Your Questions
Your Questions
Q: Dr. Eppley, I had a chin implant revision surgery 6 months ago. During the recovery, the nerve reaction on the right side is slightly weaker, causes no problem. I believe there should not be any nerve injury during the procedure.
However, intermittent numbness and pain become more severe in the latest month. The implant was perfectly screwed and didn’t shift. I found one possible reason is that one side of the incision (denoted in green color in the attached photo) is close to the mental foramen. As the underlying scar grows, it may compress the mental nerve, which causes the pain and numbness (sometimes an itchy feeling). These feelings become stronger if I pressed the skin above the mental foramen.
Could this develop into chronic pain? Is that possible to deal with this by nerve decompression surgery someday later?
I’m looking forward to your reply!
A:It would be impossible to predict how the affected mental nerve may react as its distances itself from the date of the surgery. But at 6 months out from the surgery it would seem not very likely to develop into chronic pain if it has not done so already since the scar tissue has fully formed at this point.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Hello, a couple of questions. I’m planning on getting perioral mound liposuction, mouth widening surgery, a dermal fat graft into my labiomental crease, and maybe a buccinator myectomy (if needed) I’ve already had around 85% of my buccal fat removed so I dont need anymore removed. A couple questions I workout so I fluctuate in weight by roughly 20 pounds depending if I’m bulking or cutting. I gain slowly (roughly half a pound a week) I was curious would gaining/losing weight effect the perioral mound liposuction? As in would it come back if I gained a bit of weight? As well as would the fat graft in my labiomental crease get smaller/bigger if I gain/lose weight? Also, I’m going to he getting a genioplasty at some point mostly vertical movement and maybe 2 to 3mm forward movement would it be best too get the fat graft in the labiomental crease after that procedure? Also how much would this is all cost? Sorry for so many questions!
A: Thank you for your inquiry. In answer to your questions:
1) Since the perioral mound areas is subcutaneous fat and not really a typical fat depot area, it should not be affected by the weight gain that you have described.
2) The injection fat graft is a more relevant one for the concern about it changing with weight gain or weight loss particularly if the abdomen is the donor site. Which is why the inner thigh should be used as this is not a typical fat depot site.
3) Whether you do a labiomental fat graft during or after a primarily vertical lengthening genioplasty is irrelevant from a technical standpoint. It is more relevant from the effects of the genioplasty as vertical lengthening genioplasties tend to lessen the natural depth of the labiomental sulcus. So it is possible you may not need anything done to the labiomental sulcus based on the effects of the lengthening genioplasty. This would be the argument to wait and see.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, 1. How would my face look smiling? That was something I forgot to ask during our 10 minute consultation and something the retouched images from your initial e-mail reply didn’t show. Is there any way to predict, or responsibly hypothesize what I’ll look like smiling after implants?
2. This is probably a silly question, but you said custom implant recipients tend to be more prone to wanting revisions. Do we live in such a world that if I’m not satisfied with the end results, costs are waived for revisions or implant removal? If so, what waived costs or discounts are offered?
3. I like to think catastrophically sometimes to try to be as prepared as possible, so bear with me on these next few which get a little dark. What happens if I’m in an accident after surgery and break bones where I have implants? Would I need to have them removed and have you to re-do them after the bone was mended?Are there activities I’ll need to avoid to ensure the implants don’t shift or break?
4. This one gets a little darker so I apologize in advance and hope you see my intent comes from a good place and the desired to think ahead and be prepared: Okay, let’s say we’re halfway through implant design or maybe I’ve gotten the implants and I’m happy with them but something happens and they need to be repaired but you’ve either retired or gotten struck by lightning or, for whatever reason, just aren’t available. Do you have a rolodex of surgeons you trust to do these surgeries just as well or better than you? If so, who are they? Even though it wouldn’t be particularly self-serving, is there anyone who you feel could do these implants just as well or better than you?
Thank you so much for taking the time to help me learn as much as possible before I start this journey with you and your team! I really appreciate it.
A: In answer to your custom facial implant questions:
1) I have not yet had any issues in facial animation with infraorbital-malar (IOM) or jawline implants. The only potential issue with smiling would be with the IOM implants. But because they are in higher position than standard cheek implants they are more out of the way when the cheek tissues bunch up with smiling.
2) This is a very important question and I would ask my staff about that very issue for which there is a revisional surgery policy. It spells out the risks and the patient obligations should that occur. Such revisions are not what I want but when you put implants anywhere the body that risk is very real and not insignificant.
3) The issue of trauma to the implanted site is a common question. The reality is that it has never yet occurred or one in which no patient has ever had an actual scenario as you have described that has been relayed to me. From a trauma standpoint custom IOM and jawline implants are like putting bumpers on the bones. It would be very hard (albeit not impossible) to fracture the bones underneath them. In essence they are like shock absorbers.
