Your Questions
Your Questions
Q: Dr. Eppley, Looking into the mommy makeover. I am 35 years old and I have five kids. Exercise is not gonna get it done, I can see that now. I wanna be ready for this summer. I have attached some pictures of my body so you can determine what needs to be done.
A: Thank you for sending your pictures. They give me a clear idea as to the exact Mommy Makeover procedures you need. From an abdominal standpoint, you need a full tummy tuck with flank liposuction. You have excess abdominal skin that is loose and hanging over your waistline. Full ness from fat extends around your waistline into your back. From a breast standpoint, you need implants with a vertical breast lift. Your breasts have lost substantial volume and are saggy (ptois) with the nipples hanging below the lower breast crease.
Both breast and abdominal reshaping procedures can be done during the same surgery, hence the derivation of the Mommy Makeover name. In a single operation, often lasting 3 to 5 hours depending on what is being exactly done, a women’s body can be very positively changed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I definitely want to remove my acne scars, but other than that, I’ve been given so many different suggestions, I’m not even sure anymore. For the acne scar laser resurfacing, I was told my skin type has a high chance of pigmentation. What are safe options? I do want a rhinoplasty, but I want it to be very subtle, and I’m mainly interested in fixing the tip that sort of goes down like a beak. How is this usually corrected? Also, you mentioned that it appears my buccal lobe was removed. Does this mean the maximum amount was taken out? I am now 2.5 weeks post op. Do you think my final results will give me the skeletonized appearance I desire? I still feel 2 grape sized bumps, hard as rock, when I push down on my cheeks.
A: What would structurally benefit your face is not a mystery and is very straightforward…it lies with your nose and chin. Your chin is very deficient, by at least 9mms, and is one feature that will keep your face from ever having a very defined and angular appearance., By using a sliding genioplasty to bring it forward it will improve your facial profile and help create a more defined appearance in the front view.
You have a very classic ethnic nose with a broad flat tip that has little support and no projection, hence a rounded tip that droops down. An open tip rhinoplasty will reshape the tip and give it a better profile and a more narrow appearance in the frontal view. You would also need some upper dorsal/radix augmentation.
Fractional laser resurfacing is the only type of acne laser resurfacing that you should have as this has a very low risk of any hypopigmentation problems. It will take more than one treatment and the best result you can hope for is about a 50% improvement in the appearance of your facial acne scarring.
It takes a full 3 months for the buccal space where the fat pads were removed to become soft and not feel as hard lumps, this is perfectly normal to feel what you are feeling at just 3 weeks after surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I know I want infraorbital rim implants but an additional concern is the changes in the skin under my eyes that I have noticed in the last three to four years. I have attached a PDF of some of my eye pictures. They shows the bunching up and “crepey” skin that tends to exacerbate my undereye issues and tired appearance. Even though the lower photos are the effect with an extreme smile, this tends to occur even with a mild smile, and really affects my self-esteem. I was wondering how infraorbital implants and/or fat relocation will ameliorate these folds. Though I had a series of three micro laser peels this last year, they did little to address this issue. I just would like to be realistic as possible in terms of the outcome of this procedure.
 A: The smile animation ‘deformity’ around the lower eyelids (under eye wrinkles) is a tough one since it is a muscular action effect and not a structural problem. No amount of static skin resurfacing will help a dynamic movement issue. The infraorbital rim implants will make some improvement in it due to volume expansion and some diminution of muscular excursion but ultimately animation wrinkle deformities respond best to Botox injections.
A: The smile animation ‘deformity’ around the lower eyelids (under eye wrinkles) is a tough one since it is a muscular action effect and not a structural problem. No amount of static skin resurfacing will help a dynamic movement issue. The infraorbital rim implants will make some improvement in it due to volume expansion and some diminution of muscular excursion but ultimately animation wrinkle deformities respond best to Botox injections.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, It appears that very few plastic surgeons offer a permanent solution for labiomental fold treatment (reduction). After reading your case study on the subject, and considering other options, I’ve decided to either address this issue with Silikon-1000 a permanent filler, or with an implant which I prefer. You would be my choice of surgeons for the implant. But I have one problem. As far as I’m concerned, I do not want any scars, regardless of how small or imperceptible they may be. My question to you is… Would it be possible to have the implant put in place from inside the mouth rather than through small incisions on the skin?
A: Labiomental fold treatment (reduction) is a challenging procedure and I would not refer to any treatment of it as permanent since facial aging is a progressive procedure. I would not recommend a subcutaneous labiomental fold implant be placed through an intraoral incision. Besides not being able to get it in the ideal place, there is going to be a higher risk of infection dragging the implant through oral mucosa. I think an implant is the right procedure for labiomental fold reduction, just not placing in through the mouth.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My face is really chunky and rounded and just full. I would really like to have a slim face with defined cheekbones and a square jaw. I was curious about whether any types of would be capable of altering my facial features. Also if I have facial surgery can I get liposuction in various areas consisting of belly, butt, back, and male breasts, thighs, and arms.
A: In regards to your face slimming desires, the first most important is whether any significant slimming effect with better definition can be obtained. Not all face types can be converted into those desired changes. I would need to see some pictures of your face to determine what may be possible. Fat removal procedures can have some mild to moderate facial slimming effects. Skeletal augmentation such as cheeks, chin and the jawline often produce more profound facial changes.
