached an image as to what I think can be accomplished. It is always a question of how much of the iliac crest can be reduced but at the minimum but it is usually 1 to 1/2 half cm per side which should be enough to create the image prediction. Today I have seen no short or long-term complications from the iliac crest reduction procedure other then there is some short term in the first few weeks of walking discomfort but that quickly recovers.
Dr. Barry Eppley
Q: Dr. Eppley, I am writing to seek a professional consultation regarding skull reduction and reshaping surgery. My primary concern is that the size of my head feels disproportionately large and out of balance with my overall body frame
My specific goals and inquiries are as follows:
1. Body Proportionality: I feel that my current head size is abnormal relative to my physical stature. My goal is to achieve a more harmonious and balanced appearance. I would like to understand how much reduction is realistically and safely achievable to make my head look more proportional.
2. Request for Case Studies: To help me visualize the potential transformation, could you please share or direct me to before-and-after photos of patients who had similar concerns regarding overall large skull size and achieved successful results?
3. Surgical Approach: Based on your extensive experience, what is your approach to overall volume reduction, and what are the typical success rates for achieving a natural-looking contour?
I am looking for a permanent solution and trust your expertise in this specialized field. I look forward to your guidance on the next steps.
Best regards,
Are there other cases similar to mine, and what is the success rate of the operation? I would appreciate a response. Thank you.
A: In answer to your questions:
Due to patient confidentiality we can not pass out patient pictures. Whatever has been allowed to be shown can be seen on my various websites, particularly Explore. You have classic brachcephaly of which the typical treatment is a combined custom back of the head skull implant with biparieto-temporal bone reduction. The attached recent case link will explain all you need to know about that type of skull reshaping surgery and what is achievable in perhaps what is a more severe case than yours.
https://exploreplasticsurgery.com/adult-brachycephaly-skull-reshaping-case-study/
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My goal is to slim my jawline to have a more v-line and less wide jaw. I have had masseter botox for the past 6 years. The jowls are secondary to that due to significant masseter hypertrophy. I also have a small amount of chin filler and malocclusion from an overbite.
A:Thank you for sending your pictures. I am a bit concerned about how effective jaw reduction would be for you given your very soft thick tissues and the size of your masseter muscles. The question is not whether you can have jaw reduction but would it achieve the lower facial shape that you desire. There is also the issue that when you do jaw reduction surgery it is very common to develop soft tissue laxity in patients with thicker tissues. This is why you see young people get lower facelifts after jaw reduction surgery because of this not infrequent postoperative sequelae. You have already seeing what happens with some masseter muscle reduction by the development of jowls just from that soft tissue change.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am looking to get a LeFort 1 Osteotomy surgery plus cheek implants. I am looking to do these surgeries at the same time and I am wondering how much it would be plus how long the recovery time would be.
A:It is not uncommon to perform cheek augmentation at the same time as a LeFort I osteotomy. However before any cost or other imformation can be provided I would need some more specific information about the desire/need of a LeFort I osteotomy.
1) Is this a Lefort I osteotomy in isolation=
2) if so do you have a malocclusion where ot could be performed in isolation
3) Have you had a orthodontic preparation for the surgery?
4) How much movement does the Lefort I osteotomy require?
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Looking into getting implants for my left arm. I had shoulder surgery previously, After the surgery I lost function of my bicep and tricep and now my arm has lost a lot of muscle. Would really like to get my arm looking as close to normal as can be.
A:Thank you for your inquiry and sending your excellent comparative arm pictures. Fortunately the upper arm muscle loss is moderate in size and the combination of a bicep and tricep implants should do well at making the left upper arm closer to that of the right arm The tricep implant is always placed in the subfascial location on top of the muscle. The bicep implant could be placed either under the fascia on top of the muscle or intramuscular on top of the bone. Because your muscle loss is spread through out the length of the bicep muscle I think a subfascial implant placement would be better then on top of the bone which creates more of bump projection rather than an overall increase in the size of the entire muscle.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Wishing to perform the Clavicle Reduction surgery and the Scapular reduction. All intended to achieve a little more feminization on my body. I’d like to enquire costs and if it’s worth going only with the clavicle reduction or both.