4) Admittedly a bit darker but not a completely impractical question. There are other surgeons in the US who do perform these surgeries. It is a very small number but they exist. Most are not going to have my experience in designing or perform these surgeries. I can not tell you whether any of them are poorer, as good or better than me at it, regardless of their experience since there is no assessment method to make that comparison.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was curious generally speaking what percentage of people have the type of skull shape which would accommodate a 1 inch implant for cosmetic stature gain in an aesthetically pleasing manner, and what that ideal skull shape is.
To be candid I was surprised to find that this is even done, because my first instinct was to assume that such an implant would look unnatural, like something from Star Trek or Coneheads or something. Is it the case that average skull height is variable enough throughout the population that such a change is easily concealable? Does the size of one’s forehead or their hair type or any other factors significantly affect one’s suitability for the height increasing procedure with respect to concealment?
I feel like there are two bifurcated philosophical schools when it comes to cosmetic surgery patients – those who don’t mind a slightly (or significantly) unnatural look, which perhaps represents the vanguard of cosmetic augmentation, and those who want as close to a natural appearance as humanly possible. I would definitely place myself in the latter group and wouldn’t want anyone to wonder “what’s up with your head”?
I was also curious what your opinion is regarding surgery on the scalp for patients with a history of keloids developing in common keloid forming areas. For example I have several keloids in my sternum area as well as my right shoulder, which apparently are two common areas, however I thankfully do not have any on my face. Could a small “test incision” be done on the scalp to make sure the area responds to trauma well before an actual procedure?
Thank you for reading
A: Thank you for your inquiry. The key to all skull implants is that their design has to look like they belong there as a natural extension of the convex shape of the skull. As a result they cover a much larger surface area than one would initially think to do so. And usually most patient’s way over estimate the thickness of the augmentation they need because they focus on a simple linear measurement rather than the volumetric effect of large surface area coverage. The limiting factor in any skull augmentation is the ability of the scalp to stretch to accommodate what is placed underneath it. In general most people can tolerate a 100 to 150cc implant without a first stage scalp expansion.
When it comes to what patients want, very few patients want anything but a natural looking result. One’s interpretation of what looks natural will vary as what one person deems natural may be unnatural to another. But in skull augmentation everyone wants a natural head shape result.
Trying to correlate how a scar looks on the body to what may occur on the face or scalp is not comparable. Most likely you have hypertrophic scars, not true keloids, which are common in many people particularly in the sternum (which is a terrible area for a scar) as well as the shoulder which is a high motion area with thick reactive skin. Making a test incision in the scalp is not replicative of the situation when an implant is placed underneath it with the incision subsequently closed under tension.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thank you for your reply to my son regarding further head width reduction treatment He is extremely happy that you are able to carryout further treatments to enable him to look and feel better about himself and therefore more confident.
There are a few areas I am unsure about and so would like clarification on please. Previously you mentioned two options 1. Botox and 2. electrocautery surgery.The advisory treatment offered to him is ‘Temporal Reduction Bilateral, Anterior, is this the electrocautery surgery?
Is this the preferred treatment for Nic as opposed to Botox injections? I assume this option has been chosen as he would prefer a more permanent result.
As he has already had posterior temporal reduction and now planning anterior surgery will there be any possible adverse long-term side effects?
How long will the immediate recovery period be before he will be able to leave your care and carry on with his journey?
I look forward to hearing from you
A: While Botox will likely create improvement in the fullness of the anterior temporal muscle, it will not be permanent. The thermal treatment of the muscle results in eventual partial muscle shrinking/atrophy which is permanent. I have done such anterior reductions on patients who have had prior posterior temporal muscle removals and there have been mo adverse functional effects from doing so. Like the last surgery he will be able head home on a similar time frame. While the immediate postoperative swelling is very similar the effects of muscle atrophy take much longer to see than muscle removal. The muscle shrinks down over a period of months after the surgery so getting to the final outcome requires more patience.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve wanted to get skull augmentation surgery done for a while, probably 3 procedures if not all together, the frontal, temporal and back of the head procedures and i was wondering what the cost would be. I don’t want an extreme change but to make my forehead a bit more round in shape and more prominent i guess and possibly near my brow bones or cheekbones too if possible. I was wondering if they’d have to be done all at once or not, what the cost would be etc.
A: Thank you for your inquiry. You are referring to skull augmentation in which you reference the forehead, temporal and back. Since the scalp will only permit so much augmentation to occur (unless one does a first stage scalp expansion), it is important to prioritize the areas of concern. Based on your description of your forehead /temporal objectives I would assume that is a priority area as it is also the most visible. That would be done as a combined implant in one surgery.
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley, I would like a forehead reduction procedure. My questions are:
1) is it possible to reduce the advance and the width of my forehead?
2) what is the waiting time to be operated?
3) how long do i have to stay during the operation in the USA?
I also know that a scar is visible after the operation.I was thinking of doing a FUE hair transplant procedure to hide this one and advance my front line.
Do you think this is possible?
Best regards.