When it comes to liposuction in men, by far the most common areas would be the abdomen, flanks (love handles) and chest. Thigh, arms and back would be very uncommon requests. (quite frankly I have never had a male request for liposuction in those areas my entire practice career) This raises the question of what your overall weight and body type is. I would be curious to see pictures of these areas of body concerns to determine if liposuction is the appropriate treatment.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in getting hip implants to achieve an hourglass figure. I hate the indent I have in my hips and would like implants to be inserted up over the iliac crests if I’m not mistaken. The indent has gotten bigger and worse as I tried to gain weight in the hips, but of course I can only do so much with the bone structure I have. My questions are, how wide can the hip implants be? I’m typically trying to achieve at least around an inch. And also I’m interested in getting a labiaplasty to reduce my labia, so could this procedure be done at the same time? Thanks
A: Hip implants are an option for your hip indents but placing them that high up over the iliac crests may be problematic in terms of the waistline effects of wearing clothes. Given your body type I would first consider a fat transfer as you have good volume to be harvested from the knees, inner thighs and some from the abdomen. This is the way to put fat there as opposed to trying to gain weight by your diet. While fat is unpredictable in terms of its survival, it is perfectly safe, natural and would prepare the tissues better if you ever considered placing implants in that area. (although the goal would be to never have to exercise that option) Labiaplasty could be performed with either fat grafting or implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, It appears that very few plastic surgeons offer a permanent solution for labiomental fold reduction. After reading your case study on the subject, and considering other options, I’ve decided to either address this issue with Silikon-1000 a permanent filler, or with an implant which I prefer. You would be my choice of surgeons for the implant. But I have one problem. As far as I’m concerned, I do not want any scars, regardless of how small or imperceptible they may be. My question to you is… Would it be possible to have the implant put in place from inside the mouth rather than through small incisions on the skin?
A: Labiomental fold reduction is a challenging procedure and I would not refer to any treatment of it as permanent since facial aging is a progressive process. I would not recommend subcutaneous nasolabial fold implants be placed through intraoral incisions. Besides not being able to get it in the ideal place, there is going to be a higher risk of infection dragging the implant through oral and nasal mucosa.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to know which its a better choice between a facelift or laserlift. My concern is since my face is thin and non-fat, its more sagging skin around my jaw line and a little on my neck. I don’t know if the laser will really tighten my skin or cutting it will produce a better result.
 A: While I don’t know what your face looks like and the degree of jowl and neck sagging that is present, it is fair to say that any form of a so called ‘laserlift’ pales in comparison to what a real surgical facelift can do. All so-called non-surgical ‘facelift’ technique only produce a mild amount of skin tightening that is very temporary at best. Regardless of the device used, its results are extremely modest and are best reserved for those patients whose skin laxity issues are so slight that the consideration of any form of a facelift is premature. Think of non-surgical facelift methods as a delaying tactic to push back by a few years the need for surgical improvement. In short, non-surgical facelifts are not a substitute for even the most minor form of a surgical procedure. Be aware that facelifts today have evolved so that they are done in minor to major forms depending upon the amount of jowl and neck work needed. They range from simple jowl lift procedures to more extended neck-jowl lifts. Often the debate between non-surgical vs surgical facelifts comes down to a decision between non-surgical skin tightening and a jowl lift. (level 1 facelift) For the economic investment and duration of effect, the far better value is almost always the surgical facelift hands down.
A: While I don’t know what your face looks like and the degree of jowl and neck sagging that is present, it is fair to say that any form of a so called ‘laserlift’ pales in comparison to what a real surgical facelift can do. All so-called non-surgical ‘facelift’ technique only produce a mild amount of skin tightening that is very temporary at best. Regardless of the device used, its results are extremely modest and are best reserved for those patients whose skin laxity issues are so slight that the consideration of any form of a facelift is premature. Think of non-surgical facelift methods as a delaying tactic to push back by a few years the need for surgical improvement. In short, non-surgical facelifts are not a substitute for even the most minor form of a surgical procedure. Be aware that facelifts today have evolved so that they are done in minor to major forms depending upon the amount of jowl and neck work needed. They range from simple jowl lift procedures to more extended neck-jowl lifts. Often the debate between non-surgical vs surgical facelifts comes down to a decision between non-surgical skin tightening and a jowl lift. (level 1 facelift) For the economic investment and duration of effect, the far better value is almost always the surgical facelift hands down.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 32 year-old male that has Poland’s syndrome and am interested in pectoral implants. Can you fix my chest?
 A: I can see from your pictures that you have a mild case of Poland’s that has affected the right side of your chest. The right pectoralis muscle is a little bit smaller and the nipple-afeolar complex on the right side is a little higher. I suspect that when you raise your right arm, compared to the left side, that the asymmetry between your chest sides becomes even more apparent. There are two approaches you can use for your improving the appearance of your Poland’s chest deformity. One approach is to just place a small pectoral implant on the right side with a nipple lowering procedure. Fat injection grafting as opposed to an implant can also be used although it is less reliable than an implant in terms of permanent volume. A second approach is to enhance both sides of the chest with pectoral implants (right bigger than left) with a right nipple lowering procedure. The choice between the two depends on how you view the normal left side of our chest. If you are happy with it, then you go with the first approach. If you are looking for improvement on both sides, then you go with the second approach.