A:Thank you for your inquiry and sending your front view shoulder picture. As a general rule shoulder reduction has a far more significant aesthetic impact than that of scapular reduction. Scapular reduction should be thought of as a complement to shoulder reduction not a comparative aesthetic procedure. While clavicle reduction can be done with incisions that can heal almost imperceptibly the same cannot be said for scapular reduction as the scars on the back maybe much more noticeable. Thus whether scapular reduction is aesthetically useful depends on what area of the scapular bone one sees as prominent as well as how long is the incision needed to reduce it. This will require a back view picture which highlights your scapular prominence concerns.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am an MTF transgender woman seeking gender-affirming surgery.
I am interested in the iliac crest implant procedure (Pelvic Plasty) for hip widening that you have developed. Based on my research, I understand this is a highly specialized and relatively new procedure that you have pioneered, with only a handful of cases performed.
I am requesting a consultation to discuss am I a good candidate for this procedure? I am seeking maximum hip width for feminine hourglass silhouette. I understand this procedure provides upper hip width only (does not address lower hip fullness)
-A:Thank you for your inquiry and detailing your aesthetic objectives to which I can say the following:
1) Pelvic Plasty is not a new or experimental surgery. It was developed in South Korea and they have performed it for years. I have merely brought that type of hip surgery to the United States at their request and my own interest.
2) Whether you are a good candidate for the procedure would require a picture analysis of your hips from the front and back view.
3) Pelvic Plasty can be performed by the placement of titanium iliac crest implants alone or in combination with an attached silicone hip implant. By far the latter is the most common approach based on the potential accentuation or creation of a hip dip deformity (subiliac hollow) below the iliac crest once it is widened. Whether that would be a concern for you is determined preoperatively buy taking your pictures and doing imaging to determine how it may look based on the plates alone or in combination with hip implants. Based on your description of hip augmentation objectives, Seeking maximum hip width for feminine hourglass silhouette, it would seem that the combination of crest plates and hip implants may be aestheically needed until proven otherwise (picture imaging).
4) The details of the surgery and results are well illustrated on one of my websites, www.exploreplasticsurgery.com, by searching under Pelvic Plasty.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Thank you for he detailed information on rib modification available on your website — it has been helpful in understanding the evolution of the procedure.
Before proceeding with imaging and formal planning, I would appreciate clarification on a few points so I can compare options responsibly:
• Approximately how many aesthetic rib contouring procedures (subcostal rib reduction) have you performed to date, and for how many years have you been performing them?
• Do you have additional before-and-after examples of subcostal rib reduction cases you are able to share?
Since my case would likely involve simultaneous breast implant exchange, I would also appreciate clarification on:
• How many combined rib contour + implant exchange procedures you have performed
• Whether you personally manage the breast revision component or collaborate with a breast specialist
• Any before-and-after examples of combined cases, if available
For surgery to feel worthwhile to me, I would be seeking a substantial and clearly visible reduction in projection. Ideally, I would hope for complete flattening of the area; at minimum, I would consider approximately a 50% reduction necessary for the trade-offs of surgery to make sense.
I understand that each case is unique and that a 3D CT scan would be necessary for final planning. I simply want to ensure my expectations align with what is safely achievable before moving forward.
Thank you again for your time and guidance.
A:In answer to your questions I can make the following comments:
1) I have an enormous ribcage modification surgical experience beginning over 15 years ago, most of which has been excisional in technique. Only more recently has the less invasive techniques become more popular although I am very reserved about them given the more limited results that I have seen from them.
2) With this vast experience in hundreds of patients the one thing I know for certain is that surgical results from ribcage modification are highly variable. Some patients get very modest results while others are more dramatic. And these are not all completely predictable. Thus the best patients for these procedures are those who see it as a structural operation in which this is all that can be done and they are willing to accept whatever result can be achieved, unpredictable as it may be. While I can certainly appreciate and respect the patient who is seeking a numerical or percentage result these types of patients make me apprehensive for taking them on due to the unpredictable success of the surgery despite how well the operation may be performed.
3) It is not rare for a combination of breast augmentation/implant exchange and ribcage modification procedures to be done during the same surgery. I often view that as beneficial due the diametric nature of the two surgeries. The one procedure helps make the other one look even better than if it was just done alone.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley,I am seeking a surgical evaluation regarding the feasibility of a Modified Subcranial Orbital Box Osteotomy specifically for the purposes of altering interpupillary distance (IPD) and vertical orbital positioning. My goal is a physical reduction of the IPD by 1mm to 2mm (bringing the pupils closer together) and a simultaneous vertical shift of the pupils by 0.5mm to 1mm. Given that I am strictly interested in a subcranial approach that avoids a frontal craniotomy and a coronal scalp incision, can a Modified Medial Orbital Wall Osteotomy be effectively utilized for narrowing the interorbital space rather than widening it? Specifically, how is the internal nasal and ethmoid anatomy managed to allow for a 1-2mm inward bone shift, and what are the primary risks to the nasolacrimal (tear) ducts and the origin points of the extraocular muscles at this specific magnitude of movement? Furthermore, is a vertical pupillary adjustment of 0.5-1mm surgically stable when performed alongside a medial shift, and does this combination of multi-vector bone movement significantly increase the risk of permanent diplopia (double vision) during the 6-12 month healing and settling phase?