A: Thank you for your inquiry and sending your pictures to which I can make the following comments:
1) It is not a question as to whether your bony forehead can be reduced in both width and forward projection…but by how much. Bony foreheads can be reduced by removing the outer cortical layer of the skull down to the diploic space. How thick that layer is is what determines the magnitude of change. A preoperative CT is needed to make that determination.
2) if you want to undergo a hairline advancement this is best done at the time of the forehead reduction as the best place to put the incision is at the frontal hairline. That would achieve two goals at the same time.
3) You wouldn’t do a hairline advancement and FUE hair transplants at the same time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have prominent temporals major muscles which are very strong. It bothers me in two ways:
1) I get incredible tension headaches from clenching in the night and even eating chewy food.
2) I dislike the look.
I’ve had three Botox courses into the muscle to try and reduce it and whilst it provides some temporary relief it’s short lived.
I’m interested in the surgery and wanted to understand more about it.
Thanks in advance.
A: Thank you for your inquiry and detailing your temporal muscle concerns. The critical question is which part of the temporal muscle is involved. (posterior, anterior to both) That knowledge determines the extent of the surgery and time/cost to do so. Please send some pictures that show the event/location of your temporal muscle hypertrophy. Based on your description I suspect it is a combination of both posterior and anterior area temporal reductions which, although can be surgically treated at the same time, are done by different methods.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Im wondering on the cost of getting bone cement in my forehead to fill in the sunken in curves for a beautifully shaped forehead. Thank you!
A: Thank you for your inquiry. There are three materials in which to perform forehead augmentation including two types of bone cements (PMMA and hydroxyapatite) and a custom forehead implant. With each technique comes different costs and potential outcomes. You mentioned ‘bone cement’ but I don’t know if that is what you are interested in exclusively or that is the only technique in which you are familiar. Custom forehead implants always produce the best aesthetic results and are done through the smallest scalp incision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley: I have a Medpor chin implant. At three months post-op, I went to dentist for regular cleaning. However, my soft tissues are not fully healed with the Medpor chin implant at that time, and when the dentist presses my lips, I felt a sharp pain in my chin. I lost the sensation of my chin immediately.
Now it’s about 4 month after the dentist visit, one side of my lip still feel kind of numbness. I guess my mental nerves are over-stretched by the dentist. Will the sensation of lip gets back to normal? How long will it take. Is it possible to have a permanent mental nerve damage by regular dental cleaning? Thanks a lot!
A: I do not think it is possible that permanent nerve damage to a chin implant can occur from a dental cleaning.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about a breast augmentation and possible lift. I have sagging due to two children breastfeeding. I was told having a lift would make the sagging worse from a previous surgeon. How can we ensure this would not happen if I only did the augmentation?
A: Thank you for your inquiry. I have never heard of or can understand how a lift could make sagging worse if done with breast implants. It is the opposite which is certainly true….in the presence of sagging (nipples below the inframammary fold) the use of breast implants alone can make sagging worse. Perhaps you have pseudoptosis (nipples at the level of the inframammary fold but with breast tissue hanging below) in which breast implants alone would be adequate.
As you can see the type of breast sagging determines where a lift is needed with breast implants.
To determine what this means for you I would need to see some pictures of your breasts from the front and side for a more informed recommendation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is tip reduction possible in this very thick skinned big bulbous nose tip?
A: Thank you for your inquiry and sending your picture. The question is not whether tip reduction rhinoplasty surgery can be done in your nose but whether the amount of improvement obtained would justify the effort. That answer would never really be known until the surgery was done and the outcome eventually seen. But the way to choose whether surgery is worth it up front, in a procedure where the outcome can not be accurately predicted beforehand, is the attitude one walks into surgery taking. If one says to themselves any improvement is better than what I have have…then surgery will be worth it But if one has a very specific goal (e.g., 50% reduction and a substantially thinner nose) and one feels surgery would not be worth it unless that was obtained than one shouldn’t do it.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, I came across an article written by you about fat grafting to the chin for a deep labiomental fold. It is something I struggle with and was hoping to get more information about the procedure. Thank you.
A: Thank you for your inquiry and sending your pictures. You have a moderately deep labiomental fold for which fat grafting would be an appropriate choice to treat it. The debate is whether that is injectable fat grafting or the intraoral open placement of a dermal-fat graft. That question is best answered by how the fold responds to injectable fillers. If injectable fillers pushes it out nicely then fat injections would work. If it doesn’t push it out well due to tissue adherence then the release and open placement of a solid fat graft is best.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am unsatisfied with how high my eyebrows are, and I feel like they make me look slightly feminine. When I furrow my eyebrows, they move downwards, closer towards my eyes, and become straighter, which gives me a more masculine appearance, as you will see in the image I’ve attached. Additionally, my eyes become slightly hooded as well, as the excess skin over my eyelids moves down. Overall, I am extremely pleased with this appearance, however, it is inconvenient for me to go around with my eyebrows constantly furrowed!
That being said, I am wondering if there exists any procedure(s) (surgical or nonsurgical) that will give me the look I desire when I furrow my brow. I am currently considering a reverse brow lift, but I am unsure if it will produce the result I desire. Botox is also an option, but I am uncertain how far my brow will be able to move down. Will injections give me the look I desire?