A: I can see from your pictures that you have a mild case of Poland’s that has affected the right side of your chest. The right pectoralis muscle is a little bit smaller and the nipple-afeolar complex on the right side is a little higher. I suspect that when you raise your right arm, compared to the left side, that the asymmetry between your chest sides becomes even more apparent. There are two approaches you can use for your improving the appearance of your Poland’s chest deformity. One approach is to just place a small pectoral implant on the right side with a nipple lowering procedure. Fat injection grafting as opposed to an implant can also be used although it is less reliable than an implant in terms of permanent volume. A second approach is to enhance both sides of the chest with pectoral implants (right bigger than left) with a right nipple lowering procedure. The choice between the two depends on how you view the normal left side of our chest. If you are happy with it, then you go with the first approach. If you are looking for improvement on both sides, then you go with the second approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was told in a consultation with a local plastic surgeon that I needed cheek implants, chin reduction (just shaving the bone down and removing some fat/skin), and a little off the hump in my nose. That is the basis for my inquiry. Even though those were his suggestions, I still wanted to keep looking because I didn’t see that he had a very extensive client base where he had performed all of those at once…or more than one procedure at the same time.
I normally pose differently and make myself look better in pictures, but my profile is very flat in the cheek area and prominent in the chin. I’d like to get this corrected somehow, but I think with so many things to address at once, I get concerned that the surgery would be very noticeable and I would look like a different person all together…
A: In reviewing your pictures, I could make the following comments:
Your vertically long but non-projecting chin would be best treated by an extra oral vertical reduction ostectomy. (submental chin reduction) A burring technique would not remove nearly enough. You need at least 8mms or more off to really make a difference.
Your flat mid facial profile is ideally treated by a combination of paranasal and malar shell cheek implants. This will help pull out the entire midface. (both the nasal base and the cheeks)
You do have some significant facial asymmetry that actually affects the whole left side of the face. (which is shorter) The chin reduction will help with the lower facial asymmetry. The eye asymmetry, however, will not be improved.
One realization is that these changes will make a facial difference with much better balance…but it will likely be noticeable as your face gets vertically shorter and more horizontally projected.
Dr. Barry Eppley
Indianapolis, Indianapolis
Q: Dr. Eppley, I am interested in a rib graft rhinoplasty. I consulted with a local doctor and he said that because of the height and projection of the nasal implant it made my nostril more visible. I think I’m leaning more towards rib cartilage as use for the implant. What I want to accomplish is a nose that’s less deviated, less nostril visibility and appears less short. Also, being that I have thin skin, what can we do to prevent the rib graft from being visible when someone is looking at me? At the moment, my nose looks thin and skeletal like and I want to remedy that.
For my chin, I want the implant removed and fat grafting done to the area. I just want a chin with an appropriate projection in relation to my face and nose. Also, I would like to see if we can use fat grafting to restore a natural jawline to my face before resorting to implants. I would like fat grafting to my nasal labial folds as well as the cheek/hollows of my eyes.
A: There us nothing wrong with using injectable fat and that is clearly a treatment approach that you find most comfortable. However, you need to be aware that fat grafting never works the same as an implant regardless of how it is presented in surgeon’s websites. Fat grafts are soft and don’t have the same push on the overlying soft tissues. As a result, the amount of augmentation and the definition it creates is far inferior to a firm implant. But with that being said, I think fat grafting is reasonable since you have other fat grafting needs so ti is worth the effort. There is certainly nothing to lose by so doing.
It is difficult in any rib graft to a nose with thin skin to not have it look skeletal. Ways to lessen that aesthetic risk are carving the edges of the graft so that they are round and not sharp and to cover the rib graft with a thin layer of allogeneic dermis. Together these two approaches can be effective at softening the look of a rib graft to the nose.
In replacing a chin implant with fat, it is again important to know that it will not create the same effect and many not even survive inside the relatively avascular lining surface of the chin implant pocket. But again it is a reasonable approach with little risk other than complete graft absorption.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had buccal fat pad removal (buccal lipectomy) recently and am already seeing positive results. I can see my strong cheekbones a lot more. However, there are parts of my face that still display bits of fullness. Based on your responses to other questions, it appears I still have some perioral mounds. I am considering liposuction in this area. However, my concerns are a return of fat after treatment. I’ve read different online opinions that indicate fat can return after liposuction. As such, my questions are:
1. If I get liposuction on my perioral mounds will the fat go back to my buccal fat pads to compensate for the fat loss in my perioral mounds?
2. If I choose not to get liposuction on my perioral mounds, but either gain some weight, or stay the same weight, will my buccal fat pads eventually return? From what I recall, I had my surgeon take out as much buccal fat as possible, but the temporal part was of course left alone. Can buccal fat regenerate?
3. Lastly, I am also considering some type of laser resurfacing procedure for acne scarring but I am worried the regeneration of new skin cells promoted by these laser procedures will bring my buccal fat pads back. Is this possible?
 A: When it comes to liposuction, you have to separate face and body liposuction as the long-term results can be quite different. This is especially true for the unusual buccal lipectomy procedure. To answer your specific questions:
A: When it comes to liposuction, you have to separate face and body liposuction as the long-term results can be quite different. This is especially true for the unusual buccal lipectomy procedure. To answer your specific questions:
- Once the buccal fat pads are removed, they will never come back. A buccal lipectomy is the most unusual of all fat removal procedures in the body as it is a total glandular excision not subtotal fat extraction. Fat only returns in the body by cell hypertrophy not new fat cell growth.
- Buccal fat cells, like almost all fat cells in the body, do not regenerate or make new cells. Only the residual or existing cells can get bigger.
