Your Questions
Your Questions
Q: Dr. Eppley, I would like to have a forehead augmentation. I am a female and have a small feminine-type forehead and would like a bigger more masculine forehead, one that is much more convex in shape. It is very clear to me now that the women I find the most beautiful almost all have a large forehead. Prior to the operation I will get permanent hair removal on the hairline. I think this hairline makes me look like an angry man from the sides. Thank you very much.
A: Forehead augmentation can be done to create a variety of aesthetic forehead changes. For many women that seek forehead augmentation, they are interested in a rounder or more convex forehead shape. This is one where there is no distinct brow break and a forehead shape that extends upward from the brow area in varying amounts of projection before heading back into the hairline. The degree of convexity, so to speak, is a matter of patient preference. The only issue in larger amounts of forehead augmentation is to make sure that it tapers gradually into the temporal line area on each side. Lack of a more gradual side transition can create a boxy forehead shape when the central augmentation amounts start to exceed more than 10 to 15mms.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in abdominal scar revision. I’m a 35 year old female who has a very big scar on my abdomen from an open surgery on my pancreas (Whipple procedure) done six months ago due to chronic pancreatitis and necrotizing pancreatitis. You can see where the staples were on the scar as well. I also have two small scars on both sides of my belly button from the same surgery where they attempted laparoscopic surgery. I’m most insecure about the huge scar from the open incision. Is it possible to remove this scar? What options are available to remove or reduce this scar? What cosmetic procedure is recommended? Can you tell me about these procedures? As it has only been 6 months since my surgery, how long would I have to wait before having a cosmetic procedure? As you can see I have a few other scars from a laparoscopic surgery to remove my gallbladder years before These scars are inside/right outside my belly button, two on the far right side of my upper abdomen, and one in the center of my upper abdomen right near my new scar. These scars are small and blend in well with my skin now. Will my other smaller scars from this past surgery blend in like these eventually or would it be possible to remove or revise all the scars? Would my current health be a factor in determining if I’m a candidate for cosmetic surgery? Please advise me as best as possible. I would really appreciate your help. Thank you!
A: In answer to your abdominal scar revision questions:
- I believe all of your scar appearances from this past extensive surgery are stable, will not improve, and can be revised at any time.
- As long as your healthy enough to go through surgery and heal uneventfully, then you would have no problem with extensive abdominal scar revisions. I would need to know more general health information and any medications that you may be on to answer this question better.
- Your scar revisions would be complete scar excision with abdominal skin flap raised to close the extensive subcostal excision area. (like a reverse tummy tuck skin flap)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have stretch marks covering most of the center of my abdomen. They are about two years old. I am curious about the pricing of your fractional CO2 laser resurfacing as well as recommendations for the best type of treatment or any other suggestions.
A: When it comes to treating stretch marks, there are no completely effective strategies. They may be able to be reduced but can never be completed eliminated. Fractional CO2 laser resurfacing, while effective for facial skin wrinkle reduction and skin rejuvenation, has not shown a similar profound effect on stretch marks. The best way to determine if it would have any beneficial effect would be to do treat a small area first (test patch) before embarking on treating the whole area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a lot of facelift questions for you. Which ‘full facelift’ technique do you offer? Do you offer the deep plane composite facelift technique with a 80% vertical pull and 20% lateral pull? I see on your website that most of your pulling is towards the ear. Doesn’t this result in a ‘wind pull’ ‘done’ appearance? The vertical pull seems to be more natural. And using the deep plane technique to offer a longer lasting result by accessing the the premasseter space, to lessen the jowl, and the labiomandibular fold?
A: Facelift surgery comprises a large number of techniques that can principally be broken down into incisional locations, skin flap undermining, SMAS management, platysmal muscle manipulation, method of fat removal and/or fat volume replacement. Any facelift procedure and its results and longevity is really a symphony of how these parts are put together that can really be different for each patient. Rarely do two facelifts have exactly the same anatomic components. I would submit that each and everyone of these parts have a role to play in the outcome and no one component alone is responsible for how a facelift result will look or how long it will last. There is also the other important variable which is the patient themselves…how extensive a procedure do they want, how much recovery and swelling can they tolerate and what is their budget.
But since you have ask about the SMAS component of a facelift I will address that issue in detail only as it relates to results and longevity. Manipulation of the SMAS layer in a facelift can be done by numerous methods including suture plication with no undermining to extensive undermining with a SMASectomy and plication. (what you are partially referring to with the term deep plane) While some manipulation of the SMAS has proven benefits over none at all (a simple subcutaneous facelift) it is has never been conclusively proven that deeper methods of SMAS undermining produce a more natural result or last longer than lesser degrees of SMAS undermining. It would theoretically seem like it would, and it may well be, but proving it (other than some surgeon’s touting it as so) is another matter. Its proof would be difficult as it would require one type of facelift being done on one side of the face and another on the other side in a series of patients.