Also, please let me know if there are any other procedures I could undergo to achieve the desired look, no matter how expensive or unique.
Thank you in advance!
A :The lowering of the eyebrows is a difficult tissue change to accomplish in a young person because of their tight forehead skin. Enough Botox may have a temporary effect (3 months) but that is obviously not a long term solution. A reverse browlift is not going to work for the reasons previously described. (tissue tightness) The only way to lower the brows is with a supplemented reverse browlift using forehead tissue expansion. You must create the tissue stretch closest to where you want the effect. This is done with a specially shaped type of tissue expander
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about testicle enlargement. I have normally functioning albeit small testicles. I am curious if you have noticed any atrophy of the existing testicles with the implants? Any problems with sperm count after the surgery?
Finally, would you let me know if you have any pictures of the implants and the cost of the procedure?
Thanks.
A: Thank you for your inquiry. In answer to your testicle implants questions:
1) I can not speak to whether implants have any adverse effects on the existing testicles as no such tests have ever been done (e.g., sperm counts) nor has any patient ever mentioned any issues. I would assume it does not since the vascular supply to the existing testicles remains intact. Most of the men who get this procedure are often older where any concerns about sperm counts are largely irrelevant.
2) To see pictures of the implants I would go to www.exploreplasticsurgery.com and search under Testicle Implants where you will find many articles with implant pictures on this subject.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Are you put to sleep while the occipital bone reduction procedure is being done? & how long do you have to be out of work after the procedure is done.
A: Thank you for your inquiry. In answer to your occipital skull reduction questions:
1) You are put to sleep for almost all forms of skull reshaping surgery. These are not procedures to be done under local anesthesia or IV sedation.
2) Physical recovery is very quick from skull eduction surgery and you would be out of work at most one week after the surgery. The actual results, however, takes much longer to finally see.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young African-American. man. I am looking into augmentation rhinoplasty. The concerns I have with my nose are its wide nostrils, bulbous tip, and low bridge, in order from most distressing to least. The internal structure of my nose is in great condition. I have no trouble breathing. My septum is in pristine shape, full of cartilage with no deviation. Cartilage grafting and an alar base reduction seem to be the best course of action. I am looking for a surgeon who can reasonably achieve what I’m looking for and do it affordably. I’ve attached pictures of myself below. I am asking that you provide me with a quote for the rhinoplasty procedure. I completely understand that without a physical examination you cannot give an exact quote, but I’m certain that the doctor or director can give a reasonable price range based on the information I have provided.
A:Thank you for your inquiry and sending your pictures. You have clearly outlined your rhinoplasty needs/goals of which augmentations of the dorsum, tip narrowing and elevation and nostril reduction are the cornerstones of it. The key issue in any augmentation rhinoplasty is what type of material does one want to use to do for the building and how much of a build does the patient want or need. For the tip of the nose septal cartilage is always used for the columellar strut and onlay tip grafting, there is not any debate at this augmentation area. It is the bridge (dorsum) where the discussion lies.
The bridge can be built up using three types of materials, septal and rib cartilage and an implant. Each has their own advantages and disadvantages and the results are not always similar. When using septal grafts this supply is limited and given that some of that is used for the tip there is not as much available for the bridge as one would think. Thus using septal cartilage for the bridge will only create 2mms or so of augmentation. (see attached 1st rhinoplasty prediction) More substantial cartilage augmentations require rib grating where the amount of buildup is more substantial because there is more material to use. (see 2nd rhinoplasty prediction) Thirdly the use of an implant (hand carved ePTFE not silicone) works really well in isolated bridge augmentations and produces maximal augmentation results like rib grafts but without the donor site and less operative time to perform.
Knowing how you want to do your augmentation rhinoplasty will allow a proper cost of surgery to be provided.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want my forehead lowering, my chin is too small and my forehead is big and it is asymmetrical.
A: Thank you for your inquiry and sending your pictures. The forehead lowering appears straightforward and the only issue there is how much hairline lowering you think you need and whether it can be achieved. The way to answer that question is for you to draw on yourself the ideal hairline position and take a picture of it so I can determine what is possible. For the chin the debate is not whether you would benefit by increased horizontal projection but how best to address the chin/jawline asymmetry for which there are two options. A sliding genioplasty is the historic approach as it can bring the chin forward as well as slide it over to the midline. While that is good from the centering of the midline chin point, that does not really address the jawline behind it and leaves bony stepoffs along the jawline as well. Ideally a custom chin implant addresses all aesthetic needs more completely but costs more to do so and involves an implant. In short both methods are valid approaches but each has their unique set of disadvantages.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am really interested in getting a custom jaw implant and sliding genioplasty (don’t know if I am a right candidate for genioplasty or chin implant, please see my pics). I want to get a shape like Brad Pitt. I know I won’t look exactly like him after this procedure but I wanted to give you an idea of what kind of shape I’m looking for. Also, in my picture you can clearly see my forehead is gone in a little bit. So please advice me on that, if I should get a implant for that. Lastly, do I need cheekbone implant?
