Your Questions
Your Questions
Q: Dr. Eppley, I have a 4 year old son born Jan 2021 who appears to have a “double lip”. He had a tongue and lip tie release at 8 months old in Sep 2021. I am including a zip folder with photos before the surgery and after along with videos to see how his smile was/is.
I need an opinion of someone who is an actual surgeon who understands facial muscles etc and not just a dentist with a knife. Hence why I am hoping you can just tell me if we are making a possible good next move or not. I really value your opinion after seeing some feedback you had previously put online about double lips and understanding the mechanics, cosmetics etc.
After the lip release at 1 year, the lip tigh looks high with a lot of thick tissue. He also has very tight buccal cheek ties that were never released at all. They are hard to picture, but were very thick, low, attaching right above where his teeth meet his gum. He won’t let us pull his cheek open to look so I imagine it is still present.
My concern is his smile now. He has an apparent crease across his upper lip when he smiles. It’s not obvious at all when resting – the smiling “big” creates it. The crease runs the full length of his upper lip. Is this a double lip? I’ve read that can be caused by trauma – did the release cause this? Double lips usually involve removing the redundant tissue but that would leave him with barely any upper lip. I can’t tell if the “double lip area” is outer or inner lip tissue that should even be resected. Before surgery, when smiling, did he have much of an upper lip? It was almost cliff-like if that makes any sense.
We are now faced with what to do next. We are exploring the option to re-release what’s left of his upper lip tie, and maybe ask for the buccal ties to be released too. With your knowledge of anatomy and the cosmetic side of things, would this potentially resolve the distortion in his upper lip? Or could it release the tension (particularly if the buccal is still strong + reattached upper lip).
We are beside ourselves wondering what the right thing is to do. I really appreciate anything you can offer.
A:Unless the upper double lip is causing a functional problem, which I am sure it isn’t, you need to leave it alone for now in a young growing child. I am not sure this was not caused by the maxillary frenulectomy…of which what the compelling need to do so was at such a young age. The upper lip may or may not have been caiued by the frenulectomy. This may be the ‘rabbit hole’ effect…you do one thing to fix one problem and then you develop a new problem. The goal is to get out of that cycle which in surgery is easy….stop doing surgery unless there is a compelling medical need to do so.
Double lip correction is an effective and straight forward procedure and can be done at any time. But I would let him grow some more and let his facial tissues develop further. I would only correct the double lip or any of the other associated issues when he is older and he finds it to be an issue.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley ,I have searched all over for assistance with a lower rib on the right side of my body. It cracked in year 2020 with a fall, when it healed I was told it over produced the bone substance used for healing the cracked rib. This has caused me to have severe discomfort as it feel like I am being stabbed from the inside out. At one point they did an exploratory surgery to determine it was in fact my rib. I have been to: 2-3 PCP, an orthopedic surgeon, a neurologist ( thinking numbing nerves would help ). I am out of options, everyone tells me I am stuck with this. I can’t workout anymore, run and jump as it pokes me, sex is hard. It is really killing my quality of life and depressing me. I would like to see about fixing it, as it’s causing pain. Yes, some days are worse than others. I can’t even sit at times. I have been googling things and your practice came up, is this something you would be interested in looking into for me? I have read it may have to be out of pocket, but I have also read since it’s related to a past injury and causing pain we can work in insurance as well. Please help
A:I assume the exact rib is known and there is an x-ray (plain film) that shows its location. (need that info) Rib resection would be the logical treatment approach. The only question is where it is located and can it be safely reached.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley,I am inquiring about a sliding genioplasty. I have attached some photos to show what would roughly be my goal in this surgery. My chin is recessed and seems that it would require some downward and forward repositioning to achieve a desired result. I was wondering if this seems within reach with this type of surgery.
A:I don’t think that type of chin augmentation change is completely achievable. What you are showing is a significant horizonal advancement and significant vertical shortening….a change only remotely possiboe with a sliding bony genioplasty., The problem is that with a conventional sliding genioplasty it would be very challenging and almost impossible to get that amount of vertical chin shortening no matter how much you tilted up tehg repositioned chin bone. Such a change requires a jumping genioplasty where the cut chin bone is moved directly in front of or ‘jumped onto the bone above it. The problem with the jumping genioplasty technique is that you never know whether the attached muscles to the down fractured chin segment will allow that amount of stretch to make that jump….sometimes it will and others it may not in my experience.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, “Hello I read online you can reduce the width of the hips/iliac crest.I need some information, i am from the Netherlands but did not founded anyone here how does this surgerywhat are the disadvantages? Can complaints arise after the surgery?”