A: For the very modest changes that you are seeking an orbital box osteotomy, by comparison, is an operation of magnitude that seems out of proportion to the goals. Particularly when you consider the potential risk as you have described. I might also add that I wish surgery was as precise as a millimeter or two of controlled movements, particularly vertically, but the reality is it is not as precise as the movements you desire.
The point being is it is always important to match the operation to the size of the problem. Doing a big operation for a small defined change is disproportionate and the risk:benefit ratio is altered accordingly.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have a unique problem with a dent from a steroid injection in my glabella area. It was done to bring down swelling after a seroma from a rhinoplasty in September. I am extremely embarrassed by it and want it fixed desperately. I can not do filler because I had a terrible reaction to filler. The rhinoplasty was done to remove granulomas from Restylane filler! I’m told this is a dangerous area for filler and fat transfer due to vascular occlusion risk. I saw a case you did with dermal grafting in the glabella area and wondered if that may be an option for me. I will include a photo
A:That is an impressive glabellar indentation from a steroid injection. You are correct in that injections iin this low central forehead area do have a potential history of adverse events. Thus the use of a dermal-fat that graft placed through an endoscopic approach seems to be the most prudent treatment option.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I had shoulder implants does that keep me from this surgery?
A:Your existing deltoid implants do not preclude you from having clavicle lengthening is that surgery is done on the clavicle bone well away from the implants.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I want know if I can get the largest custom testicle implant size possible.
A: Testicle implants size is not the issue as with custom designs any size can be made. I’ve seen patients receive is large as 11 cm implants. The rate limiting issue is the scrotum and how much implant volume can it safely accommodate. There are numerous factors that go into the ability of the scrotum to stretch including patient age, history of any implants or other materials out of been placed into the scrotum, as well as what one’s perception is of the largest implant size possible.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, One year ago I got a genioplasty done. One side of my chin appears to be longer than the other which gives the appearance of my chin pointing towards the left. I prefer the length of my chin on the right which appears shorter and when I feel the left side it feels like soft tissue as opposed to a bone issue. I’ve not heard of only muscle work on the chin but is it possible? What can be done to correct the balance of my lower face?
A:If you had had a advancement sliding genioplasty and the chin is now asymmetric you assume, until proven otherwise, that this is a cant to the bone advancement and it is a bony issue no matter how it feels. To determine the anatomic basis of this post sliding genioplasty chin asymmetry you need a 3-D CT scan which will clearly show you the position of the advanced chin segment. It is not rare at all that a tilt in the bone position has occurred with the advancement.
Also you have correctly surmised that the concept of ‘chin muscle work’ to correct asymmetry is unheard of. And that probably is so because of the obvious reason but it does not exist in my experience.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley,I would like a virtual consultations with 3d imaging of what will be medically possible to make me look prettier. Im looking to do rhinoplasty as well . Im not sure if you do that as well but can you show me a picture of what outcome I can get if I were to have an implant or some type of work done to make my face more balanced.