It is also important to understand the movement of the SMAS layer and the overlying skin may and often are different. Since the skin and SMAS are commonly separated, their tissue movements are usually in slightly different vectors. The SMAS layer can be done in a completely vertical direction (when it is plicated) or in a more superolateral direction when it is undermined and repositioned. Likewise the skin layer can be similarly moved in these directions. Both the SMAS and skin layers are moved in varying degrees of superolateral movements. There is no such true lateral repositioning in either the SMAS or the skin layers. This is probably where you have gotten the phrase ’80% vertical and 20% lateral’, demonstrating that tissue relocation in a facelift is a combined superolateral translocation of tissue that is directed primarily towards the ear and the lower temporal region.
When it comes to what makes a facelift look natural, it is not an issue that is caused by one facelift technique being better in that regard than another. All facelift techniques, big or small, can make for an unnatural result. It is most significantly influenced by the ‘artistry’ of the plastic surgeon…not overlifting or overpulling any tissue layer and in how the incisions and hairline are managed around the ears and the temporal hair-bearing region. (e.g., more vertical directions of skin movement will move the hairline up higher unless that is factored into the incision design.
The deep plane composite facelift is unique amongst facial rejuvenation techniques because it basically does not separate the skin and the SMAS layer once beyond the anterior border of the parotid gland. Once the tissue plane is elevated, the entire composite of tissues is then lifted and secured. This composite tissue unit will always have a more vertical direction of relation, because if it does not, the amount of change would be minimized because the skin is attached to the SMAS layer throughout the flap. The deep composite facelift takes the longest to perform, has the greatest risk to injury of the buccal facial nerve branches, and will have a longer recovery due to prolonged swelling. Its best benefit, in my experience, is that it is the ‘safest’ facelift technique in smokers and others that may have compromised healing as the blood supply to the overlying skin is not disrupted by making a completely separate tissue layer from the SMAS.
Facelifting in men offers several unique considerations. The vector of tissue lifting in men has to be as vertical as possible since any significant lateral movement will result in having to workout tissue excesses behind the ear, risking a longer and more visible scar into the occipital hairline. Moving the sideburn higher is overcome by merely growing out the beard skin to drop the hair level back down. (which is why it is advised that men grow longer sideburns before the procedure) Too much of a lateral movement will also risk placing the beard skin closer to or on the tragus of the ear which is obviously undesirable. (although this can be prevented regardless of tissue movement by the location of the incision) Men are also unique facelift patients as their tolerance for a lot of swelling and prolonged recovery is not typically very high.
As you can see, facelift surgery is a myriad of assembled parts. While it is understandably convenient to label them as certain types, each facelift technique has varying influences on the outcomes, recovery and risk of complications. One facelift type is neither completely superior nor applicable to every patients’s facial aging needs and concerns.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question concerning using injectable fillers in the jawline. I’m considering doing a jaw implant, not so much to widen the jaw but to lengthen the jawline down in the vertical direction. I know that injectable fillers (such as Juvederm Voluma) is a great option when it comes to widening the jaw and this is commonly done. But my question is if it´s possible to also lengthen the jawline in the vertical direction with fillers. Is it a good use of an injectable filler? I don´t want it to float about when your laugh for instance but I guess it could be a good strategy to start with fillers before possibly doing an implant. I also would like to know how much approximately you can lengthen it with fillers, maybe 4mm to 5 mms?
A: Injectable fillers can be a good starting point when considering any type of facial skeletal augmentation including the jawline. It will work equally well for vertical jawline lengthening as well as jawline widening/accentuation. It will not move around anymore on the lower edge of the jawline than it will when it is placed on the side.
Dr. Barry Eppley
Indianapolis, Indianapolis
Q: Dr. Eppley, Could you tell me when diced cartilage injections are recommended in rhinoplasty? Five years ago I received a septal cartilage graft on my nasal dorsum but there remains a little gap on the side of the dorsum between the eyes. Could a diced cartilage injection resolves my problem? Does it need a lot of spetal cartilage which was used initially for my dorsal cartilage graft?
A: Small cartilage deficient areas of the nose are fairly ideal for an injectable diced cartilage rhinoplasty. What you are ‘missing’ is that the dorsal augmentation has created a relative deficiency along your nasal sidewalls. That could be filled in with diced cartilage injected from an intranasal approach. A small septal or ear cartilage should suffice as the cartilage donor source.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve been looking into cranial augmentation and it has led me to here. You seem to have a lot of experience in the matter so I have a few questions. I have flatness in the back of my head and also a hump on the top of my head. If you look at my pictures, the flatness starts at point A up to the top of my head. The hump starts at point B and continues to point C. I have also outlined a drawing of how I would like the final result to shape into. My questions are:
1. Can both of these issues be corrected in the same procedure and through the same incision point?
2. Could a single vertical incision,essentially from point A to point C give better access to address both issues, or is a coronal incision still the method of choice?
3. I would be an out of town patient. If I were to go through with the procedure, how many days would I have to stay in the Indianapolis area for?
A: When it comes to skull reshaping, it is very common to simultaneously perform areas of reduction and augmentation. In answer to your specific questions:
- Both the sagittal ridge reduction and the occipital augmentation can be done through the same incision at the same time.