A: You are referring to iliac crest reduction which. is associated very issues if any other than the small incision/scar needed to do so. The most important issue is whether the procedure would be effective for your goals. I would need some hip pictures to do some imaging of potential results.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, do you offer a service to design a chin/jaw implant only from a supplied CT scan or solid model of the Mandible (pre-segmented). The design would be used to print in PEEK for use by another doctor/patient outside the USA. Thanks
A: I do not design implants for other surgeons to place.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Can my visible temporal arteries be ligated? I have attached pictures.
A: These are classic prominent temporal arterial branches that are takeoffs of the main temporal artery. (not the more common anterior branch of the superficial temporal artery) But regardless of this anatomic variation they can be successfully ligated.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I hope this email finds you well. I would like to inquire about treatment options for plagiocephaly. Specifically, I have noticed that the left side of my face is more protruding compared to the right, with a tilt to the right as well. I wanted to ask if it is possible to address this asymmetry through cheekbone reduction and shaving, particularly the anterior zygomatic prominence, as it appears longer on the affected side. Additionally, I would like to know if anything can be done to address the protrusion of the eye on the same side. Furthermore, I have noticed that the skin over the ear (I believe it is related to the masseter muscle) appears baggy or “puffy.” Is there any way this can be stretched or addressed without a skull implant? Otoplasty and a orthognathic surgery is something I’ll definitely check to. Thank you for your time and expertise. I look forward to hearing your thoughts.
A: When it comes to reductive facial asymmetry corrections there are a variety of bone reduction techniques of either osteotomy or ostectomy. (shaving) How effective they would be requires a 3D CT craniofacial scan to assess the bone differences and thicknesses on the larger asymmetric side. That is where to begin the facial asymmetry surgery process.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I am interested in this technique for its potential to improve scalp hair growth, I shaved my head once and I realised that I have quite an odd shaped head, and I also read that perhaps skull shape, effects hair growth. I guess through restricting or liberating blood flow to the follicles.
A: Having performed over 500 skull implant cases I can’t say any patient has reported after surgery that they noticed increased hair growth. In theory the placement of s skull implant does block vascular ingrowth from the bone or fascia over which it lies. To maintain scalp vascular homeostasis blood must be increased through peripheral channels to the expanded scalp. While it is tempting to think that this vascular change can stimulate the hair follicles I have not conclusively seen it. While I wish that was true the proven benefits of skull implants are for contour change.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I’m looking to get a custom jaw implant later this year. Do you have any specific information about the procedure and recovery that might help me make a decision about choosing you as my doctor? I will be coming from New Mexico and will be alone. Will I need someone to take me back to my hotel after the surgery or is there something else you can provide? Thank you
A: Having performed over 500 custom jawline implant surgeries and having written about this topic extensovely I would refer you to the following three websites which provides a wealth of information about the procedure.
www.exploreplasticsurgery.com indications, surgical technique, implant designs, recovery
www.eppleycustomfacialimplants.com implant designs
www.eppleyplasticsurgery.com before and after patient photos
Having an international practice where most patients fly in from all over the world for surgery, and most are traveling alone, we are well versed in managing the logistics of the surgery from arrival to departure.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, What materials available for implants? I see he uses a lot of silicone and was wondering why that is. I prefer different material would that be okay?
A: There are a variety of materials for custom facial implants including solid silicone, Omnipore/Medpor, PEEK, PEKK and titanium…each with their own advantages and disadvantages There is no perfect faciak implant material.
While patients and even most surgeons get caught up in the implant material properties on a handling basis, often with very erroneous perceptions in vivo, to the body an implant is an implant is an implant. It is still a foreign material and no material offers any different or superior biologic benefit.
What separates these facial implant materials is not their biologic responsesbut other features such as cost, design limitations, and ease of placement and revision/removal .
Given that the revision rate of any custom facial implant is in the 40% range (shocking to patients but true), the concept of ‘easy in, easy out and easy back in’ has great clinical merit. This is where solid silicone has a significant material benefit and explains its broader clinical use than the other materials.