A:Thank you for your inquiry. You have a common misconception about what imaging is designed to achieve. Photo imaging and manipulations thereof is not done to show patients what their surgical outcome will be… no one can predict or guarantee that with absolute accuracy. Rather it is done to determine what the patient’s objectives are by trying to seeing what changes they see as aesthetically beneficial. Then that imaging serves as the target for which surgical procedures are designed to try and achieve or come reasonably close to it within the restrcctions of what tissue healing and their anatomy will allow. In other words 3D picture imaging is about goal setting not about outcomes.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I’d like to inquire about a skull reshaping procedure. I’m looking to address my peaked frontal skull shape along with a mid-line ridge and some other dents along the top and towards the back of my skull in one procedure There seems to be minor-moderate parasagittal deficiencies towards the front of my skull/forehead (not extending all the way to the back) causing the appearance of a peak at the front that is more prominent in certain lighting and from certain angles of view. I have a mid-line ridge also, along with several other minor ‘dents’ along the top and towards the back of my skull including a slightly depressed area at back. I have attached quite a few images to try give a complete idea of the shape of my skull as it is quite hard to capture it in just a few. I guess the deficiencies are not major, but they are apparent in real life situations due to lighting, angles etc. I would estimate that the parasagittal areas would need to be augmented 8-12 mm at highest points. I’m hoping to have the entire top of my skull contoured to a normal, aesthetically pleasing look. A few questions: 1) What approach would you recommend in order to achieve my goal? If custom implant is used, are minor bumps able to be address along with main deficiencies? 2) Would I need scans of my skull for this etc? 3) How soon could the implant be created and the procedure done once I am ready to commit to the process? Thank you so much for your time
A:Thank you for your inquiry and sending your pictures. In the treatment of the peaked head shaved there are two fundamental approaches which are diametric in nature. For the most minor and least invasive approach some patients may opt for reduction of the peak in the center of the skull which produces a very modest improvement. The other option would be augmentation of the parasagittal and upper temporal areas for a more overall rounded and profound change which requires a custom skull implant to do so. Based on your aesthetic Head reshaping objectives it appears at the latter maybe the preferred approach. In that regard I have attached some imaging of what that potential concept may be able to do.
You have correctly surmised that the fabrication of a custom skull implant requires a 3-D CT skull scan and it generally takes up to eight weeks to have the implant designed and ready for surgery.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, i would like to know about temporal implant and skull implants. My goal is a large forehead / skull and heart face shape.
A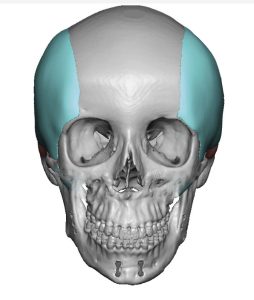
 :What you are seeking is what I call the classic female head widening concept which involves custom fronto-temporal implants as per the attached illustrated implant designs. They come close to the side of the fore head and may to a small degree blend over onto it. Technically what the patients are usually trying to accomplish is to widen the four head but what they really mean is widening the temporal area next to it and have the temporal augmentation blends slightly into the side of the forehead.
:What you are seeking is what I call the classic female head widening concept which involves custom fronto-temporal implants as per the attached illustrated implant designs. They come close to the side of the fore head and may to a small degree blend over onto it. Technically what the patients are usually trying to accomplish is to widen the four head but what they really mean is widening the temporal area next to it and have the temporal augmentation blends slightly into the side of the forehead.
 But if the objective is frontotemporal widening combined with head widening, as suggested in the back view of your pictures that you provided, then the implant concept is expanded to cover a broader surface area also widen the side of the head as well. (see attached design)
But if the objective is frontotemporal widening combined with head widening, as suggested in the back view of your pictures that you provided, then the implant concept is expanded to cover a broader surface area also widen the side of the head as well. (see attached design)
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in infraorbital and submalar facial implants.
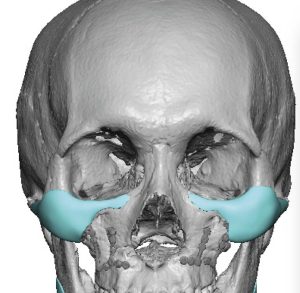 A: Thank you for your inquiry and sending your pictures. While you have an infraorbital rim deficiency it is really part of an overall midface deficiency of a few millimeters throughout the entire bone surface area. The question then becomes does one merely address the infraorbital rim-malar area in isolation (custom female IOM implants)
A: Thank you for your inquiry and sending your pictures. While you have an infraorbital rim deficiency it is really part of an overall midface deficiency of a few millimeters throughout the entire bone surface area. The question then becomes does one merely address the infraorbital rim-malar area in isolation (custom female IOM implants)
 …or approach it from a more global midface perspective (extended IOM implant design to augment the lower paranasal area as well)
…or approach it from a more global midface perspective (extended IOM implant design to augment the lower paranasal area as well)
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am planning to have temporal reduction surgery sometime in the future, but I have a question: will the result be long-lasting? Will I need a second surgery in the long term? Is it possible to avoid the need for a second surgery? I read on your website that: “however, due to the limitations of the incision, the surgery does not extend much into the anterior and thicker portion of the muscle covering the fossa concava. Although most patients do not require treatment in this area, a small degree of residual fullness may persist. In my experience, this is the main reason why a second procedure may be requested”. I would prefer not to have a second surgery; would a single surgery be sufficient?