- The transverse coronal incision would be the standard approach. While there is nothing wrong per se with a sagittal or vertical incision, as equal access to do the procedure can be obtained as the coronal incision, there would be greater scar widening with that scalp incision orientation.
- You would be able to leave for home by 48 hours after surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I am interested in a testicular implant. I’ am 24 years old and I have monorchism. When I was in grade school my older brothers thought it was funny to tell every one and this humiliation as stuck with me my whole life. They called me “Half a Man” or “UniBall”. It was a traumatic experience to say the least. Now that I am older I would like to have an implant put in. I just want to feel normal. I’ve read enough about testicular implants over the years to know the surgery is considered an aesthetic procedure but there’s so much more to it than that. Is there any way an insurance provider would consider covering such a surgery?
A: Whether insurance would cover a procedure like a testicular implant is one they have to answer. I can not predict with any accuracy what any insurance may or may not do. My experience would suggest, however, that they are likely to call it a cosmetic procedure as it serves no medical benefit. (unfortunately they do not consider the psychological aspects of any missing or deformed body part as being medically significant) However this is a question that you would have to ask your insurance carrier.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a rhinoplasty combined with orbital and maxillary osteotomies on me. I am wondering if it is possible to completely or partially reverse the osteotomies specially the orbital ones. In my picture you see how there is a bone that sort of curves from the eyebrow to the eye corner and then from the eye corner to under the eye and then becomes the nasal sidewall? This bone is missing now. The entire nose is thinner at the dorsum and base of the pyramid and the bone between my eyes is thinner too. The operative report says he performed medial and lateral osteotomies. I don’t like how my sidewalks are gone… Is there a way to make my bones back to how they used to be? My nose is flat on the sides and has a very thin dorsum I had to add filler to make normal-looking. I liked my wide sidewalls before the surgery. The best way I can explain this is that the ascending process of the maxilla used to be very far apart from each other and now it’s all closer to the midline.
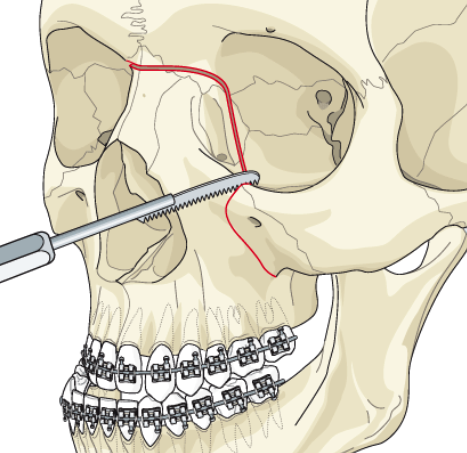 A: What you had done was a LeFort II osteotomy. Bringing the nasomaxillary complex forward, it could be predicted that the nasal sidewalls would get more narrow. This is due to not only the bony area moving forward (telescoping effect) but the probable collapse of this thin bone area from the destabilizating effect of the osteotomies.
A: What you had done was a LeFort II osteotomy. Bringing the nasomaxillary complex forward, it could be predicted that the nasal sidewalls would get more narrow. This is due to not only the bony area moving forward (telescoping effect) but the probable collapse of this thin bone area from the destabilizating effect of the osteotomies.
To rebuilt this area, there are multiple options depending upon the type of graft to be used and the surgical approach. The simplest approach would be using injectable fat with the disadvantage of the high unpredictability of its survival. I would only do this if one was seeking a ‘non-surgical approach. Another semi-injectable approach would be the placement of hydroxyapatite cement placed through intranasal incisions. (similar to how nasal osteotomies are done) More traditionally, the bone grafts can be inserted through either an intranasal, eyelid or coronal approach. I assume that your LeFort II procedure was done through a combined intraoral and coronal incisions.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in pubic liposuction. I have an enlarged mons pubis and always have. It sticks out, is soft and doughy and protrudes further than my stomach. I wonder if my pelvic bones are at the wrong angle. My mound has really no sensation which I assume is because it is just a mound of fat. This is very embarrassing as I am small and thin with a weight of 104 lbs at 5’ 2” tall. While my weight fluctuates a little, there is no change in the size of the pubic mound. I am assuming that some form of liposuction is the best method to reduce this mound to a flatter profile.
A: A protrusive pubic mound is a not uncommon problem for many women. It is most frequently seen after a tummy tuck where the waistline is the most narrow circumferential area and a residual pubic mound (not recognized before surgery) now sticks out further than most of the stomach. It can also be seen in very thin women who naturally have a thicker fibrofatty layer on their pubic mound. This type of fat is not responsive to weight changes as it has a protective padding purpose and not a metabolic fat depot role.
 You are correct in assuming that pubic mound liposuction is the definitive treatment. While much is made of the type of liposuction used, the reality is that ‘simple’ non-energy based liposuction will work just as well. The key is that it must be of the small cannula variety since the area is so small. This discrete type of small fat removal does fall into the moniker of ‘liposculpture’.