A: Thanks for sending your pictures in this additional email. I have done some imaging for you looking at jawline augmentation alone as well as with infraornital-malar and forehead augmentations from which I can make the following comments:
1) I believe you are correct in that a bony genioplasty with custom jawline implants is best for you because you have a vertically short chin which needs an 8 to 10mm lengthening. This is best done with an opening wedge intraoral bony genioplasty to which the jawline behind is matched with custom implants. When you get into vertical chin lengthening at 8mms and above the soft tissue chin pad will not stretch over an implant. When you drop down the bone, however, the soft tissue chin pad comes with it. That will also help the depth of your labiomental fold as the soft tissue is stretched/lengthened down as well.
2) I added on infraorbital-forehead augmentations in a second set of imaging with the jaw augmentation predictions. As would be expected these help your overall face as they continue the reshaping effect to the next two levels above the jawline. (jaw-cheek-forehead facial architecture) Whether you do one, two for all three levels in a single surgery is a personal choice.
3) Imaging is provided and it is important to understand its role in facial reshaping surgery. These are examples of one degree of change for any facial structure altered, this does not mean it is the only type of change possible. Imaging creates a dialogue to help better determine what degree of facial change a patient is seeking.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if you would have time to pop a quick email response back to me with some advice and quotes. I have a heavy lower 3rd of my face. I have seen a variety of ways to address this (jaw reduction, buccal fat removal, perioral mound lipo, facelift) and I’m wondering what he would recommend. My goal is to have cheeks that are round and full in the front and a vline, slimmer jaw shape that is not so bottom heavy and long. When I lift the tissue around my jaw towards my cheeks/ears it helps me get more of the look I desire. I will attach some photos! Thank you.
A: Thank you for your inquiry, sending your pictures and detailing your facial concerns/objectives. Your facial reshaping question is a common one to which I can make the following comments:
1) While pushing/pulling the tissues back along your jawline in front of the ear creates the desired lower facial reshaping change, that does not mean that a lower facelift will end up with the same result in a young person without significant tissue laxity. In other words, the ‘facelift’ maneuver over estimates the effect it can create and sustain. And this should not in a young person be the go to first procedure for lower facial slimming. That doesn’t mean it should never be done but it should be either the procedure of last resort or a complementary procedure to others being done
2) For you the procedures of bony jaw angle reduction (width only), masseter muscle reduction and perioral/lower facial liposuction would be the foundational procedures.
3) You have good cheekbone structure but to enhance that further buccal lipectomies with anterior cheek augmentation using either the buccal fat as pedicled transfers or converted to fat injections or a small malar shell implant would be the approaches to achieve cheeks that are rounder and fuller.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, I am a former patient of yours when you performed a breast augmentation/breast lift with saline implants in 2004.
I have experienced some changes to my breasts in recent months. I have lost fullness at the top of both breasts and can now feel both implants along the bottom folds and lower sides of both breasts. Both breasts are still symmetrical and of equal size and fullness. The changes do not appear to be a result of deflating.
I can only assume that I need to consider replacing my implants.
I do not anticipate the need for additional lift or procedures as my nipples are in place.
I would like to inquiry about the general cost associated for a replacement breast implant surgery to determine if I want to move forward with a consultation at this time.
Any information would be appreciated.
A: Good to hear from you after all these years. With 16 years of service out of your indwelling saline breast implants that is getting them into more ‘senior citizen’ range as very few saline implants make it to 20 years without deflating. Replacing them with highly cohesive silicone implants will restore upper pole fullness as well as improve much of their wrinkling. My assistant Camille will pass along the cost of the surgery as part of this email.
The good news is that, unlike the first time which involved making the tissue pockets, they are already established so you should have minimal to zero pain with their replacements.
Dr. Barry Eppley
Indianapolis,Indiana
Q: Dr. Eppley, I’m a young women and very interesting in doing a few procedures with you. I’m going for a face with more “modelesque” features with the appearance of more prominent bone structure. I don’t want to look too masculine or sharp. I have a decent bone structure but there’s still baby fat in my face which I believe covers it, it’d like it to be stronger and keep my youthful look and don’t want to remove any fat if I don’t have to.
I’m looking to get a custom zygomatic-orbital rim implant, custom jaw angle implants, and a sliding genioplasty with you. If fat removal is necessary than I may consider that too depending on your inputs. Roughly, how much would this cost?
I have a mild recessed chin. I want a more defined bone structure so I can look more sultry and modelesque. I’ve provided photos of women with such bone structure. I’m not looking to replicate them , simply get a result with a likeness to them.
A: Thank you for your inquiry and sending your pictures to which I can make the following comments:
1) The jawlines you are showing can only be achieved by a custom jawline implant. Those are linear and connected jawlines between the chin and jaw angles. That can not be achieved by separate procedures on the chin and jaw angles even if the jaw angles were custom made. Economically it makes more sense to have one custom implant made that can do the entire jawline.
