Your Questions
Your Questions
Q: Dr. Eppley, I had a chin implant in 1995. Twenty-five years later, I began to have very specific localized pain in the jaw bone directly at edge of implant, and also feel overall tightness and discomfort throughout my chin. There was back and forth that the pain was dental; ultimately had two teeth extracted and still have the pain. CT scan shows the implant is secured with 4 metal screws. I want to have the implant and screws removed and am worried about the risks of this, bone remodeling, etc, after so many years. (The original surgeon has long retired so I don’t know what the implant or screw is made of). I have attached a cone beam xray.
A:While there is nothing ominous in the 3D CT scan and the implant looks normal (well below the tooth roots, has no signs of significant settling into bone and even has reparative bone overgrowth over the top of the implant) I would agree with you that by the process of elimination the implant should be removed. By the way the implant appears to have been hand carved and appears on the 3D scan it is either silicone or Goretex. (most likely the former) But regardless of its material composition it can be removed along with the screws. If there is any bony irregularities I would just fill them in with allogeneic bone chips/paste.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a transgender person. I have been following your work for some time and have the intention to get shoulder reduction and rib removal done.
I have been bothered by the masculine and broad shape of my upper body for years and have never been able to make dues with it. As a result, I have considered your surgeries for a few years now and am finally in a financial situation where I feel comfortable requesting a consult or for more information.
I have attached some images of the related regions – my shoulders from a front view, and my lower torso/waistline from a rear view. I included pictures of this nature, following the way sample pictures on your site have been taken.
What would you recommend regarding waist narrowing procedures? As a transgender individual, I figured the type 2 would be suggested but I would like to hear your opinion on it. My interest is in reducing the general width of the rib cage but also improving the waistline as much as I can.
In addition, what seems to be the maximum amount that could be reduced in the shoulder regions? I would like to reduce the broadness and ‘masculine’ appearance of the shoulder region. I am not as much bothered by the high shoulder-waist-ratio that I have as I am by the simple fact that my shoulders are just quite broad compared to the average to begin with.
Finally, I was wondering if it would be possible to schedule this for early May 2025 and wanted to discuss financing plans following more information. In addition, would assuming a month for recovery for both procedures (if they can be done at the same time) be a fair assumption?
Thank you very much for your time and I hope you are having a pleasant day!
A:Thank you for your inquiry and sending your pictures to which I can provide the following answers:
1) For maximal waistline reductive effect you are correct in that the Type 2 Rib Removal procedure is best. There is no procedure for overall ribcage narrowing but at least the Type 2 is the most aggressive approach for addressing the lower ribcage.
2) To get an idea of the potential effects of shoulder reduction and rib removal skeletal procedures I have attached the following images.
3) It is not uncommon to have both shoulder reduction and rib removal surgery done at the same time. The key to doing so is to have adequate postoperative care arranged in the immediate after surgery time period.
4) It would be fair to say that at least one month recovery is needed but this answer is dependent on what one is recovery to…..which will vary based on the activity. (more or less time)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have questions about chin augmentation. Specifically, I’m interested in achieving 10mm of horizontal projection with a chin implant.
I understand that custom implants can also provide vertical length adjustments. While adding vertical length isn’t a priority, if I opt for a custom implant, I would like to add 4mm of vertical height. Could you let me know whether you offer both regular and custom chin implants or primarily focus on custom options? Additionally, I’d appreciate it if you could outline the price difference between the two, as I’d prefer a regular implant if it offers comparable results at a lower cost.
I also wanted to ask about the possibility of combining the chin implant procedure with other surgeries I plan to have with you. My current surgical plan includes a top head skull reduction, temporal reduction surgery with temporal muscle removal, occipital reduction, forehead bone reduction, and a hairline lowering surgery with a 25mm lowering of the hairline.
When I contacted your clinic, I was told that all these procedures could be done together. I am aiming to schedule everything for winter or spring 2025. Would it be feasible to include the chin implant surgery at the same time as these other procedures? I live out of state, and I would be saving a lot of money on airfare if all the surgeries were done together.
Thank you for your time and guidance.
A:i remember you well from an inquiry and imaging done in September 2022. In answers to your questions:
1) If the goal is 10mm of horizontal projection and vertical lengthening is not a priority (remember that even pure horizontal chin augmentation will add the perception of some increased vertical length then a standard chin implant should suffice.