You are correct in assuming that pubic mound liposuction is the definitive treatment. While much is made of the type of liposuction used, the reality is that ‘simple’ non-energy based liposuction will work just as well. The key is that it must be of the small cannula variety since the area is so small. This discrete type of small fat removal does fall into the moniker of ‘liposculpture’.
Pubic mound liposuction can be done under local or IV sedation, takes less than one hour to do, and involves very little recovery. One needs to be aware that there will be some bruising and swelling of the mound and labia and that it will take several months until the pubic area feels soft and normal again.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull augmentation I was wondering if you ever use an inflatable under the crown of skull to inflate skin so you can have more room to shape head? My niece needed an inflatable on her leg when she was young, which they used when they removed cancerous skin. I believe they can do this if area on skull needs extra skin to cover cement. If you do this, maybe you can tell he how much and my procedure can be a two step procedure. If I can pay for this and come back when time for procedure to correct and reshape flat areas. Please let me know. Not sure what the procedures are called but I may need more serious fix and may need more room for reshaping.
A: When it comes to skull reshaping or skull augmentation, you are referring to a two-stage approach initially using a tissue expander. For larger amounts of skull augmentation, particularly for a flat back of the head, more scalp is needed. A small scalp tissue expander, slowly inflated over six weeks, creates more than enough extra scalp tissue to cover any degree of augmentation desired.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I need help in figuring out the best way to enhance facial volume. I have hollowing under my eyes and would like a stronger jawline. I had cheek implants placed two years which have done great so am looking for similar impact on my other facial areas. But I’m not sure what the best way to accomplish this is using either facial implants, fat injections or injectable fillers.
A: When it comes to facial volume enhancement the surgical debate is always whether it should be done by fat injections or facial mplants. This is no different that the debate would have been about your previous cheek augmentation. There are advantages and disadvantages for either approach but that debate must be assessed more specifically for the facial area that one wants to enhance and whether it is composed of underlying bone, soft tissue or both.
The jawline is primarily supported by bone so any effective augmentation is almost always done by some form of implant placement. You would have to further define what jawline area to which you want changed to better answer what type of implant may best address it. This is identical to your cheeks which are usually most effectively done by implant because they are a bony supported area.
The under eye area is different than the jawline because it is a combined bone and soft tissue area. The lower end of the under eye area is the inferior orbital rim while most of the lower eyelid is soft tissue supported. This usually means that fat injections are needed as an implant only covers the very lower end of the under eye area and placing it requires a lower eyelid incision to do so. So fat injections, even though they are unpredictable, usually win out over any implant augmentation. Their ‘softness’ is kore appropriate for the under eye area than the jawline.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about skull reduction surgery. I have read online said that you can reduce the head. I have always been very conscious about how wide my head Is. It’s wide and big. What can you do exactly? May I send you some pics so you see what I am talking about? I also am losing hair and I read on your website that you don’t recommend the procedure for hair loss. But I am not entirely sure how you narrow the head, mine is very broad. I often wear hats because I am self conscious about my wide head and hair loss.
A: Thank you for sending your pictures and expressing your concerns. There are procedures that can very effectively reduce the size of your head including temporal muscle reduction and bone burring. (skull reduction) There is no doubt in my experience that they could change the way you see your head. However, to do these procedures one needs a scalp incision to do it and with your hair loss I would have grave concerns about the remaining fine line scar from the surgery. Thus in your case I would seriously question that aesthetic trade-off. You don’t want to trade one problem for another. While there are trade-offs in every aesthetic procedure, what one trades into should be perceived as being better than what they currently have.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull reshaping surgery. I am a 35 year old female who is concerned about head size and shape. My head is wide and big overall. Especially, the top and the sides of parietal bone are bulged so that it is really difficult to find hats to wear. I hope to reduce the top and side portions of my skull as much as possible. Having the surgery done is only way to get to rid of my life long distress. Is it possible for a patient who lives outside of the US to get this surgery done? The hardest part for me is to take a long absent from work so the time is my big concern. How many visits are required before and after the surgery? If I am sure to have the surgery, is it possible for me to visit you first time and get the surgery done in a week or so? I could possible use the weekend for before and after consultations. Another concern is that I need to visit and get through it by myself. Would that be okay?
I am sending you some pictures. Because of my thick hair, it might be hard to understand my head shape. But my hair is wet and pushed to my skull. I would not say my head is deformed. The head shape is like an apple. Both back sides of my head are sticking out. I also wish to reduce the top portion of my head as well to make my head smaller overall. Especially, the back side of the parietal region.
Here are some specific questions…I am sure you get these questions all the time.
1) What are the risks of the head reshaping surgery?
2) How much swelling will be expected? Does my head get bigger than before until the swelling goes down?
3) What will happen to the excess skin? Is it possible to cut it off? Is there any sagging skin issue after?
4) For the top and the side skull reduction how long the incision will be?
I don’t know how much physical difference you can make. But even 5 to 7mm, I will be
happy.
Sorry to bother you with many questions. Looking forward to hearing from you.