2) Since I do not have a full view of your face it is hard to say what type of ‘cheek’ implant you need. Most likely you may mean a cheek-arch style implant rather than an infraorbital-cheek implant as the goal is to get that linear higher cheekbone look.
3) There may be a role for a buccal lipectomy to help the desired cheek look.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a young male and I’ve been dealing with severe anxiety since my teenage years due to the size of my skull, which I find too small. Hitherto, I thought there would be no way to fix that, but I’ve learned about your work, so I browsed your gallery and what I saw was absolutely amazing. Basically, the idea would be to lightly increase the width of my head and to give some volume at the back of it. I want you to ask you several questions :
1) Can the implant be kept for a lifetime ?
2) What is the look of a typical scar after healing ? (scarring is not so much an issue, and compared to how the skull enlargement procedure would benefit me, I wouldn’t care so much)
3) Is there a risk for the implant to “slide” ? I suppose it is attached to the skull solidly, so no, but still unsure.
4)What would be the typical cost for such an operation, including the price of an implant ? I guess this may vary drastically upon the complexity/nbr of implant and the difficulty of the operation.
5) Silly question but : is the thickness of the implant a modifiable parameter ? If I want quite a thin one for instance ?
Thank you for your time, looking forward for an answer ! Hope you have a great week and congratulations for your work.
Best regards,
A: Thank you for your inquiry and detailing your head shape concerns and objectives. In answer to your skull augmentation questions:
1) Custom skull implants are made of solid silicone that will last a lifetime and never need to be replaced due to material degradation or breakdown.
2) Custom skull implants are typically placed through remarkably small incisions given the size of the implants that heal remarkably well. Many people only envision the traditional use of full coronal incisions that are used in craniofacal surgery but that type of scalp incision is almost never used in aesthetic skull reshaping surgery.
3) Custom skull implants do not become displaced or ever slide around. They are firmly fixed to the bone and/or fascia and actually get tissue ingrowth through them.
4) My assistant Camille will pass along the general cost of such surgery.
5) The design (footprint and dimensions) of custom skull implants is done in any way that achieves the patient’s aesthetic goal, That is why they are custom designed and made individually for each patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young woman who has an abnormally narrow face / skull / forehead. My skull is considerably narrow while the width of my forehead is abnormally small which makes my forehead with a bulging deformation. The more I get older and the more it becomes unbearable. I wish I could find a solution in order to make this face more normal, balanced and harmonious. I recently discovered that skull implants I exists. Until this day I did not know. I would hope to widen my forehead at the level of the sides of my forehead and as well as my head size. I understand that it is not necessary to carry out a heavy operation because I think that it is just an insertion of materials on the surface since it is not even a question of touching the cranial box but simply of inserting materials under the skin? What is it possible to do dear doctor?
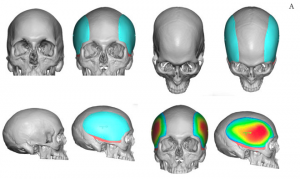 A: Thank you for your inquiry and sending all of your morphed pictures. Fundamentally your suppositions are correct in that there are custom head widening implants made just for the very purpose you described and have imaged on yourself…a complete head widening effect from the forehead back along the sides of the head.(see attached implant designs) You are also correct in that their placement is under the scalp on the bone in the forehead and on top of the temporalis muscle on the side of the head.The width increase you are demonstrating is probably no more than 5 or 6mms at the widest part above the ear.
A: Thank you for your inquiry and sending all of your morphed pictures. Fundamentally your suppositions are correct in that there are custom head widening implants made just for the very purpose you described and have imaged on yourself…a complete head widening effect from the forehead back along the sides of the head.(see attached implant designs) You are also correct in that their placement is under the scalp on the bone in the forehead and on top of the temporalis muscle on the side of the head.The width increase you are demonstrating is probably no more than 5 or 6mms at the widest part above the ear.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for a dramatic chin augmentation as I have a really short chin.
A: Thank you for your inquiry and sending your pictures. A significant chin augmentation is generally anything north of 10 to 12mms. Your chin deficiency is probably in the range of 15mms. Such can augmentation are best done by a composite approach combining a sliding genioplasty with a chin implant overlay were the bone movement serves as the majority of the movement and the implant overlay adds to it but equally importantly keeps the chin from becoming too tapered and narrowed due to the bone movement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My lower lip sags since I had a silicone chin implant removed over 5 years ago. I only had it in for 9 months. Since then I have trouble making my lips meet and my mouth is usually gaping open. I went to a maxillofacial surgeon a couple years ago who said he thought it was caused by scar tissue in my mouth from where the implant was removed and there was nothing that could be done. Could it also be caused by my mentalis muscle?