2) A chin implant can be added to all of the mentioned skull reshaping procedures.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Hello! I am primarily interested in modestly increasing the anterior projection of my chin, avoiding facial lengthening and jaw widening. I would like to explore which options are most suitable for my face, learn more Dr. Eppley’s custom implant process and pricing for each option that I would be a good candidate for.
I am also interested in assessing my candidacy for subnasal philtrum shortening, as well as associated procedural details and pricing.
A:To achieve the dimensional chin augmentation changes of increased horizontal projection and no width or length increases can be done by two approaches both based on the need to bring the augmentation upward as it comes forward. If you don’t make that compensation in the movement the chin will get longer. This can be done by either a bony sliding genioplasty or a custom chin implant. When it comes to an implant augmentation it requires a unique design for which no standard implant can achieve. (see attached imaging
For the upper lip you can’t really have a subnasal lip lift alone as the sides of your upper lip have the vermilion disappearing as it goes to the sides. (greater on the right than the left) You would have to combine that with lateral vermilion advancements to avoid an A frame upper lip deformity. (see attached showing the subnasal lip lift without and with lateral vermilion advancements)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, my forehead is slopped on one side and wavy on the other. I was wondering how much it would cost to get that fix? It has been something that I have long felt insecure about.
A:With the combination of an excessively sloped forehead on one side and irregularities on the other side this sounds like a custom forehead implant would be the most effective approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
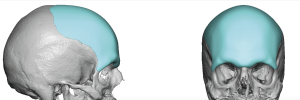
Q: Dr. Eppley, I’m 32 year old female. Through out my life, I’ve never liked the shape of the back of my head but couldn’t do anything about it because i was too young, didn’t have the money or couldn’t afford insurance. Now that I’m older, i have been researching head augmentation through implants . Ever since i was a baby, I’ve been layed on my back and over the years it flatten the back of my head. So i have always had an Afro hair style to cover the shake of my head. But now I’m losing hair slowly and i really want to see if there is anything you can do to change the shape of my head to look normal. One of the implant I’ve looked up is call methyl methacrylate. or if there is any other bone substitution you may recommend. I’ve attached some pictures for you to look at. Please give me a little more information about the procedure with the cost of it and what type of insurance I need.
A: For flat back of the head augmentations a custom skull implant is the best approach for maximum projection, smoothness and the smallest scalp scar to place it. (see attached image) I have abandoned the use of PMMA acrylic bone cements years ago because of their limited effects and other issues. Such aesthetic skull augmentations are never covered by insurance since they do not cause any functional problems.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What are the pros and cons of thigh, buttock and hip implants compared to fat grafting? Should they be considered as standard for body feminization as breast implants are for breast augmentation? Or are they riskier?
A:This is a complex question which defies a simple answer. But it speaks to the fundamental differences between implant vs autologous aesthetic augmentations. The ‘simple’ answer is if the area in question can get similar results with both methods then one should undergo fat grafting first as it is ha a lower risk of complications than an implant…and one can always graduate to an implant of the desired result is not obtained with fat grafting.
The complex nature of the question lies in that most aesthetic areas for augmentation can not get similar result with both treatment methods. So each aesthetic area in consideration must be evaluated in that context on an individual basis.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello i would like to ask you if It is possible to solve my condition. I have a problem on my eye area appearance and i think it’s because of my narrow brow bone width and wide byzigomatic distance. I think the eye separation ratio isn’t ideal, i mean the ratio between IPD and byzigomatic distance is too wide and make my eyes look too much at the centre of the face. And i think It s because my brow bone width is too short in relation with my other features.
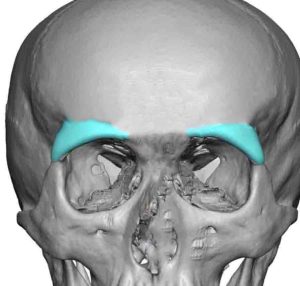 A:I believe your supposition is correct in that the lack of brow bone width makes your eyes look too close together. The attached imaging proves that theory. This could be achieved with tail of the brow bone augmentation with custom implant designs placed through upper eyelid incisions. (see attached implant designs)
A:I believe your supposition is correct in that the lack of brow bone width makes your eyes look too close together. The attached imaging proves that theory. This could be achieved with tail of the brow bone augmentation with custom implant designs placed through upper eyelid incisions. (see attached implant designs)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For the shoulder reduction would the amount removed per side (2-2.5cm) scale as well with height and if so – how much would potentially be removed for a height of 174cm?