A: It is very common in my practice to have patients come from all over the world so we are very familiar with this scenario. Far away patients usually come in a day or two before surgery, have the surgery, and return home in 3 to 4 days after this type of surgery. Most do come but themselves which is why they stay overnite in the facility after surgery. Any after surgery followup is done online by email so there is no reason to return for a specific follow-up appointment. It is usually just a one time visit for the combined consultation and surgery.
In regards to skull reshaping, specifically skull reduction, the answer to your question is as follows:
1) The only risk is that there will be an incision (scar) to do the surgery and the question of how much can be reduced. (i.e., can enough be done to make the surgery worthwhile) In that regard you have made a key statement in that if even 5 to 7mms was taken down that would be viewed as an improvement. By that measurement of success, then it would be worthwhile as that is what can be maximally taken down in most areas.
2) There would be some swelling and your head would initially be slightly bigger than when you started. But the swelling is not so significantly different that it makes your head look overly big.
3) There would be no sagging skin afterwards. The scalp skin will shrink down quickly to adapt to the smaller size.
4) To get the maximal reduction of all involved areas, an incision would be needed in the more traditional coronal style, meaning a longer incision from the top of the ear from wide to side. This gives maximal exposure to do the work for the best reduction possible. It is an incision that heals well with a very fine line scar in most cases.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, two years ago I had jaw advancement and sliding genioplasty surgery. Although my face symmetry has improved dramatically, this surgery has left me with lower lip incompetence. There is a 5mm to7mm gap between my top and lower lip when my lips are in resting phase, and although I have no evident mentalis strain when I force my lips to close, I would like to know if anything can be done to correct this lip incompetence. I have read that mentalis resuspension can work but I am not sure if this applies to me as I do not know the source of my lip incompetence (though I suspect it has to do with the mentalis muscle). Please see a before and after picture demonstrating the change in my lower face shape/size as well as my lower lip incompetence.
A: Any lower lip repositioning downward after any intraoral procedure that involves an incision inside the mouth at the chin area disrupts the mentalis muscle. Whether the muscle was adequately resuspended or not I would have no idea. But when the lower jaw is advanced combined with a sliding genioplasty, the amount of soft tissue to cover over the chin may simply have become ‘inadequate’ or stretched. This is reflected in the lower lip position which is affected by being pulled downward. Whether you can overcome the lower lip position by mentalis resuspension alone is suspect. That alone is unlikely to hold the lower lip upward and reduce the incompetence. This is a problem of tissue deficiency not just one of tissue malposition. The mentalis resuspension would have to be combined with other maneuvers to have chance of success. The addition of dermal-fat graft on top of the muscle suspension and a V-Y mucosal closure would be needed to end up seeing any improvement in your lip incompetence.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am concerned about my lack of volume and height in the back of my head. In order to achieve a more normal look, I am considering the two step occipital augmentation process with the tissue expander. Would this require me to take a month off of work? Have people been happy with the results? Is it possible instead to perform a series of smaller buildups to avoid having an expander in my head for a month?
A: When large amounts of occipital (back of the head) augmentation is desired, the limiting factor is how much the scalp will stretch to accomodate the bone buildup. This is overcome by the use of a tissue expander. By initially placing an expanding balloon, the scalp is slowly stretched to the desired amount. The same effect can not be achieved by serially building up the bone due to the scalp scar tissue that is created with the bone augmentation material. Most women have little problem with continuing to work through much of the tissue expander period because their hair masks much of the scalp expansion that is occurring. In the handful of patients with flat back of the heads that wanted a large amount of occipital augmentation, all have achieved greater volume and most were happy with the new shape of their heads.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I received Botox injections for migraine headaches once and they did not give me relief, If the injections did not give me relief…then would migraine surgery not give me relief as well?
A: Botox is usually used as an indicator of success for the actual migraine surgery. When the Botox test is positive, there usually is a near 100% success with surgery. But when the Botox test is not positive, I have seen a few patients still have success with surgery. The other questions is how and where were the Botox injections done. I have seen quite a few patients who have had Botox for migraines where the injections were not done properly. As a result they had a negative test when, in fact, it might have been a positive test result if the injections were properly placed near the nerves.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve read two things regarding facial attractiveness.
1) The middle third and lower third of the face should be roughly equal in size (my middle third is 224 and my lower 216)
2) The lower third can be divided into three sections and the top section, the upper lip, should equal 1/3 of the total area and the bottom two sections, the lower lip and chin, should equal 2/3 of the total lower third height. (my upper lip is 71 and my lower lip and chin combined are 139 so it almost perfectly matches the ideal 1:2 ratio).
According to these measurements, my chin is actually not too long. This surprises me because I was always under the impression I had a long chin and would benefit from a slight reduction in chin height. (vertical chin reduction)
Do you have an opinion on my chin height? I’m trying to approach this scientifically, but I’m not sure I’m succeeding.