- A skin laser treatment will have no effect on the deeper underlying fat in terms of ever promoting fat cell hypertrophy or fat cell replication.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a subnasal lip lift proceure but I must admit that the procedure worries me. There seems to be lots of unhappy results, in which columella has gotten longer, nostrils became wider, and people end up looking like rabbits etc . My local surgeon says that in his experience, after the lip lift, is that with time the lip always goes back to its original position, due to the weight. Do you use a special kind of suture and/or technique that would prevent the lip from pushing back down?
 A: While the subnasal lip lift procedure is relatively simple to do from a surgical standpoint, it is a procedure that has no tolerance for error. From selecting the right patient, to the design of the skin removal area and to the method of closure, all impact what the final result will look like. There are several key points to a successful lip lift result. The first is to recognize that its effects are on the central or cupid’s bow area of the lip and does not extend to the mouth corners. Secondly, the excisional pattern of design should mimic exactly the curvatures of the lip-nasal base junction and should not extend around to the side of the nostrils. Third, the amount of vertical skin excision (as measured at the philtral columns) should never, and I repeat never, exceed 25% in a man and 33% in female. Lastly, no attempt should be made to prevent some after surgery relapse by sewing muscle, removing muscle or otherwise trying to secure the skin down in a tightened fashion.
A: While the subnasal lip lift procedure is relatively simple to do from a surgical standpoint, it is a procedure that has no tolerance for error. From selecting the right patient, to the design of the skin removal area and to the method of closure, all impact what the final result will look like. There are several key points to a successful lip lift result. The first is to recognize that its effects are on the central or cupid’s bow area of the lip and does not extend to the mouth corners. Secondly, the excisional pattern of design should mimic exactly the curvatures of the lip-nasal base junction and should not extend around to the side of the nostrils. Third, the amount of vertical skin excision (as measured at the philtral columns) should never, and I repeat never, exceed 25% in a man and 33% in female. Lastly, no attempt should be made to prevent some after surgery relapse by sewing muscle, removing muscle or otherwise trying to secure the skin down in a tightened fashion.
If you add up all of these points together, one can see that the key to a happy subnasal lip lift result is to not try and over do it. Overcorrection and lack of attention to detail makes for most of unhappy subnasal lip lift results.
It is important to recognize that in the first six months after surgery there will be some ‘relapse’ of the initial result. This is due to natural skin stretching from lifting any type of tissue upward. (no different than a browlift or facelift) My observations have been that it is about 25% to 33% vertical change in the first six months after the procedure. But trying to overcorrect to factor in this after surgery lengthening is a mistake. It is far better to have a natural looking lip result that a patient wants to secondarily revise (about 10% do) than to have an initial overdone too pulled up look that the patient is waiting months for it to settle down and drop.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in some type of temporal plastic surgery. As you could see from my pictures my temples are not symmetrical. Even though I was born with my temporal muscles having a natural arch, an injury on the left side tore that muscle At least that’s what I hypothesis. What are your thoughts, regarding an operation that will make my skull shape even again? Thanks for your time.
A: What I am seeing is that you left temporal region is larger than your left which is most likely due to a difference in the size of the muscles in that area. This can be approached by two different types of surgeries depending upon which side of your head you like the best. If you prefer the bigger left side, then a temporal implant can be placed from behind the ear under the muscle to make it bigger. If you prefer the right side, then a temporalis muscle reduction would be needed to make that muscle smaller through a vertical incision in the temporal hairline. Or if you don’t like the bulging on either side, then the temporalis muscle could be reduced on both sides.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a revision rhinoplasty, sliding genioplasty and a lip lift. I was born with a unilateral cleft lip and I want my face to be more symmetric. What procedures do you think should be done?I have had one rhinoplasty and I have an L shaped implant. I would like for my nose to be more narrow and symmetrical. With the lip lift I want my lip to be about 15mm or shorter. I have a chin implant, but I think with the genioplasty it will make my chin balance out with the rest of my face.
A: I have done some computer imaging done on your chin, jaw angles, lip and nose. I think it is fairly clear that your chin is fairly short even with the implant in place. This shows that the jaw is rotated up and back (short) and is why the jaw angles are high. A sliding genioplasty (possibly leaving the chin implant in place and moving it with the bone) may be needed to get the 12 to 15mms forward movement you need. Moderate jaw angle implants in the back will help fill give them some more definition. You don’t need your upper lip lifted by 15mms, that would be too much. Something like 5 to 7mms would be more appropriate. The question here is whether it should be done by a subnasal lip lift (lift only the central portion) or a vermilion advancement which moves the whole lip up. (probably better) The nose is challenging because of your very thick skin and the naturally thicker tip skin that many cleft patients have. To make a real difference, the implant ideally needs to be replaced by an L-shaped rib graft so you can get more of a push/lift on the skin and a sharper tip point. The implant just makes it rounder and still short.
The imaging done is to just figure out of these procedures are beneficial. The fine details of it and the degree of changes is an issue up for discussion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting deltoid implants. I am a 36 years old male and I have very short clavicles and a larger than average head to make my shoulders appear even more narrow. I have read a response to a deltoid implant question it made me come up with a few questions.
1. The response stated that the implants can be place in a intramuscular location. Does that apply to an implant for both lateral and posterior deltoid heads? If not, what type of deltoid implant can be placed in the muscle?
2. How much actual width could be added using the largest implant possible without effecting practical functions (such as lifting the arms sideways)? I attached a picture of my narrow shoulder along with a photo-reference of a look I’m going for. I’ve provided of a picture of the look I’m trying to achieve with surgery. The red area is what would be the ideal mass added with an implant. Would this be possible?