A: Thank you for your inquiry and detailing your concerns. Chin soft tissue sag and/or lower lip incompetence is not uncommon after a chin implant is removed albeit for just a few weeks or nine months after implantation. Once the soft tissues are surgically elevated off of the bone and then the soft tissue support is removed (implant) this can happen. The key question is whether intraoral soft tissue suspension can be effective. It can be but it is more effective if some type of soft tissue support is placed underneath it such as a very thin small piece of material (e.g., medpor sheet) to which the soft tissue pad can stick to so that it doesn’t exclusively rely on the muscle suspension for uplifted success.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I hope this finds you safe and well. I’m a young man who would like to look the best I possibly can and have long considered cosmetic surgery but never quite pulled the trigger. Part of it is that I’m fairly confident in my appearance to start and have worried that augmentations could end up making things worse instead of better. Still, I find myself carefully adjusting my face by how I hold my jaw or flex my cheek muscles under my eyes or pout my upper lip, not just in photos but almost constantly when I’m with other people.
In wanting to look like the best possible version of myself, I’d love your professional input, but I do have some ideas. I’ve attached 6 photos of my face in sunlight (no makeup or filters) relaxed and not biting down on my cheeks to help show you what I think could be improved. My main concern areas are the under-eyes/tear-troughs and my jawline/chin as well as balancing some facial discrepancies (mostly in these areas). I tend to trust all that Golden Phi Ratio stuff, and I’m assuming that helps guide your work as well, so the closer I can get to that, the better. I’ve considered fillers, but I think I thought implants might be more effective (and cost-effective) for what I’m looking for. Hopefully you appreciate thoroughness and this isn’t overkill, but I figured it would be most helpful for me to split comments up photo by photo since they’re all different angles.
Photo 1: Front-facing. You can see there isn’t a lot of structure beneath the eyes making me appear a little hollow and tired. This is worse on my right side with my right eye appearing to droop a bit, especially the lower lid and outer corner. My lower eyes/eyelid also have a mild bulgy kind of appearance I’d like to mitigate. The midface is somewhat flat whereas I’d prefer I looked more awake, even, and contoured. The tear troughs are rather prominent as well. You can see my left cheekbone has more structural integrity than my right; the entire right side of my face is just a little droopier overall, even that corner of my mouth is a bit lower. Also, while not super prominent here, my nasolabial folds are getting a little deep. To address all of this, I’m sure you have recommendations, but my assumptions would be a custom jawline/chin implant, cheek/orbital rim implants, and philtrum shortening/upper lip lift possibly with some filler. The overall goal being a more balanced/movie star/contoured appearance. I do definitely want to be wary of any jaw or cheekbone implants being too wide since I already have relatively close-set eyes.
Photo 2 is a three quarter profile turned to my right. You can see my right cheekbone is a little less developed than my right and my left jawline isn’t quite as strong as my right (see Photo 4), it even manages to make my chin look slightly weaker from this angle. Again, the under-eye/orbital rim/upper cheek area could be built up more and the philtrum area is a little long.
Photo 3 is the left side profile. Another view of how the jaw could be strengthen and cheekbone/under-eye area given more structure.
Photo 4 is the three quarter profile turned to my left. My face is more attractive from this angle. You can see the left cheekbone and right jawline are sharper, Even so, you can see the way the lack of structure is worse beneath my right eye and how, really, all myall my features get more delicate beneath my brow bone. It suits my nose well, but everything else could be strengthened a bit so long as we keep everything well-proportioned.
Photo 5 is the right side profile – not bad, same notes really, jaw and cheek/under-eye could be stronger.
Thanks for taking the time to read this novel. I look forward to connecting, hearing your perspective, and learning what’s possible!
A: Thank you for your inquiry, sending all of your pictures and detailing your facial concerns and objectives:
1) Your facial assessment is correct in that you have facial imbalances manifest as a negative orbital vector, under eye hollows with associated flatter anterior cheeks and a deep labiomental sulcus which is associated with primarily a vertically short lower chin/jawline. Many of these facial structural symptoms people try to compensate for by facial posturing (holding the lower jaw open to elongate the face, sucking in the soft tissue below the cheeks to make the cheeks appear more evident) just as you describe yourself doing. (see attached facial vectors of deficiency)
2) These facial symptoms fundamentally come down to facial skeletal deficiencies of infraorbital-malar hypoplasia and a vertically short lower jaw.
3) What you have is very common in my experience and is treated by custom infraorbital-malar and jawline implants +/- midface defatting. (see attached imaging as one version of change)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Do you perform orthognathic surgery? I came across some very interesting comments from you on Realself posts. I started my orthodontic treatment over a year ag.. I refused to accept extractions and accepted IPR instead. Two orthognathic surgeons that I was recommended to by my orthodontist saw my case and called it “common” and “nothing to worry about.” They suggested a sliding genioplasty instead to aid with my lip incompetence, and assured me that jaw surgery was unnecessary. I accepted. I ended up undergoing two sliding genioplasties in one month. This is because the first time turned out to be a total mess. My chin had been advanced too much (8 mm), and that was after I had refused a 10mm advancement. The second one turned out better (5 mm), but now I have ended up with chin ptosis. My lip incompetence is worse than ever before. I drool without realizing it and have trouble sleeping at night. Recently I’ve been waking up at night, gasping for air. After paying closer attention to my x-rays, I noticed my airway is very narrow. Shouldn’t that have been taken into consideration? Wouldn’t jaw surgery help with my narrow airway? I had no idea what to look for before, but after doing research, I learned that a narrow airway may lead to sleep apnea. I fear that I may have sleep apnea. A part of me feels like I’ve been neglected multiple times by several professionals. I found hope in your responses to several posts on Realself regarding v-y lip advancement, mentalis resuspension, and jaw surgery. I hope you can help me. Thank you for your time. I appreciate it so much.