A: What you are learning is that facial measurements and ratios are general guidelines and do not always translate directly into perceived attractiveness. Case in point…you felt your chin was too vertically long but the numbers say otherwise. While the numbers may be ‘right’, in the end all that matters is what you think. What you need to do is approach your chin concerns in reverse…so some computer imaging with shortening the chin (vertical chin reduction) and see if it looks better to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I had cheek implants done 6 months ago, but they have unfortunately have become infected with a low-grade infection. My surgeon has advised that I get them removed, and has given me the option of either local or general anesthesia. I’m trying to save on this if possible, but I have a few concerns about going the local anesthesia route. Anyway, here are my questions:
1) Is it safe to get them removed via local? Is this something that you’ve done for your patients?
2) More importantly, how comfortable is it? Will it be a very painful experience, or just some mild discomfort at worst?
A: In answer to your questions:
1) The use of local anesthesia to remove your cheek implants is certainly safe. Fortunately I have never had a cheek implant infection so I have never had to do it. But if I did and that is the way the patient wanted to remove them, I would. Are your cheek implants silicone or Medpor. Are they screwed in? That would affect the question of whether local anesthesia is a good option or not.
2) With good local infiltration and infraorbital nerve blocks, it should be able to be done comfortably. But that would depend on the skill and experience of the surgeon in doing the local anesthetic injections.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was interested in having breast implants done via TUBA. Do you perform those? Is What is the cost of this surgery? My daughter is getting married in June and I really want to have this done before that. I have attached 2 photos. One is with my normal bra and the other is what I would like my breasts to look like (I used several bras to accomplish this). I look forward to hearing from you.
 A:Trying to place breast implants via the umbilical approach (TUBA) is a very poor way to do the operation. It is fraught with problems such as the inability to use silicone implants, difficulty in getting into the proper submuscular plane and persistent problems of after surgery upper abdominal pain. If you are looking for a scarless method of breast augmentation, the transaxillary approach is far more successful with less potential complications. Using saline implants through the armpit would also be the most economical approach to breast augmentation. It is hard to know exactly the size (volume) of implants you would need just based on how the change in the upper pole of your breasts. (as shown in your pictures) A volumetric sizing method is the best way to pick the proper size for you.
A:Trying to place breast implants via the umbilical approach (TUBA) is a very poor way to do the operation. It is fraught with problems such as the inability to use silicone implants, difficulty in getting into the proper submuscular plane and persistent problems of after surgery upper abdominal pain. If you are looking for a scarless method of breast augmentation, the transaxillary approach is far more successful with less potential complications. Using saline implants through the armpit would also be the most economical approach to breast augmentation. It is hard to know exactly the size (volume) of implants you would need just based on how the change in the upper pole of your breasts. (as shown in your pictures) A volumetric sizing method is the best way to pick the proper size for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Our four year old daughter has a flat back of the head due to positional brachycephaly. She has the additional bone growth over her ears that we would consider also having reduced. We want to know our options for building up the flat spot when she gets older. What is the right age? Have you built up flat spots for younger kids? We’d prefer to wait until she’s at least a teen but want to fully understand our options. Does the single step procedure provide enough material to build up the flat spot to the satisfaction of most clients or would you anticipate the two step method where the scalp is stretched to accommodate more material might make more sense?
A: The timing of elective skull augmentation for a flat back of head is matter of personal preference. In my opinion, it can be done very young or anytime later in life. Building up the bone requires the overlying scalp to stretch and age does make any difference in that regard. Since this is an onlay technique, the hydroxyapatite cement will grow with the surrounding bone so age is not a concern in that regard. I have done a child with unilateral occipital augmentation as young as age 4. The timing is merely a matter of parental and, if old enough, patient choice.
Because your child has bilateral occipital issues with biparietal width increase, the need to reduce the wider bone indicates a need to do it when she is older and the bone is thicker. So the teenage years would be a good consideration in your child’s case. While most cases are done in a single stage procedure, that would depend on how flat it is and how much occipital expansion is needed. If more than 15 to 20mms of occipital expansion is needed, then a first stage tissue expansion would be needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have had three babies in just under four years. Each time, I was all belly, which was ok while I was pregnant, but it’s left my stomach impossible to flatten again! I’m interested in a tummy tuck and possible liposuction on my sides. I also have an umbilical hernia. Could that also be repaired at the same time?
 A: Pregnancy, if repeated often enough and at close enough frequencies, makes numerous permanent changes to the abdomen. Stretched out skin, stretch marks and umbiilical hernias are common sequelae of pregnancy. While losing baby fat and weight can help make some difference, there is no amount of exercise and dieting that can help remove extra skin, reapproximate a rectus diastasis or fix an umbilical hernia. Because of the wide open exposure of a tummy tuck, both the umbilical hernia and the rectus diastasis can be repaired. The removal of extra abdominal skin completes the tummy tuck and can, in many cases, make a woman’s abdomen completely flat again. The amount of loose skin and fat, condition of the rectus muscles and whether a hernia exists or not makes for numerous types of tummy tucks.