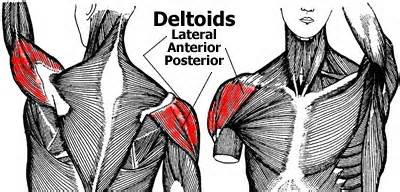 A: When it comes to deltoid implants, an understanding of the anatomy is important when considering implant placement. The deltoid muscle is a broad muscle that creates the rounded contour of the shoulder. While it technically has three sections or muscle bellies (anterior, central and posterior), it is best to surgically think if it as single muscle belly as they are difficult to separate. The muscle is also enveloped by a fascial lining that is most manifest on its outer surface. Thus implants can be placed either submuscular (under the muscle) or subfascial. (above the muscle but under the fascia)
A: When it comes to deltoid implants, an understanding of the anatomy is important when considering implant placement. The deltoid muscle is a broad muscle that creates the rounded contour of the shoulder. While it technically has three sections or muscle bellies (anterior, central and posterior), it is best to surgically think if it as single muscle belly as they are difficult to separate. The muscle is also enveloped by a fascial lining that is most manifest on its outer surface. Thus implants can be placed either submuscular (under the muscle) or subfascial. (above the muscle but under the fascia)
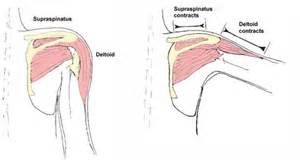 When considering where to place a deltoid implant, one has to take into consideration the movement of the muscle and the arm. As the arm lifts away from the body, the deltoid muscle contracts and becomes shorter. There is the risk, therefore, that a submuscular implant placed directly under the central belly of the muscle could interfere with arm motion. This would be less true for a very small implant or one that is placed closer to the front or back edge of muscle, but this then would not have much of a visible effect as you desire. This makes the subfascial location preferred in most cases.
When considering where to place a deltoid implant, one has to take into consideration the movement of the muscle and the arm. As the arm lifts away from the body, the deltoid muscle contracts and becomes shorter. There is the risk, therefore, that a submuscular implant placed directly under the central belly of the muscle could interfere with arm motion. This would be less true for a very small implant or one that is placed closer to the front or back edge of muscle, but this then would not have much of a visible effect as you desire. This makes the subfascial location preferred in most cases.
Lastly there is the issue of incision location to place a deltoid implant. This is almost always best done on the back side of the arm where it meeds the trunk, keeping any scarring in the least visible location.
Your photo reference indicates a result that probably can not be achieved. Maybe half to three-quarters of that amount of shoulder augmentation is more realistic. Think of adding about 1 to 1.5cms width per side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in depressor septi muscle surgery. When I smile the tip of my nose really gets pulled down. Also my upper lip crunches up and a wrinkle appears across the top of my upper lip. I have read online that this is due to a muscle under the nose and if it is released my nose and lip will look better when I smile. How is this surgery done?
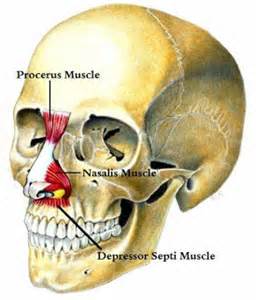 A: The muscle you are referring to is the depressor septi muscle. It is attached from the upper jaw at the base of the nose upwards where it attaches to the nasal septum and the back part of the nasalis muscle. It is this muscle then when overactive pulls the tip of the nose down an pulls up on the upper lip which sort of crunches the nose and lip together. In rhinoplasty this is known as the smiling deformity.
A: The muscle you are referring to is the depressor septi muscle. It is attached from the upper jaw at the base of the nose upwards where it attaches to the nasal septum and the back part of the nasalis muscle. It is this muscle then when overactive pulls the tip of the nose down an pulls up on the upper lip which sort of crunches the nose and lip together. In rhinoplasty this is known as the smiling deformity.
This smiling deformity is often treated at the time of a rhinoplasty or can be done as an isolated procedure. The surgical techniques for treating an overactive depressor septi nasi muscle vary and consist of either an(intranasal resection or an intraoral release/transposition. A recent study has shown that the both techniques produce similar effects in how much they decreased the effects of smiling on the length of the nose, tip projection or upper lip length.
The intranasal approach is historically more common due to the anatomic location of the muscle when doing a closed rhinoplasty. It has a side benefit of decreasing the interalar distance. The intraoral approach has been more recently described undoubtably due to the now widespread use of open rhinoplasty. Coming from below (inside the mouth) allows an actual release and transposition of the paired muscles. This results in an increased fullness to the upper lip afterwards.
Either depressor septi muscle surgery techique can be done under local or IV sedation and has a minimal recovery with some short-term upper lip swelling.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m currently struggling with a flat back of the head and a small head too. Can skull reshaping surgery be done on me to add any implant to mainly the back and top parts of my skull that would give me a decent sized head that is also well rounded ? How effective is this surgical procedure and what are the possible negative effects of any implant on my actual skull?
A: Skull reshaping (augmenting a flat area) can be done to almost any part of the skull and its limits are based on how much the scalp can stretch to accommodate the volume of augmentation. Based on what one’s expectations are, it can be a highly effective procedure. I would have to see some pictures of your head that show the flatness and then do some computer imaging to see if what skull augmentation can do is sufficient. It is always important before surgery to find out if the changes meet a patient’s expectations and to determine how much volume is needed to create that augmented effect.