That being said it does not matter to me what material a patient wants to use as I have placed and removed every implant material that is available. What I care about is that the patient understands the advantages and disadvantages of their material choice.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in feminization surgeries. I currently present male, and would like to do surgeries before moving on. Ultimately I would like to have a number of procedures, but have no idea about cost or insurance. I had gastric sleeve performed 18 months ago and have lost 100 lbs. 5′ 9″ currently 180 up from a low of 170lbs. 48 years old next month. Procedures i am interested in: Butt and hip augmentation. (Currently thinking solid implants are preferable to fat grafting) Floating rib removal and/or repositioning Mid rib(lower attached ribs) repositioning Clavicle reduction Liposuction. (Belly, upper/lower back, thigh..etc) Overall skin removal and tightening (belly, butt, thighs, lower, mid and upper back) I am willing and able to travel for procedures and recovery. I would really like to get info on which procedures can be done simultaneously and approximate cost. Would like complete as much at one time as possible. Would also be interested in FFS at a future time. Thank you
A: When it comes to body feminizing surgery you have one unique anatomic feature that separates you from most other patients…..the large amount of weight loss. (massive weight loss or MWL) This creates the need for numerous body contouring procedures (skin removal and tightening) that do not necessarily have feminizing effects but are more of a ‘reconstructive’ nature. As a result considerable thought must begin to both MWL and body feminizing procedures to create a staged surgical plan for maximum efficiency and effectiveness.
That process begins by looking at your body pictures from numerous angles (front, back and sides) for an initial assessment.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in replacing my PEEK infraorbital-malar implants as they don’t saddle the rim and as a result they stick put unnaturally. These implants were placed intraorally at the time of double jaw surgery.
A: Be aware of two very relevant aesthetic issues. 1) when have to saddle the infraorbital rim you have to use a lower eyelid incision to do the dissection needed as well as to ensure proper placement and 2) PEEK is not a good implant material for thin tissues like the lower eyelid and orbital rims as it can not be made withj feather edging as it is machined in its fabrication. You will likely end up with visible edging even if it saddles the rim. …less than what you have now just at a different level and degree
There is a reason your current PEEK implants don’t haver a feathered edge design and look bulky…which is very obvious in bot the design and after actual placement. This is a design limitation of all very rigid materials that have to be machined in manufacturing. There is always going to be at least a 1mm edge. This is not an aesthetic issue in thicker tissues like the jawline and lower cheeks. But it will be one around the orbital rim which is an unforgiving implant placement site.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a separate medical enquiry, regarding bone burring to correct the prominence of my forehead. Can this be done please. Not sure if I’m imagining things but my right side seems to appear a bit smoother than the left, so it’s this left side I would’ve wanted addressing.
A:Are you referring to the prominence of your forehead or that of the brow bones. I ask because I don’t see any true forehead prominence. The other issue is for any forehead work where is the scalp incision going to be placed to do it. In the male with short hair here is no aesthetically hidden place to put it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley I hope this email finds you well. I’m reaching out to ask about surgery for the two horns on my forehead that stick out noticeably. I’ve attached a recent photo to show how they usually look.
I have a few questions:
1. How is the procedure done?
2. How much does it typically cost?
3. Will I be able to safely play soccer afterward, especially since I frequently head the ball?
I’d appreciate any details you can provide and look forward to your guidance.
Thank you for your time and expertise.
A:Forehead Horn reduction is typically done by bone shaving through a small scalp incision. In very large forehead horns like yours the key question is whether the bone is thick enough in the horn area to permit an adequate reduction. This requires a CT scan to make that assessment. Provided reduction can be safely done there would be no postoperative limitations in terms of playing soccer or any other activity where trauma to the head can occur.
The CT scan can be done in our local area and we provide the order form at a local imaging facility to have it done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m planning to have a genioplasty with you this spring and had a few questions about the healing process.How long does it usually take for the chin bone to heal enough to avoid bending in case of trauma.Would it be around 2, 4, or 6 weeks post op?
A:The chin bone is generally healed enough after 6 weeks that trauma to it would not change the bone position.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have very thin lower forearms from the wrist back. I know it is possible to have implants to the upper forearms but would the dr be able to use implants to thicken the lower forearms?
 A:Your pictures show a lower forearm deficiency which is most apparent in the dorsal position. (as you have shown all pictures from that perspective) Between largely being a dorsal deficiency and not having to cross the wrist this is a favorable area for implant augmentation. These would be suprafascial implants that wrap onto the volar part of the forearm which are ultrasoft with very feathered edges. (see attached picture) These would be made by taking measurements of the lower forearm area that needs the augmentation. (you can take the length vs width measurements) This procedure would be performed under local anesthesia.