A: Pregnancy, if repeated often enough and at close enough frequencies, makes numerous permanent changes to the abdomen. Stretched out skin, stretch marks and umbiilical hernias are common sequelae of pregnancy. While losing baby fat and weight can help make some difference, there is no amount of exercise and dieting that can help remove extra skin, reapproximate a rectus diastasis or fix an umbilical hernia. Because of the wide open exposure of a tummy tuck, both the umbilical hernia and the rectus diastasis can be repaired. The removal of extra abdominal skin completes the tummy tuck and can, in many cases, make a woman’s abdomen completely flat again. The amount of loose skin and fat, condition of the rectus muscles and whether a hernia exists or not makes for numerous types of tummy tucks.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a mother of three and have breastfed each baby for about 13 months. I amcurrently breastfeeding my 9 month old. Once I’m done, I’d like to have breast augmentation with gummy bear implants. After breastfeeding, I’m left with very small breasts (embarrassing!). I’ll be probably a small B cup and will want a natural looking D cup. What is the cost of gummy bear breast augmentation?
 A: Breast feeding eventually leads many women to consider or undergo breast augmentation surgery. Each child and each round of breastfeeding causes more breast tissue loss known as involution. I have seen many women who after two or more children have virtually lost all of their breast size and with that some of their feeling of being an attractive woman. Breast augmentation is a quick way to restore what was once lost. An important issues is whether you have any sagging after three children and that may necessitate some form of a breast lift with your implants. The other issue is that it is a good idea to have your milk dried up before having the surgery. (although the surgery can still be done with some light milk production) The total cost of gummy bear silicone breast augmentation is around $5500.
A: Breast feeding eventually leads many women to consider or undergo breast augmentation surgery. Each child and each round of breastfeeding causes more breast tissue loss known as involution. I have seen many women who after two or more children have virtually lost all of their breast size and with that some of their feeling of being an attractive woman. Breast augmentation is a quick way to restore what was once lost. An important issues is whether you have any sagging after three children and that may necessitate some form of a breast lift with your implants. The other issue is that it is a good idea to have your milk dried up before having the surgery. (although the surgery can still be done with some light milk production) The total cost of gummy bear silicone breast augmentation is around $5500.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had two facial problems my entire life, dark circles and retracted lower eyelids. I have always hated my look when I am not squinting and because of that I think that my ower eyelid muscles have become overdeveloped. I have attached pictures of when I squint and when I don’t. This will give you an idea of my orbital/cheek area.
The area circled in the picture was filled with Juvederm already as suggested by a local plastic surgeon to improve lower eyelid projection but it didn’t help at all. Though I do like my cheeks now and I am also thinking about making this permanent with cheek implants to give even better support to lower eyelid. What do you think about this idea? The local plastic surgeon seemed to think that cheek implants were a bad idea.
What procedures would you recommend? Also would canthopexy/canthoplasty address problem with overdeveloped muscle, or would it need to be trimmed with another procedure ? Could all procedures be done together?
A: Your pictures show a large orbicularis muscle roll of the lower eyelid (when squinting), cheek bone hypoplasia and lower eyelid hollows. (with some slight scleral show) I would recommend medium submalar shell cheek implants, a pinch lower blepharoplasty with excision of redundant muscle and fat injections for undereye hollows, all of which could be done as a single procedure. When done locally this is an outpatient procedure but, if from afar, most patients would return home in 48 hours. It would take about 10 to 14 days to look very acceptable without obvious signs of surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley ,I have a question about the Brazilian Butt Lift. I am wondering with this procedure if the fat could be taken from my stomach? Also is there an extra fee for the liposuction that takes place for the fat transfer to the buttock?
A: The fat harvest portion by liposuction of a Brazilian Butt Lift is included as part of the overall buttock augmentation procedure and fee. That is, perhaps, one of the great appeals and bonuses of the procedure. While the amount of fat that will survive after injection is unpredictable, the body contouring effects from the liposuction harvest are predictable and assured.
The stomach is almost always the first place on the body that is liposuction harvested. And for the vast majority of patients it is also the greatest source of donor fat material.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I found you from an internet search for “bulging temporal artery”. I have read that you recommend multiple location ligation done in office as the treatment. I do, however, have a few questions for you.
1. The artery doesn’t always bulge. I don’t know what triggers it but there are times it’s almost flat. Can a ligation be done ONLY if it’s bulging? (It can be irritated to swell up by rubbing or me crying)
2. Are there chances of complications? (loss of hair due to lower blood flow? Surrounding arteries swelling from diverted blood flow?) The internet has scary scenarios!
3. How would I attend follow up appointments for stitch removal etc since I’m 4 hours away?
4) How long is the recovery time and what can I expect in the way of swelling, bleeding or bruising? (take a week off or more?)
A: In answer to your questions about temporal artery ligation of a bulging or prominent temporal artery branch in the forehead/temple area:
1) It is important to be able to find the temporal artery branch to ligate it. So some degree of bulging is needed for the surgical ligation procedure to find the potential multiple ligation points.
2) Other than some very small scars, the risks of the procedure are merely as to how well it works. There is no risk of hair loss and surrounding arteries become dilated as a result of these ligations.
3) The small suture that are placed are dissolveable so there is no need for any follow-up visits.