A:I always try and remove the maximum amount of bone length based on the length of the clavicle but there are limitations based on the ft of the fixation plates. But it is fair to say that in tall patients they may get 2.75cms…very rarely 3cms removal per side can be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello. I was wondering if there was a way to minimize or fix my brachycephaly. Thank you
A: Augmentation of the flat back of the head is done by the placement of custom skull implants. What degree of correction/augmentation you desire would determine whether it is a one stage or a two stage process.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was looking into your forehead surgeries and I was wondering what you’d have in order to get a more forward projected forehead/brow ridge? I’d like to bring the entire thing forward so much so that it shadows over my eyes, but look natural in the way that it isn’t just a protrusion in my forehead.
 A:The most effective approach is a custom forehead-brow bone implant which I do often for these exact upper facial male needs.
A:The most effective approach is a custom forehead-brow bone implant which I do often for these exact upper facial male needs.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a complex regarding my chin area, as I think it lacks projection and makes my already thick lips look more protruding. I think a sliding genioplasty would help with my facial profile, but I would like to have your expert opinion on whether this surgery would help. I am also concerned about the presence of titanium screws, as I have read this can offset certain sensitive airport security machines. Would there be a non-titanium fixation option as well, and if so, are there downsides to this as opposed to the traditional titanium fixation? I have attached photos.
Thank you!
A:I do think that chin augmentation would be beneficial for your profile. But in females one must be careful to not try and make the augmentation too excessive which can also make the nasolabial fold much deeper. (se attached imaging) Any form of titanium plate/screw fixation has NO adverse effects on airport scanners or in getting medical MRIs. This appears to be a persistent misconception which is a regular question from many patients.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am reaching out to inquiry about the Correction of Eye/Orbital Asymmetry, as you will see from the attached photos I have some degree of Vertical Orbital Dystopia on my Left Eye due to my low cheekbone on left side. My question is will a customized orbital floor that also correct left cheek bone. My wish result will be to minimize asymmetry of my upper mid face.I’m looking forward to your response!
A:Your type of orbital facial asymmetry appears more horizontal than vertical although it could be a mixture. The best way to make the proper diagnosis as well as determine what can be done is a 3D face CT scan. That will accurately show the true bony differences between the two sides as is the only way to tell how to treat the bony orbito-malar asymmetry. You never make judgments based on an external assessment only.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a lump on my forehead, I want to come in to get it checked and possibly remove it.
A:Saying you have a lump on your forehead is a bit of an understatement. That is definitely a very large lump. A CT scan is needed to determine if this is a benign outer cortical bone growth (osteoma…which can be shaved down) or whether this is an osteoid osteoma (full thickness of the frontal bone involvement( which requires a craniotomy to remove.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 25 year old male interested in the macrotia/ear reduction surgery. My primary issue is that my ears stick out quite a bit, particularly due to a relatively wide concha.
A:While I can see the desire for ear size reduction you have to be careful in your case because of your elongated conchal bowl. Reducing the ear around the bowl, which is how most macrotia reduction surgeries are done, can make the ear look ‘odd’. To determine how you would interpret that change I have attached some imaging of the potential change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to inquire about a consultation regarding potential facial reconstructive surgery. I have several concerns about my facial structure that I would like to address, and I am hoping to explore options for surgical correction.Specifically, my primary concerns include:
Forehead: I have a pronounced or prominent forehead, which I believe may be related to frontal bossing. I am interested in discussing potential procedures to reduce the prominence of the forehead and achieve a more balanced facial profile.
Brow Ridge: I have minimal to no definition of the supraorbital ridges (brow ridges) above my eyes, which gives my face a flatter appearance in the upper facial area. I would like to discuss whether brow augmentation or other procedures could help enhance this region and create a more defined appearance.