A: Thank you for your inquiry, sending your pictures and detailing your concerns to which I can say the following:
1) While I have only limited information (a few pictures and a lateral cephalometric x-ray) it would be imprudent for me to make any in-depth comments about your candidacy for orthognathic surgery. All I can see is that you have a very significant flare to the upper and lower incisors and did not wish to undergo extractions as part of your orthodontic therapy. Thus with your current occlusal state orthognathic surgery is not an option. Perhaps that may have been different had extraction therapy been done where bimaxillary surgery may have come into play. That is a question for the orthodontists to answer.
2) Obstructive sleep apnea is a multi factorial condition of which a single piece of information (narrow airway seen on a lateral cephalometric x-ray) is way inadequate to make an accurate diagnosis. A formal sleep study is needed to determine if you have sleep apnea, whether it is central or obstructive in nature and what the appropriate treatment might be for it. It is a big leap to go from looking at the lateral cephalometric x-ray to assuming one would benefit by upper and or lower jaw advancement surgery for presumed sleep apnea.
3) Just like changing a big chin implant to smaller one (or removing it completely), subtotal reversal of a sliding genioplasty can cause lower lip incompetence. (even though that was what it was done to treat) I have heard this postoperative development from numerous females that have had subtotal sliding genioplasty reversals when the amount of forward movement was excessive. With the soft tissue elevation from the bone to perform the osteotomy, this is not totally surprising when the bone is then partially setback. Such lower lip incompetence is evident in your pictures. The question is now is whether an intraoral chin resuspension would be an effective treatment for you. While it is not always a 100% successful procedure, it is always a procedure that does not make anything worse and usually provides some improvement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in gynecomastia reduction surgery with nipple reduction at the same time. But did have one concern that another physician raised regarding a nipple reduction – specifically, the physician was very hesitant that such a procedure was worthwhile considering the risks (which he described as a 20% chance of necrosis of the nipple following such a procedure) – I would be curious to hear your assessment of this risk (or others) as pertains to a nipple reduction procedure before I make a decision.
A: I am not sure at all what is the origin of the statement by a surgeon of ‘there is a 20% risk of nipple necrosis when nipple reductions are performed with gynecomastia reduction’ for the following reasons:
1) Nipple reduction in a male almost always means nipple amputation, the complete removal of the projecting nipple, thus there is no nipple left to have any necrosis. I can only assume what this doctor is more likely referring to is ‘areolar necrosis’ or difficulty with the nipple reduction site healing. This has not been an issue that I have ever seen.
2) This ‘statistic’ is based on what I do not know since there has never been anything published in the plastic surgery literature in that regard or any other literature since the performance of male nipple reduction in gynecomastia reduction is so rarely done.
3) The relevancy of potential vascular compromise to the nipple-areolar complex is based on what type of gynecomastia reduction is being performed. If an open gynecomastia reduction is performed through an inferior areolar incision, where the nipple-areolar complex is left with a thin layer of tissue underneath it and it depends on vascular inflow from the surrounding dermis (where half has been cut off from the inferior areolar incision). then one would have reason to consider there may be the potential for vascular compromise from the healing nipple reduction site. But this issue becomes moot when the gynecomastia reduction is performed by liposuction without a direct areolar incision.
4) But when in doubt one can always delay the nipple reduction for a week or two after surgery since it can easily be done as an office procedure under local anesthesia. (where the chest is largely numb anyway for awhile)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about the shoulder width reduction surgery. I am very insecure about how broad my shoulders are. I’ve always wanted a delicate, feminine shape so that I could wear whatever I wanted to without feeling like I had to hide a part of myself. For reducing the width of your shoulders, is the restraint of ~ 4-5cm removed per operation, or in a lifetime? Would repeat surgeries be possible if a person wanted to remove more than 4-5cm? As you can see there is a very drastic difference between my shoulder width and hip width.
A: Thank you for your inquiry and sending your picture. Your question about whether one should have a second clavicle reduction surgery is an interesting one and I can not speak from personal experience having never done it as such as the issue has never arisen before. But I would see no reason why one could not later have a second shoulder width reduction surgery if one desires at the same osteotomy site. Obviously the goal the first time would be to make that unnecessary taking out 3cms oer side. I think you might be surprised how much difference that can make and hopefully the consideration of a second surgery for you remains a theoretical one.
Dr. Barry Eppley
Indianapolis, Indiana