A:Your pictures show a lower forearm deficiency which is most apparent in the dorsal position. (as you have shown all pictures from that perspective) Between largely being a dorsal deficiency and not having to cross the wrist this is a favorable area for implant augmentation. These would be suprafascial implants that wrap onto the volar part of the forearm which are ultrasoft with very feathered edges. (see attached picture) These would be made by taking measurements of the lower forearm area that needs the augmentation. (you can take the length vs width measurements) This procedure would be performed under local anesthesia.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can Botox effectively reduce the size of the temporal muscle long term?
A: No, its limited effects are temporary.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q:Dr. Eppley, I am scheduled to have braces on the 30th can or will that interfere with cheek implant surgery?
A: No it will not. Braces in the teeth do not get in the way of intraoral access for the placement of cheek implants.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a previous patient of Dr. Eppley (Sept 15, 2022 surgery date). That procedure involved a surgically implanted plate and screws.I have an upcoming MRI and I need to confirm what implant material Dr. Eppley used, to be sure that it is completely MRI-safe and not at all magnetic. Can you check with Dr. Eppley and your documentation to find out?
Thanks for your consideration,
A: All metal implants used in the face since the early 1990s is made of titanium, a non-ferromagnetic metal.Thus any metal hardware implanted in your face would be MRI compatible.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, im interested in custom implants to make my masseter muscle bigger. I already have a jaw implant inserted because my jaw was shaved a decade ago and it ended up being a bad choice. Along with the jaw shaving they ended up shaving a good amount of my masseter which I desperately want the appearance of back. My face was much wider and now it is narrow. I have had fat taken out of my face, so im not talking about that, but the overall shape of the face. I last picture is the look i’m going for.
A: The challenge that you now have is that adding implants to the implant you have in place would be very difficult from an intraoral perspective. That is clearly a titanium or PEEK implant material in which fixing an implant onto it would be difficult. This is best done from an external approach where implant placement and fixation would be more assured.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Im wondering if I can get Kybella after a custom wraparound jaw implant?
A: Yes you can. Since Kybella is usually injected into soft tissues to reduce fat under which implants do not lie they would be perfectly safe to use.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in 5mm mouth width expansion per side, I was wondering how long it would take for “normal” scarring that usually happens as a trade-off to look acceptable enough to not have it be easily noticeable by other people or distract from the result.
A: Corner of mouth scars generally take 3 to 4 months to mature particularly in intermediate skin pigments.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in revision options for my custom jawline implant. During my last discussion with Dr. Eppley, he mentioned several options beyond a full revision. One option involved adding additional components to the existing implant to enhance projection and angles. He also suggested a soft tissue graft to address and cover the bulging near the masseter muscles.
Could you please provide more details about this approach? Specifically:
• Would the current implant need to be removed to incorporate the new components, or can they be added without removal?
• How are the additional parts secured—are surgical screws or adhesive methods used?
A:‘During my last discussion with Dr. Eppley, he mentioned several options beyond a full revision’
FYI it would be a full implant replacement….not a revision. A revision is when you are taking what you have and try to modify it. Plus a revision relates to the primary surgeon wo did the original work. When a new surgeon assumes that initial work it is a secondary procedure not a revision. While a bit semantical there are very different implication between the two.
‘One option involved adding additional components to the existing implant to enhance projection and angles’
 You are referring to Transcutaneous Soft Tissue Jaw Angle Implants. A common technique that I employ to treat masseteric muscle dehiscence with implant reveal. It is the only technique that works if one desires to keep their current jaw angle implant shape. The alternative is to change the implant with a new design that doesn’t have such a square jaw angle shape…which is what caused the problem in the first place.
You are referring to Transcutaneous Soft Tissue Jaw Angle Implants. A common technique that I employ to treat masseteric muscle dehiscence with implant reveal. It is the only technique that works if one desires to keep their current jaw angle implant shape. The alternative is to change the implant with a new design that doesn’t have such a square jaw angle shape…which is what caused the problem in the first place.
Soft tissue jaw angle implants are placed in the soft tissues overlying the current implants, they are not bone implants. (see attached picture)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in Lefort 1 osteotomy surgery. The reason I want to have this surgery is that the maxilla, the middle part of my face, is long and I want to make it look shorter. My face, which is between the eyes and the lips. how much of a change there could be?