A:In answer to your temporal reduction surgery questions:
1) The vast majority of temporal reduction patients only need one surgery and it is rare that ever need a second stage.
2) The reason being is that whether management of the anterior muscle portion needs to be done is determined initially and is then incorporated into the primary procedure as an anterior muscle transposition and posterior muscle removal.
3) In rare cases the patient may only initially feel that they need only the posterior segment treated and then they may choose to have the anterior muscle reduced secondarily. But again, this is rare because these are issues we discuss initially and it was usually pretty obvious from the beginning whether both muscle segment need to be treated.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I’ve been to so many doctors I’ve lost count as to how to fix my undereye hollows. Had them since I was young I’d do anything to get rid of themDo you work with 3D-milled PEEK or custom Medpor implants? Given how clearly I can feel my orbital rim, I’m concerned about the transition being seamless. How do you ensure the edges won’t be palpable?
A: Custom infraorbital-malar-maxillary implants are the only method to properly treat a negative orbital vector. Whether the material uses is solid silicone or PEEK as a matter of further discussion each of which has distinct advantages and disadvantages. As a general rule PEEK implants often are too small even when custom made to properly treat the negative orbital vector. This is why I prefer solid silicone in this area where more sufficient designs can be used. I would never use Medpor material in the periorbital area because it does not have fine edges and is a real problem for both placement as well as subsequent removal or revision if ever needed.
Your case of negative orbital vector poses a special problem because you have a distinct lid – cheek groove (see attached picture) which would not be completely eliminated as the effects of the augmentation are largely above it. This would need to be treated with fat injections as a combination with the implant to try to reduce that line as much as possible.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley,Wondering if the lump on my forehead is a pseudolipoma from trauma and if Kybella would work to help flatten it, or, if another procedure would be more appropriate.
A:I am not sure what a pseudo-lipoma is. But it is more likely, because it has occurred from trauma, of being an osteoma. But whatever the pathology is it is highly unlikely Kybella injections would be effective for its reduction. It is going to require surgical removal.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, would it be possible to deproject the radix slightly, to give the illusion of a brow ridge (assuming my radix is already really outgrown) (it looks kind of like those blue avatar people from the side profile). I attached a morph of my nose (the first is unedited, with just me pulling back the soft tissue to show the bone more clearly, and the second is how i would want it to look). Do think a result like this is achievable without making my nose slope straight down from my forehead (The main issue isn’t that it’s too big, even though it is too big, the issue isn’t that is molds into my forehead and makes it look super flat). Any advice or help would be greatly appreciated, thank you.
A:While I see no attachment that shows your morphed nasal changes I can tell you that reduction of the high nasal radix is one of the hardest things to do in all of rhinoplasty surgery because it is a bone structure located in the no man zone between the nose and the forehead where there is limited surgical access. I have done numerous high radix reductions through a dual osteotome technique from an intranasal and a percutaneous approach. Whether your ideal morphed changes are achievable would require an actual assessment of that image.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am interested in improving the appearance of the area above my lips and softening my lip lines. I am also interested in lip surgery or augmentation for my upper lip which is basically non existent now at the age of 51. Improved volume and symmetry in both the upper and lower lip is desired. I have been looking for a surgeon that has a specialization in this area. I was excited to see so many examples in the photo gallery. Looking forward to seeing what the possibilities are. I had two prior consultations wbut in the end did not feel they were the right doctors for me.
A: Thank you for your inquiry and sending your pictured. You have four aesthetic lip issues: 1) a very long upper lip with a lot of skin between the nose and the upper lip vermilion, 2) small vermilion height (pencil lip), 3) vertical lip lines (wrinkles) and 4) a larger but still small lower lip vermilion/size with central vertical lip lines
Because of the amount of nasal base/sill show I don’t recommend a subnasal lip lift. The upper lip vermilion advancement is better because it changes the entire vermilion from one side to the other and will also diretcly remove those lip lines in the zone of excision. Because of the central lower lip lines and to keep the lip size proportionate a 2mm lower lip advancement would be helpful as well. (see attached diagram)
While I believe pip advancements would be the only effective surgical lip augmentation method it does create fine line lip scars so one needs to be cognizant of that tradeoff.
Vertical lip lines are a very difficult problem to improve long term due to their dynamic cause (lip movements) and occur almost exclusively in Caucasian females due to their thinner skin. The only treatment is laser resurfacing but I don’t recommend that at the same time as the lip advancements as it may make negatively affect the vermilion-cutaneous scar lines.
Dr. Barry Eppley
Plastic Surgeon