There are no known long-term effects of the materials used in skull augmentation as it relates to the bone or the overlying scalp tissues. Bone resorption is not known to occur nor is scalp thinning over it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question regarding chin reduction. Could my chin be reduced in height vertically with out having my chin split into pieces? I think that is too much of a risk and to much time to recover from for me. Is there something else you can possibly do like burr it upwards from underneath as well as backwards because I have what I consider to be a pointed chin. I would like to have it rasp to the point it looks wider, flatter and shorter. Is this surgery at all available? How much is allowed to be vertically shaved off before it reaches into the too much taking off zone? I would prefer the incision inside my mouth being as though I’m a person of color but I’m willing to take that risk to have the chin exposed through the under cut to obtain the result I so desperately desire. I’ll just get my scar revised if that’s what it takes.
A: The type of chin reduction you are referring to is common and is known as a submental chin reduction. While burring is used for some minor shaping, more significant reduction is done by a saw blade cut and the edges then burred. This can make a radical reduction in vertical chin length and definitely can take a pointy chin and make it shorter, wider and flatter. With this much vertical chin reduction, the submental approach is best anyway because it allows the excess soft tissue to be removed and tightened as well to prevent a witch’s chin deformity. The amount of bone reduction that can be done is based on the location of the tooth roots and the exit of the mental nerve which is usually above the 10 to 12mm mark from the lower edge of the chin.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a Brazilian Butt Lift. Could this procedure include having liposuction for weight loss reasons as well as butt enlargement? It seems like you get two benefits at once, a bigger butt and dropping your weight at the same time.
A: Every Brazilian Butt Lift requires liposuction to harvest the fat that needs to be transferred by injection into the buttocks. This almost always comes from the abdomen, flanks and waistline and as much fat is taken as possible in most cases. But to call this liposuction harvest, or any liposuction procedure, a weight loss method would not be appropriate. That is not what it accomplishes. Liposuction is a shaping technique but it does not create any substantial or sustained weight loss in most cases.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, i want my forehead made smaller with a shorter hairline. I would like to have a procedure at your facility to have the central frontal bone vault reduced to about 5mm and the glabella the triangular area in between the eyes over the nose and under the brows,I had a interview with a previous surgeon who was actually to far from me to travel but he was saying my scalp is flexible Enough to bring it down to 2 cmd maybe another half once he loosened this area underneath my scalp. I forgot the name of it,do you have any idea what he’s referring to and do you use this same technique?
A: You are referring to a hairline advancement procedure as part of an overall forehead reduction. This requires the scalp be loosed up so it can be brought forward and the hairline lowered. The more natural scalp flexibility one has, the easier and more hairline advancement that can be achieved. This is often done with frontal bone remodeling such as frontal bone reduction and some brow reshaping/contouring. You are correct in assuming that about 5mms of frontal bone can be safely reduced by burring.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young man and I am embarrassed of the shape of my head. My head circumference is about 58 cm which seems to be only about 1-2 cm more than the average but the shape is abnormal- as it gets wider above the ears and temples on both sides. What is very surprising when I clench my jaw both sides of the head gets wider (about 0.5 cm) each side, and when I widely open my mouth both sides of the head get thinner and head looks almost normal. Would you be so kind to answer my questions. Is there any possibility to reshape my head on both sides. If yes what is the potential risk of such surgery- is there any chance to damage my brain, nerves, veins etc and is such surgery a big risk for my health and life? Does the surgery may affect in a bad way circulation of the blood in my head which my cause for example hair loss (it is extremely important for me to protect my hair because that is the only way I can mask shape of the head). What is the recovery time? I train bodybuilding and boxing especially the second one is obviously extremely contact sport- will I be able to continue my two passions and how long after surgery will I be able to come back to training?
A: What you are describing perfectly are thick temporalis muscles which is making a major contribution to the width that you are seeing above your ears and into the temple region. This is evidenced by the widening effect that occurs when you clench your teeth together (temporalis bulging) and why it gets thinner when you open your mouth. (stretches and thins the temporalis muscle) This dynamic head width changes indicate that a temporal reduction (temporalis muscle shortening/relocation procedure) would be very effective. This results in a 5 to 7mm change per side (1.0 to 1.5 cms transversely combined) when these muscles are shortened. In addition a small amount of bone burring can be done at the same time. Not that you know the correct procedure, the answer to your questions are as follows:
1) There is no risk to your brain or any major blood vessels or nerves.
2) There is no risk to your general health. This is an aesthetic operation.
3) This surgery does not affect the circulation to your scalp or head.
4) There is no risk of any hair loss.
5) The recovery is fairly quick, just some swelling on the sides of the head that looks pretty normal in a wee. There are no restrictions after surgery.
6) You could return to contact sports within two weeks after surgery.
7) I will have my assistant Camille pass along the cost of the surgery to you later today.
The biggest issue in performing temporalis reduction surgery is that fine line incisions are needed on the side of your head to perform it. These incisions do not cause any hair loss and I do not shave the incision line to perform them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in breast augmentation surgery but needs some basic recovery questions answered. What is the average time you recommend returning to work? I already have dates that I’m taking off for this year for vacation and other things, so I don’t want to have to take too much time off work. Also, I have an 18 month old, and she is a big girl for her age right now! She is a momma’s girl and is always wanting me to hold her and carry her, so my other concern was being able to lift her and carry her. What are your lifting requirements after surgery?