4) There really is no recovery of any significance. Other than some small swelling at the ligation points, there are other issues of concern.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was inquiring on if you have any experience with congenital symmastia? It’s something that I’m quite certain I have and something that has always bothered me. I do not think I need breast implants and my breasts are a good size. But I do not like this web of skin that crosses between my two breasts. In bras it looks even worse. How can this be corrected?
A: Symmastia presents in one two ways, either from a congenital basis (like yours) or iatrogenically created by breast augmentation surgery. In congenital symmastia, there is usually a web of tissue between the two breasts. In this web there is fat and therein lies the way to treat it…liposuction. By removing the fat in the web and with postoperative compression, the tissue between the breasts can be made to stick down to the sternum thus eliminating the web. This can be done as s stand alone procedure or combined with breast augmentation. (although by your pictures this is not something that you need)
The success of symmastia correction by liposuction depends on how well the skin will adhere down to the sternum. After liposuction compression is applied but this is a difficult area in which to keep good compression on the skin for any sustained amount of time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in breast reduction surgery. Next month I am having barbaric surgery with a sleeve done. I have had a lot of female problems. I am having pain in my back and my chest from my large breasts. I do have Aetna Insurance so how does that process work to get a reduction on my breasts and having the insurance cover it?
 A: Breast reduction is often covered by insurance and the process to determine if they will pay for it is known as predetermination. This requires photos to be sent as well as documentation that efforts at physical therapy are done (I don’t make the rules, we just have to follow them) for the insurance company to consider coverage. However, if you are going to lose weight, particularly through bariatric surgery, breast reduction surgery should only be considered after the weight loss has occurred. Significant weight loss has been shown to affect breast volume. You may find out that you only need a lift and not a reduction as extreme amounts of weight loss can cause a lot of breast volume to be lost. Wait to consider breast reshaping/reduction surgery until your breasts are in a stable period where your weight is where you want it or the best that it can be.
A: Breast reduction is often covered by insurance and the process to determine if they will pay for it is known as predetermination. This requires photos to be sent as well as documentation that efforts at physical therapy are done (I don’t make the rules, we just have to follow them) for the insurance company to consider coverage. However, if you are going to lose weight, particularly through bariatric surgery, breast reduction surgery should only be considered after the weight loss has occurred. Significant weight loss has been shown to affect breast volume. You may find out that you only need a lift and not a reduction as extreme amounts of weight loss can cause a lot of breast volume to be lost. Wait to consider breast reshaping/reduction surgery until your breasts are in a stable period where your weight is where you want it or the best that it can be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in some form of a buttock lift. I I would like to have the extra skin/wrinkles removed from my butt. I have hoped to find a procedure that did not include implants. Do you feel I am I a candidate for this surgery procedure?
 A: What you are demonstrating is a severe buttock sag with a lot of folds/rolls of skin around the bottom of the buttocks. This often occurs in very thin women as they age and may also happen after a significant amount of weight loss. While it it true that buttock augmentation would help pick up some of this loose skin, it would take a massively large augmentation to do so. The better approach is to do a lower buttock lift or tuck which removes all the skin folds on the bottom half of the buttock. This places the scar along what should be the infragluteal fold or lower buttock crease. This will not increase the volume of the buttocks, which will still be very flat but it will get rid of a lot of that saggy skin which makes one’s buttocks look a lot older than they really are.
A: What you are demonstrating is a severe buttock sag with a lot of folds/rolls of skin around the bottom of the buttocks. This often occurs in very thin women as they age and may also happen after a significant amount of weight loss. While it it true that buttock augmentation would help pick up some of this loose skin, it would take a massively large augmentation to do so. The better approach is to do a lower buttock lift or tuck which removes all the skin folds on the bottom half of the buttock. This places the scar along what should be the infragluteal fold or lower buttock crease. This will not increase the volume of the buttocks, which will still be very flat but it will get rid of a lot of that saggy skin which makes one’s buttocks look a lot older than they really are.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 32 year old female interested in having chin reduction surgery. I underwent orthognathic surgery in 2011 to correct a class III malocclusion and to straighten my midline with a bilateral sagittal split mandibular setback osteotomy. I am pleased with the way my bite looks as a result of this surgery, but I am still unhappy with the extent to which my chin protrudes. I am very interested in learning what can be done to reduce the size of my chin and to improve my facial profile. I have attached some frnt and side view pictures for you to review.
A: Chin reduction surgery must take into account the extent of bone and soft tissue to determine what technique to use. What I see is a central button of bone on the chin which appears to be the primary culprit. It looks like it could be horizontally reduced by at least 5mms and the bone tapered backward along the jawline a few cms. The real question is whether this should be done by a submental or an intraoral approach. It is tempting to do it from inside the mouth but there is always the issue of what will happen with the overlying skin. As tempting as that seems with a smaller chin excess problem like yours, that is probably a mistake. The submental approach has the added benefit of removing and tucking in any soft tissue excess which complements the bone reduction.
Dr. Barry Eppley
Indianapolis, Indiana