A: You are under a common misconception that if you shorten the maxillary bone (LeFort I impaction) your external midface appearance will get shorter…which it will not. The LeFort I impaction is for the treatment of the excessive gummy smile patient to achieve less tooth and gum show. It can not shorten the appearance of the midface as where does all the soft tissue go if the bone is shortened? It doesn’t go anywhere…it will remain the same.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What is the recovery time for temporal muscle reduction? I suffer from migraines a lot, would Botox injections help shrink the temporal muscle?
A: It takes a good 2 to 3 weeks for the swelling to resolve. But there are no physical restrictions during the recovery.
My assumption in your questions is that you may be seeking temporal reductions for migraines?? If that is the case the important question is where is the location of the migraine pain in the temporal area? Knowing that information will determine whether surgical reduction or Botox is the appropriate treatment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
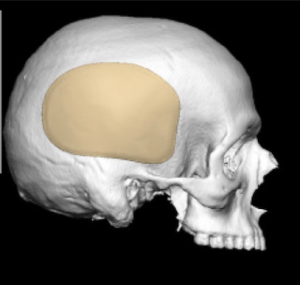
Q: Dr. Eppley, I’m interested in aesthetic skull reshaping surgery & the costs involved. I’ve attached a few photos to see of the desired “after” results are possible and what costs would be involved.
A: Based on your own imaging it appears that you have done a modest left forehead-parasagittal augmentation. This would be very achievable as with a 3D Ct scan one could see the difference between the two sides and from that difference a small custom skull implant can be designed/made to provide a symmetry-achieving effect.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi Im very interested in ZSO on my right cheekbone to expand and match my left.
A: The main concept to grasp is that when one side of the cheek is asymmetric (smaller ot bigger) it is a three-dimensional problem not a two dimensional one. The cheek is a solitary projection from the side of the midface so there is more than just a width deficiency when it appears amaller. The zygomatic sandwich osteotomy (ZSO) creates a two dimensional effect not a 3D one. This will likely become glaringly apparent when the ZSO operation is performed. This is why a 3D cuystoim cheek implant produces a better aesthetic result from all facial angles.
But even if a ZSO is to be performed the critical question is how much expansion is needed to optimie cheek symmetry. This is where a 3D CT scan of the face is needed to determine not only how much width addition is needed but how significant the 3D bone differences are
Dr. Barry Eppley
World Renowned Plastic Surgeon
\
Q: Dr. Eppley, I am interested in changing the shape of my head. Attached below are two pictures of me and 3 picture that I can find to best describe what I want. Hope this helps.
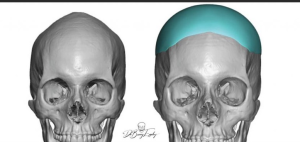
 A: Based on the pictures you have sent you appear to have an inverted V shaped top of the head with narrow sides. (parasagittal and temporal deficiencies) The two skull implant shapes you have shown are designed to address those goals and can be placed during a single surgery.
A: Based on the pictures you have sent you appear to have an inverted V shaped top of the head with narrow sides. (parasagittal and temporal deficiencies) The two skull implant shapes you have shown are designed to address those goals and can be placed during a single surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi!! I just heard that dr barry eppley had done inferior orbital box osteotomy, which is less riskier than 360 degree OBO. Actually i just wanna reduce my IPD as a woman. Can this technique reduce my IPD by upto 5 mm. Also can Dr. Eppley perform it?
A:Inferior box osteotomies can be effective for modest IPD increases but not for IPD decreases.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I was looking at some videos on youtube of Dr. Eppley performing this procedure and I was wondering if the implant that is slid under the skin on the scalp could cause some kind of damage to hair follicles?
Also once the surgery is performed could the implant move? If the back of the head was to be hit or hit some sort of surface could the implant be displaced under the skin?
Would wearing a motorcylce helmet also potentially cause this? Or other complications?
A: 1) The implant is placed on the bone under all five layers of the scalp way under the location ofmthe hair follicles. As long as the patient doesn’t insist on having an implant that is too bog there is no excessive stress on the hair follicles. (shock loss)
2) Because of their large surface area coverage and the tightness of the overlying scalp skull implants can never move or change position.
3) Skull implants are impossible to fracture or be damaged. As a result ther are very much like putting a bumper on the skull….providing inadvertent protection to the skull from any future trauma.
Dr. Barry Eppley
World Renowned Plastic Surgeon