 A: Returning to work after breast augmentation is highly variable based on what one does, how physical their job is and their own discomfort tolerance. On average, it can be anywhere from 3 to 5 days. I place patients on arm range of motion exercises the night of surgery and the more you move the quicker you will recover. I have no lifting restrictions after surgery and you can lift anything you want without fear of hurting the result. Your body will tell you what you can and cannot do.
A: Returning to work after breast augmentation is highly variable based on what one does, how physical their job is and their own discomfort tolerance. On average, it can be anywhere from 3 to 5 days. I place patients on arm range of motion exercises the night of surgery and the more you move the quicker you will recover. I have no lifting restrictions after surgery and you can lift anything you want without fear of hurting the result. Your body will tell you what you can and cannot do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in deltoid implants. I am a 25 year-old male who has done bodybuilding for the past two years with great results. This is with the exception of my deltoid muscles, which are one of the most important and prominent muscles on a male body. My dad has also weak shoulder muscles so I think it’s genetics.
Now my questions:
1. How are the (silicone ?) implants placed and where exactly, so that the most obvious effect in width is achieved ? Are they placed into the muscles or above, because one should not feel the material when one touch the shoulders if possible.
2. How thick are they? How much shoulder width can be added with the implants ?
3. What are the risks during and after such a surgery?
4. Is the result permanent?
 A: In answer to your questions about deltoid implants:
A: In answer to your questions about deltoid implants:
1) They are silicone implants and are placed either subfascial or intramuscular, depending on which head of the deltoid is being augmented. Of the three heads of the deltoid, the most commonly augmented are the lateral and posterior heads with the implant placed between them. This also creates the greatest amount of width augmentation. It would be helpful to see exactly by pictures which areas of the deltoid you want augmented.
2) Since there are no real deltoid implants commercially made, I use calf implants which have three sizes (volumes 70 to 170ccs) with up to 2 cm of thickness per implant.
3) The risks of surgery are a permanent scar, infection, undercorrection/overcorrection, and implant malposition. (which are the standard risks of any implant-related surgery)
4) The implants will never degrade or breakdown and thus add permanent muscle augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in rhinoplasty surgery. As you can see from my attached pictures, I have a bulbous tip and a deviated septum. I hope to reduce the bulbous tip as well as straighten my nose. Can you please notify me if this can be done? Also from the pictures can you tell me whether or not I have thick nose skin? If I do have thick skin, will I still be able to reduce my bulbous tip and gain a more straighter profile on my nose?
 A: I think you are an excellent candidate for rhinoplasty. You have a wide bulbous tip with played domes of the lower alar cartilages with intervening fat. But it should shape up nicely with an open rhinoplasty where the cartilages can be reshaped and brought together to create a much more narrow tip with more refined definition. I do not see that the thickness of your skin as being a limiting problem for getting a good rhinoplasty result. You have intermediate skin thickness which will shrink nicely when the underlying cartilages are reshaped.
A: I think you are an excellent candidate for rhinoplasty. You have a wide bulbous tip with played domes of the lower alar cartilages with intervening fat. But it should shape up nicely with an open rhinoplasty where the cartilages can be reshaped and brought together to create a much more narrow tip with more refined definition. I do not see that the thickness of your skin as being a limiting problem for getting a good rhinoplasty result. You have intermediate skin thickness which will shrink nicely when the underlying cartilages are reshaped.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in facial asymmetry correction. My face is crooked, particularly my chin and jaw. When I smile my chin pulls to the left and makes the jaw asymmetry look worse as it points to the left. The rest if my face on the left side is also uneven. My left eye and eyebrow are lower and my cheekbone seems smaller. When I look in the mirror I don’t look too bad but it looks much worse obvious in pictures. Can my facial asymmetry be fixed?
A: Like many cases of facial asymmetry, it rarely is just one area of the face. What you are describing is a more complete unilateral or one-sided facial underdevelopment. This is evidenced by a lower eyebrow and eyeball position, a flatter cheek and a shorter jawline distance from chin back to the jaw angles. In essence the vertical length of the face is shorter on your left side than your right. The jaw asymmetry in particular is magnified when you smile as the soft tissue of the chin is pulled back and deviates to the less developed side.
There are a variety of facial asymmetry procedures that can be done from the eyebrow down to the jawline. What you would do depends on how much of the facial asymmetry you want to treat. The chin/jawline often displays the most severe aspects of facial asymmetry and is often the most important area for many patients to correct. This can be treated by a sliding genioplasty to realign the bony chin to the midline. This can be possibly combined with a small jaw angle implant in the back to completely lengthen the entire jawline.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know if the following facial surgery results are possible.
1) With a custom cheek/orbital implant can I augment all of the inferior, lateral, and superior orbital rims along with a small portion of the malar bone?
2) Can off-the-shelf jaw angle implants guarantee that my jaw angles will look more squared/pointed rather than U shaped and heavy?
3) With a rhinoplasty do you believe you can achieve an aesthetically pleasing nose job that keeps a lot of masculinity to my nose. (i.e., keeping a majority of the nasal bone projection and width while still projecting the tip out a slight bit and straightening the nasal bone and cartilage from a frontal view?
A: In answer to your questions:
- While any design can be made for custom cheek and orbital implants, there are limitations to the surgical access to place them. Through a lower eyelid incision, a custom implant can be placed to cover the inferior and lower lateral orbital rim and cheek, but not the upper lateral orbital rim or superior orbital rim. (those require a coronal scalp incision for placement)
- A preformed off-the-shelf jaw angle implant that I commonly use has a more flared and square jaw angle point to it that does not usually cause a rounded jaw angle look. (that patient undoubtably has the traditional rounded style of silicone jaw angle implant that is what is available to most surgeons)
- I believe your thinoplasty goals are achieveable as you have defined them and as we have looked at them with computer imaging in the past.