Eyes: My eyes have a prominent, rounded appearance, sometimes referred to as “puppy dog eyes.” I believe this might be due to proptosis or larger eye openings (palpebral fissures). I would like to understand if there are options to make my eyes appear less prominent and more in harmony with the rest of my facial features.
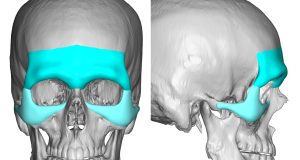 A: Thank you for your inquiry and sending your pictures. What you actually have is pseudo frontal bossing…meaning it looks like frontal bossing but only appears that way because the bones around the eye (periorbital) area are deficient. This can be seen when the periorbital bones are augmented that the frontal bossing goes away. (see attached imaging) The concept of combining a custom brow bone implant with a custom infra/lateral orbital-malar implant is the only way to achieve this effect (see attached image designs) and optimally addresses your listed forehead, brow ridge and eye area concerns/objectives.
A: Thank you for your inquiry and sending your pictures. What you actually have is pseudo frontal bossing…meaning it looks like frontal bossing but only appears that way because the bones around the eye (periorbital) area are deficient. This can be seen when the periorbital bones are augmented that the frontal bossing goes away. (see attached imaging) The concept of combining a custom brow bone implant with a custom infra/lateral orbital-malar implant is the only way to achieve this effect (see attached image designs) and optimally addresses your listed forehead, brow ridge and eye area concerns/objectives.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I am very interested in a skull reduction to improve my confidence and treatment of stress caused by body dysmorphic disorder. I’m a 26yo male who was had anxiety about my head shape my whole life. My main concern is the top of my head being too tall, and a slight outward shape above my ears and around the back. No hairstyles look suitable on me, and I think any improvement could be huge for my health. I can’t slick my hair back, my forehead is very square and feels almost too vertical instead of protruding in a natural shape. I had a horrible hair transplant done which I need to get corrected first. I was hoping reducing my forehead would the the solution, but the issue is more the shape of my head combined with a high and wide hairline.
My main questions are what the scars and usually like, and how hard it is to hide them under hair? I did see one photo on your website but the patients hair looks a lot different and messy in the after photo, which I as wondering is a result of hiding the scars. If you have any more patient before and afters I’d love to see them. I have good hair genetics with my parents having most of their hair still, and use minoxodil daily to help keep it thick. I would be willing to try finasteride at a low dosed and hopefully have no bad side effects, as a hair loss prevention.
A: By your description of the desired skull reduction locations the incision would have to be across the top of the head between the bony temporal lines or may just a bit below them. This would provide access for removal of the outer cortical layer of the top 0f the head as well as onto the sides and even into the upper forehead. These incisions usually heal quite well with minimal scarring particularly in skull reduction surgery where there is no tension on the healing closure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am reaching out to see if you could help me with my lip incompetence. I have had lip incompetence since I was a teenager, I am now 22. I had Double Jaw Surgery + Genio in April of this year. However, immediately after surgery I noticed that my lower lip was very tight and had limited mobility. Fast forward to today and my surgeon says that it isn’t chin ptosis but I have a lot of lower tooth show and my bottom lip cannot reach the top no matter how hard I try, so I am lost and would like your help if possible.
A: As you can see in your animated picture there is evidence of scar contracture of the soft tissue chin pad which is not rare as the soft tissues heal and settle down into the bony stepoff of the genioplasty. (which I assume was not grafted) Like all scar contractures a release and interpositional fat graft is the definitive solution for the tightness issue which did not exist before the surgery. What that may due for the lip incompetence is a different matter and less assured. By your own description your lip incompetence is long standing and existed before your jaw surgery. Thus it is essentially a congenital deformity not an iatrogenic one like the tightness which is more readily improved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My grandson has a webbed neck condition but no syndrome attached to it. What is your professional opinion of the procedure Posterior Cervical Lift and would you perform it? Thank you very much!
A: Like many aesthetic procedures the surgical treatment of the webbed neck has a variety of techniques to improve it, each with their advantages and disadvantages. There is no perfect webbed neck surgery method.