With that being said, let me make some general statements based on a lot of experience with male facial structural surgery. (of which all your procedures would qualify) It is important to understand that there are no guarantees in surgery. No surgeon can guarantee that any specific outcome will be obtained no matter how much thought goes into it beforehand. Aesthetic surgery involves risk of which the biggest one is less than the desired result. I mention this as you have used the term ‘guaranteed’, this is not an assurance I can give you. In the same vein, it is important to also understand that male facial restructuring is associated with a notoriously high rate of revisional surgery, probably approximating 25% to 33%. This is of paramount note in the young male patient who often is very difficult to please in their search for an optimal result. A good rule of thumb is that the patient will put twice the amount of time assessing their result after surgery than what they spent beforehand…hence leading to such high revisional rates. Slight asymmetries and imperfections are very poorly tolerated in the young male patient.
I mention these issues as you need to factor these considerations also into whether the facial surgeries we have discussed are for you, your expectations and your level of risk tolerance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How much will a rhinoplasty surgery cost me? I have Aetna Insurance and I want to know how much they might cover. By the way I have breathing issues and I went to a doctor and he told me my septum needs correction and my insurance might cover half of the whole surgery price.
A: Let me provide you with some clarification on your nose surgery and a better understanding about the costs of such surgery. The concept the ‘insurance may pay half of the whole cost of the procedure’ is both misinformed and overly simplistic.
What you are seeking is a nose procedure known as a septorhinoplasty. This is a procedure that combines the correction of a functional problem (septum and turbinates) and an aesthetic nasal issue. (rhinoplasty) While they are commonly done together and one does affect the other one, they are viewed economically as two separate issues no matter where you are having the procedure performed. The septum and turbinates are functional airway issues and are often covered by insurance. The rhinoplasty is an aesthetic issue and is never covered by insurance for common aesthetic reasons. Just because the two procedures are done together does not in any way mean that insurance is covering any cost of the rhinoplasty. Those fees must be paid out of pocket and in advance and includes the surgeon’s fee and the operating room and anesthesiologist’s time to do it. When done together a surgeon may choose to lower their professional fee for the rhinoplasty as a courtesy although they are under no obligation to do so.
Thus the only thing that insurance covers has nothing to do with the rhinoplasty. And if you do not do careful financial analysis beforehand (how much is your deductible, what is your percentage of costs beyond a certain dollar amount of what insurance pays), you could easily end up paying more for the whole procedure using insurance than if you paid the entire septorhinoplasty as a complete cosmetic procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in forehead augmentation. I am wondering what all can be done to make my forehead go more up and down rather than how it slants severely back starting immediately above my eyes. After looking up pictures and seeing people with different types of foreheads I think I have found the answer to my problem, or rather, what I would desire to have for myself. I just don’t know how much can actually be done in the present time and how realistic my ideal results are. I would like to add quite a bit to my forehead to make it more vertical instead of so severely slanted and I was wondering if I am desiring something beyond the limits that are currently set? I gave a picture of myself from the side with wet hair to give an accurate shape of my skull as a whole, especially the slanting forehead/top of head, and then another picture of what I am thinking I would like my forehead to look like. I look at pictures of myself (such as this one) and worry if it is only a small amount that can actually be added onto one’s skull, and if I am drastically unrealistic in my hopes, what are the limiting factors? Some of the ones I read about (like the amount the skin will stretch on one’s head) seem like the major one.
 A: What you are seeking is a commonly performed aesthetic craniofacial procedure, forehead augmentation. This is done for a variety of forehead shape concerns, one of which is to change a sloping backward slanting forehead to a more vertical one. While the limiting factor is how much the scalp and forehead skin can stretch, the result you are desiring to achieve is largely very realistic and within the ability of the scalp to accommodate a greater volume and convexity underneath it.
A: What you are seeking is a commonly performed aesthetic craniofacial procedure, forehead augmentation. This is done for a variety of forehead shape concerns, one of which is to change a sloping backward slanting forehead to a more vertical one. While the limiting factor is how much the scalp and forehead skin can stretch, the result you are desiring to achieve is largely very realistic and within the ability of the scalp to accommodate a greater volume and convexity underneath it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had eyebrow hair transplants 12 days ago. Anyway, it seems like the transplanted hairs have been falling out these past few days. There wasn’t much crusting or scabbing, and I have not noticed any blood on my eyebrows. I’ve spoken with my surgeon who has told me that it’s normal for the transplanted hairs to fall out. But I’m still a little concerned, which is why I would like your opinion as to whether this shedding is normal? If so, why do these transplanted hairs fall out and not continue growing?
A: The basic concept of any hair transplantation procedure, including eyebrow hair transplants, is to do follicular (hair bulb) transfer and implantation. The hair shaft is merely a handle by which to do that. It provides a convenient means to move the hair follicle into a new site. The shock of the transplantation procedure causes the shedding of the dead hair shaft 10 to 14 days after the procedure and is both expected and normal. The transferred hair bulbs are intact under the skin and new hair will not be seen until grows out from the follicle. Given the rate of hair growth, it will take months to see new hair emerge and a full six months to have the desires hair length that you seek.
Dr. Barry Eppley
Indianapolis, Indiana