The posterior cervical lift is a variation of a direct webbed neck approach through a flap transposition rather than tissue rearrangements (z-plasties) along the outer web line. It is definitely an improvement over the historic webbed neck method which is effective and also fixes the laterally displaced M-shaped occipital hairline. It does of course create long linear scars that at least are out of the direct line of sight in the frontal view and a bit in the oblique view as well. Are they great scars….no…and they go well below the neck web into the trapezius area in order to work out the dog ears.
In comparison to any indirect webbed neck correction method it produces a more effective result but with more significant scarring. It really comes down to how the patient views the scars and how they value effectiveness vs the scar tradeoff. That is a patient choice. My approach is I don’t tell patients what to do if there is more than one way to do a surgery. I educate the patient on their options and let them decide.
Thus your question of…would you perform it…can be answered two ways:
1) Do I think it is an effective and valid approach to webbed neck corrections? Yes as long as the patient is aware and can accept the scars.
2) Would I do it if asked by an educated patient…yes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a couple of questions regarding genioplasty and osteosynthesis plates:
1. If you have a lean face, would you be able to feel the osteosynthesis plate when touching your chin bone (i.e., when shaving or when scratching the chin bone)?
2. Can you feel the genioplasty osteotomies’ cuts/lines when touching your chin bone?
3. If I want to remove the osteosynthesis plate after the genioplasty. What would be the ideal time window? Is plate removal a straightforward procedure with low downtime?
4. It seems like they are different models of osteosynthesis plates. In the illustration of the procedure, one can see an X-like design placed in the middle of the chin bone; others are like small bars placed on the right and left of the chin bone. Is there any particular indication to use a specific model of osteosynthesis plate, or is this based on the surgeon’s preferences?
Thank you,
A: In answer to your bony genioplasty questions:
1) Hardware palpation is an uncommon occurrence given the thickness of the soft tissue chin pad even in lean faces.
2) In some patients the back end of the osteotomy lines (step offs) may be palpable. This is more evident in larger bony genioplasty movements.
3) Hardware removal can be done as early as 3 months after the original procedure when the bone is adequately healed. As you have surmised hardware removal is associated with a reduced surgery and recovery time.
4) There are numerous methods of genioplasty fixation, all of which can be effective when properly used Thus the method of fixation used is largely surgeon dependent. In larger and unique bony movements one method of fixation may be more effective than others.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 20 year old asian girl with lambdoid craniosystosis. Is there any skull reshaping possible for this??
A: You are referring to a flattening of the back of the head for which custom skull implants can create improved projection.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question regarding the intraoral approach to treating horizontal hyper-projection of the chin.
In your previous discussions, you emphasized that the most effective method for addressing hyper-projected chins in the horizontal plane is bone burring via a submental approach. However, it seems that many plastic and maxillofacial surgeons may lack the experience or training for this procedure and often prefer intraoral osteotomies instead.
I was wondering if a wedge osteotomy could be considered a viable alternative for reducing chin projection, as opposed to a reverse sliding genioplasty. If so, would the wedge osteotomy present similar aesthetic challenges as the reverse sliding genioplasty, such as soft tissue redundancy in the submental region and a boxy chin appearance in the frontal view? Additionally, would this technique inevitably reduce the vertical height of the lower third of the face?
I greatly appreciate your insights and guidance on this matter.
A: The key to any horizontal chin reduction lies in the soft tissue and not the bone. It doesn’t matter how the bone is reduced, what matters is what is going to happen to the excess soft tissue chin pad once its bone support is lessened. Only the submental approach allows for soft tissue removal/tightening. This issue is not going to be overcome by any intraoral osteotomy..
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 29 years old male who is going to have a sliding genioplasty (8-10 mm horizontal projection) next week.I am very concerned about the large step off areas located both superior and posteroinferior parts of my advanced distal chin fragment.I know that their occurence will be inevitable because of my large horizontal advancement(8-10 mm).
My question is that
Can we get a fully filled up smooth bone contour by properly grafting those two step off area bone gaps (particulary the one locating at the inferoposterior area of my chin) with allogenic bonny grafts like hydroxapatite which will be replaced by my own bone?
Thanks for answering.You are the most skilled plastic surgeon I have ever seen.
A: With a low angled and long osteotomy cut there is usually no significant step offs in my experience with 10mm+ sliding genioplasties. But for the sake of this discussion you are askng about grafting them should they occur to which I can say the following:
1) Hydroxyapatite is a ceramic calcium phosphate material which does not turn into bone….but it doesn’t have to as a permanent bone void filler material.
2) Allogeneic or cadaveric bone chips have the potential to allow bone ingrowth…although it is usually not robust or complete.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m wondering what I should do of my ears position and rotation, is it possible to rotate them to be more straight, or would a reduction help at all? I don’t know if they are lowset or just big and tilted. What can fix this
A: They may be a bit low set and with a backward tilt, neither of which can be changed. I would no advise ear reduction either as with a large concha that would look odd with the usual high-low ear reduction technique. The only ear reduction technique that could be done is a mid-conchal excision method but that may make more of backward tilt effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m not interested in having more chin. I have too much as is. am *scared of this ending up appearing as though I have a more lengthened chin, but I am still interested if this fixes the problem. There’s also a curved line above the tissue of my chin present when resting or static. Would this be addressed if I were to have this procedure?
A: Lengthening the chin does help soften the deep labiomental fold. The deep labiomental fold exists because the bone is not long enough to support the size of the soft tissue chin pad.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr., Eppley, would you have any idea what type of metal was used for chin implant screws in 1995? (I need to have a MRI, but no one knows what type of metal it is). Do you know if titanium screws were even used yet in 1995? Thank you!
A: Most likely titanium in 1995 but no one can say for sure. The x-ray will not provide that information as the material density between titanium, stainless steel, and vitallium is not that different.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some facial asymmetry and I’m potentially interested in pursuing custom implants as a solution.
When ordering a CT scan of the head, is there anything special I have to ask for to totally maximize image quality, other than that they use the thinnest possible slices and send me 100% of the raw data with no postprocessing?
A: We place the order for the 3D face CT scan so there is no confusion about how it is done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in learning more about testicle implants and exploring how it may be possible to achieve an oversized low “bull” look. I have seen a few different self achieved cases over the years that have turned out incredibly aesthetically pleasing to me, however the one I adore the most was self injected silicone (~700ml) which I have reservations on for obvious reasons. The “locked in” sheath look he accomplished is amazing, but I am not sure if that is achievable in a medically safe manner. I am fully fine with limitations on penetration if something like that is possible. My testicles naturally ride high and my scrotum is pretty stretchy which leads me to believe that I may be a good candidate for side by side. I would eventually like to have an oversized look similar to the attached images.
A: To achieve that look it would take custom side by side testicle implants. Whether that would require more than one set of implants to come closer to that look is the unknown question.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there, I have a question about skull reshaping. I have a shaved head so I’m concerned about scarring. Is there a way to do this surgery without visible scarring on the scalp?
My head shape and hair style is very similar to this. Before I proceed, I just wondered if this is a realistic procedure for someone who keeps a shaved hair style or if it must leave large visible scars.

 A: Sagittal ridge/crest reductions are one of the more commonly performed aesthetic skull reshaping procedures. The shaved head or bald male patient is the typical patient who presents for it. While no form of skull reshaping surgery can be without incisions and resultant scars the incision used in sagittal ridge reduction are very small and heal in a near imperceptible manner. No patient has ever stated the fine line scar bothers them or had requested a scar revision.
A: Sagittal ridge/crest reductions are one of the more commonly performed aesthetic skull reshaping procedures. The shaved head or bald male patient is the typical patient who presents for it. While no form of skull reshaping surgery can be without incisions and resultant scars the incision used in sagittal ridge reduction are very small and heal in a near imperceptible manner. No patient has ever stated the fine line scar bothers them or had requested a scar revision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a male looking into a chin augmentation as my chin is recessed upon researching the implantech website, I had some follow-up questions. If my primary goal is to increase lateral projection, and I have a deep mental crease: what implant would be most suitable for me, the flowers mandibular glove, the extended anatomical, or the Terino 1?
They all seem like great options, just unsure which would be best.
A: Since you mentioned lateral (horizontal chin augmentation along with a deep labiomental crease my assumption\ is that you may believe that one of the three chin implants styles may not magnify the depth of the labiomental fold. The reality is any form of chin augmentation os going to do exactly that regardless of chin implant style. It cannot be avoided as the labiomental fold is a fixed anatomic point that lies above the part of the chin that is affected by implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon