Chin Surgery
Chin Surgery
Dr. Barry Eppley has years of experience helping his chin augmentation and chin reduction surgery patients with their aesthetic needs. Please visit the chin surgery before and after photos page to view patients who have undergone this procedure.
THE AESTHETICS OF THE CHIN – MALE vs FEMALE

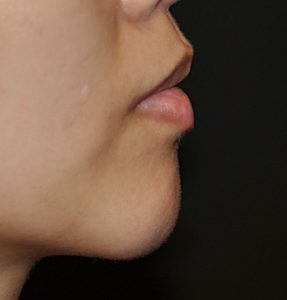
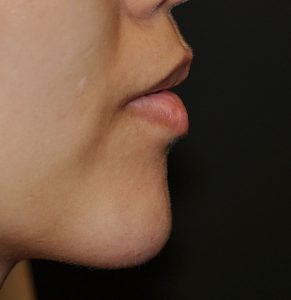
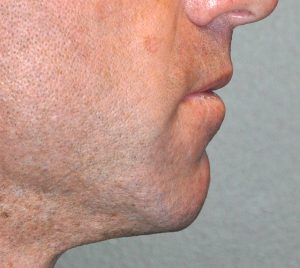
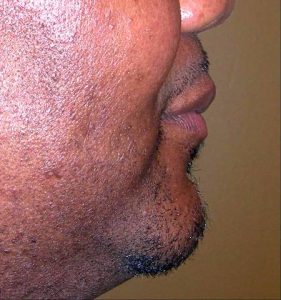
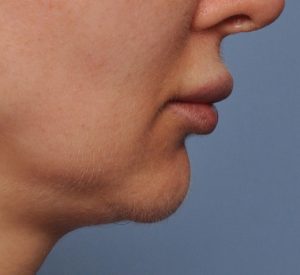
 The chin serves as the most prominent feature of the lower third of the face…at least ideally. As a result, it has a major influence on facial appearance and how the face is perceived by others. Whether it is too small, too big, too narrow or too wide, there are many options for changing the shape of one’s chin. One very important consideration in any chin surgery is an appreciation of the differences between the male and a female chin. The male chin projects further forward and is wider, sometimes eve square. Conversely the female chin is more narrow with a little bit less projection and sometimes less vertical length. Understanding these gender differences is extremely important when doing any form of chin reshaping surgery as they often become one of the major aesthetic reasons for revisional chin surgery.
The chin serves as the most prominent feature of the lower third of the face…at least ideally. As a result, it has a major influence on facial appearance and how the face is perceived by others. Whether it is too small, too big, too narrow or too wide, there are many options for changing the shape of one’s chin. One very important consideration in any chin surgery is an appreciation of the differences between the male and a female chin. The male chin projects further forward and is wider, sometimes eve square. Conversely the female chin is more narrow with a little bit less projection and sometimes less vertical length. Understanding these gender differences is extremely important when doing any form of chin reshaping surgery as they often become one of the major aesthetic reasons for revisional chin surgery.
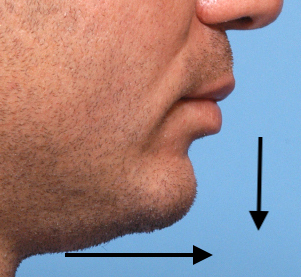
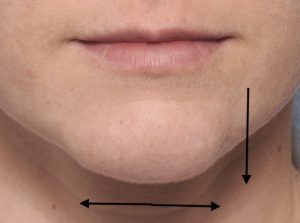 In addition to gender differences the other extremely important consideration in chin reshaping surgery is dimensions. What are the specific dimensional needs that need to be changed to achieve the patient’s aesthetic goal? (horizontal projection, vertical length and transverse width) As a projecting facial structure all three dimensions must be considered in determining the best procedure in how to change its shape. Chin shape is too often only assessed in the side or profile view when selecting the treatment or evaluating the results which is inadequate. It is important to remember that patients see themselves most often in the front or three quarter view. (although today cell phones and selfies allow people to see their side view more than ever before)
In addition to gender differences the other extremely important consideration in chin reshaping surgery is dimensions. What are the specific dimensional needs that need to be changed to achieve the patient’s aesthetic goal? (horizontal projection, vertical length and transverse width) As a projecting facial structure all three dimensions must be considered in determining the best procedure in how to change its shape. Chin shape is too often only assessed in the side or profile view when selecting the treatment or evaluating the results which is inadequate. It is important to remember that patients see themselves most often in the front or three quarter view. (although today cell phones and selfies allow people to see their side view more than ever before)
There are multiple dimensional changes that can be done to the chin bone as well as its overlying soft tissue. This includes the bony changes of chin augmentation and chin reduction as well as soft tissues alterations of ptosis repair, labiomental fold reduction and the creation/removal of chin dimples and chin clefts.
CHIN AUGMENTATION
One of the historic and still most common reason for aesthetic chin surgery is to augment a deficient chin. A short chin makes the neck look full, the jawline ill-defined, and can make the nose seem larger than what it is. Chin augmentation has one of the most dramatic effects of all of the facial procedures can be done by injection, implants or moving the chin bone forward
Injectable Chin Enhancement
 Any of the available synthetic injectable fillers can be used for a chin augmentation effect. The more viscous the filler the more push it will have on the overlying soft tissue chin pad. For the first time patient it is best to use a hyaluronic acid-based filler with the assured complete resorption of it should the effect not be desired. Only graduate to semi-permanent fillers, which are not easily dissolved or may not completely resorb, when one is certain that adding volume by injection aesthetically works. While not permanent injectable fillers provide a modest chin augmentation effect that can also be used for giving it a shape change as well. One of the benefits of an injectable chin augmentation is that it can serve as a trial procedure…try a reversible method first if one is not absolutely certain chin augmentation would produce a favorable change.
Any of the available synthetic injectable fillers can be used for a chin augmentation effect. The more viscous the filler the more push it will have on the overlying soft tissue chin pad. For the first time patient it is best to use a hyaluronic acid-based filler with the assured complete resorption of it should the effect not be desired. Only graduate to semi-permanent fillers, which are not easily dissolved or may not completely resorb, when one is certain that adding volume by injection aesthetically works. While not permanent injectable fillers provide a modest chin augmentation effect that can also be used for giving it a shape change as well. One of the benefits of an injectable chin augmentation is that it can serve as a trial procedure…try a reversible method first if one is not absolutely certain chin augmentation would produce a favorable change.
The other injectable chin augmentation method is by fat injections. While a bit more surgical in nature due to the harvest, it is still a method to non-invasively create a chin augmentation effect. Fat injections are not always completely predictable in terms of volume persistence but do have a chance to be so. Because the fat is mainly injected into the soft tissues it is not easily reversible should the augmentation result be excessive or irregular/uneven.
Chin Implants
 Chin implants have a long hist0ry of clinical use and design evolution. As a general guideline, chin implants are typically used when small to moderate amounts of permanent chin augmentation are needed. Equally importantly is that chin implants can provide considerable horizontal projection, many styles have a widening effect if desired but they have a limited ability to create much vertical height increase in most implant styles.
Chin implants have a long hist0ry of clinical use and design evolution. As a general guideline, chin implants are typically used when small to moderate amounts of permanent chin augmentation are needed. Equally importantly is that chin implants can provide considerable horizontal projection, many styles have a widening effect if desired but they have a limited ability to create much vertical height increase in most implant styles.
Since chin implants have been around the longest of any type of facial implant and is still the most common standard facial implant used, a wide variety of chin implant styles and sizes exist. Given that many of them have surgeons’ names and the appearance differences between them can be subtle, it is not surprising that how to choose amongst them can be confusing.
 Adding to this confusion are the different materials available for preformed chin implants (solid silicone, Medpor and ePTFE) to which I can say ….the body doesn’t care what the material is. It treats them all the same as synthetic materials. (foreign bodies) None possess better biologic advantages over the other even though some patients and surgeons may think so. They might get slightly different tissue responses (complete smooth encapsulation vs capsular adherence) but an implant is still an implant. I have used them all and what differentiates them are nuances in handling characteristics, ease of insertion and removal and how well they can be intraoperatively contoured and positioned.
Adding to this confusion are the different materials available for preformed chin implants (solid silicone, Medpor and ePTFE) to which I can say ….the body doesn’t care what the material is. It treats them all the same as synthetic materials. (foreign bodies) None possess better biologic advantages over the other even though some patients and surgeons may think so. They might get slightly different tissue responses (complete smooth encapsulation vs capsular adherence) but an implant is still an implant. I have used them all and what differentiates them are nuances in handling characteristics, ease of insertion and removal and how well they can be intraoperatively contoured and positioned.

 But none of these different implant materials choices should supersede what is most needed from them….can they fulfill the patient’s desired dimensional chin augmentation needs? The ‘best’ implant material will fail if it can not meet the desired size and shape of the patient’s chin augmentation goal. Solid silicone chin implants remain the most commonly used as they offer eleven (11) different implant styles.
But none of these different implant materials choices should supersede what is most needed from them….can they fulfill the patient’s desired dimensional chin augmentation needs? The ‘best’ implant material will fail if it can not meet the desired size and shape of the patient’s chin augmentation goal. Solid silicone chin implants remain the most commonly used as they offer eleven (11) different implant styles.

 Chin implants can be inserted from either under the chin (submental) or from inside the mouth. (intraoral) There are advantages and disadvantages to either chin implant insertion approach. The submental (under the chin) skin approach offers the most direct access to placing the implant over the inferior end of the chin bone where they are designed to sit. The intraoral approach may be scarless but is prone to superior malpositioning unless screw fixation issued.
Chin implants can be inserted from either under the chin (submental) or from inside the mouth. (intraoral) There are advantages and disadvantages to either chin implant insertion approach. The submental (under the chin) skin approach offers the most direct access to placing the implant over the inferior end of the chin bone where they are designed to sit. The intraoral approach may be scarless but is prone to superior malpositioning unless screw fixation issued.
Chin implants are frequently done in conjunction with other aesthetic facial surgeries, particularly rhinoplasty and facelift surgery. Different forms of neck reshaping such as liposuction and submentoplasties enhance the chin augmentation effect.
Sliding Genioplasty
Changing the position of the bony chin through an osteotomy is the alternative to that of an implant for certain chin reshaping effects. Unlike an implant, however, a bony genioplasty is capable of a wider array of dimensional changes. The bony chin position can be changed in all three dimensions from increasing horizontal projection, adding vertical length as well as making the chin wider or even less wide. These dimensional changes in combination with being an autologous operation are its main differences over an implant.
 The term ‘sliding genioplasty’ is how this bony chin operation is most commonly referred. But this is an archaic and inaccurate term today as to how the operation is done and used. Historically this operation was done as the name implies…the chin bone was cut and slide forward along the osteotomy line and then held in position with wire fixation. It was largely restricted to a horizontal movement and the use of wire fixation limited in to that main effect. But along came plate fixation and the movement of the chin was no longer controlled by the osteotomy line. Plate fixation allows the downfractured bone segment to be placed in the dimensional position desired without the need for complete bone contact for healing. As a result a more contemporary term for the operation should be a ‘bony genioplasty’ with the prefix as what dimensional change is being done.
The term ‘sliding genioplasty’ is how this bony chin operation is most commonly referred. But this is an archaic and inaccurate term today as to how the operation is done and used. Historically this operation was done as the name implies…the chin bone was cut and slide forward along the osteotomy line and then held in position with wire fixation. It was largely restricted to a horizontal movement and the use of wire fixation limited in to that main effect. But along came plate fixation and the movement of the chin was no longer controlled by the osteotomy line. Plate fixation allows the downfractured bone segment to be placed in the dimensional position desired without the need for complete bone contact for healing. As a result a more contemporary term for the operation should be a ‘bony genioplasty’ with the prefix as what dimensional change is being done.

 Compared to a chin implant the amount of forward projection by moving the bone is greater. How far the chin bone can be moved forward is dependent on the thickness of the mandibular symphysis. Horizontal movements can be up to 16mms. But the tradeoff for medium to larger forward chin bone movements is that the chin will likely appear more narrow in the frontal view. This occurs due to the geometric effects of taking the front part of an inverted U (when viewing the jaw shape from below) and making the front edge of it longer. This is an important consideration for men and is where an implant can provide width as the chin projection is increased. In women, however, this narrowing effect may an aesthetic advantage to keep the natural chin width or make it even more tapered. One other effect that a sliding genioplasty has is to pull the neck muscles forward that are attached to its backside or lingual surface. This offers some neck shape improvement that an implant does not.
Compared to a chin implant the amount of forward projection by moving the bone is greater. How far the chin bone can be moved forward is dependent on the thickness of the mandibular symphysis. Horizontal movements can be up to 16mms. But the tradeoff for medium to larger forward chin bone movements is that the chin will likely appear more narrow in the frontal view. This occurs due to the geometric effects of taking the front part of an inverted U (when viewing the jaw shape from below) and making the front edge of it longer. This is an important consideration for men and is where an implant can provide width as the chin projection is increased. In women, however, this narrowing effect may an aesthetic advantage to keep the natural chin width or make it even more tapered. One other effect that a sliding genioplasty has is to pull the neck muscles forward that are attached to its backside or lingual surface. This offers some neck shape improvement that an implant does not.

 The ability to make this simultaneous two-dimensional chin augmentation change is an historic advantage of a bony genioplasty over that of an implant. While some argue that a chin implant can be positioned lower on the bone to create this effect, this effect is limited and such implant positioning is potentially unstable. How much vertical elongation and horizontal projection can be combined and still maintain some bone contact between the upper and lower bone segments are not absolute numbers. Usually the horizontal movement is greater than the amount of vertical lengthening needed in most patients and this does not pose any restrictions from so doing.
The ability to make this simultaneous two-dimensional chin augmentation change is an historic advantage of a bony genioplasty over that of an implant. While some argue that a chin implant can be positioned lower on the bone to create this effect, this effect is limited and such implant positioning is potentially unstable. How much vertical elongation and horizontal projection can be combined and still maintain some bone contact between the upper and lower bone segments are not absolute numbers. Usually the horizontal movement is greater than the amount of vertical lengthening needed in most patients and this does not pose any restrictions from so doing.

 The chin osteotomy can also be done as an isolated vertical lengthening which is indicated when the lower third of the face is disproportionally deficient even if adequate chin projection exists. Just like cutting the chin bone and moving it forward, it can also be cut and vertically lengthened. Also known as an opening wedge bony genioplasty, the chin is opened with the back ends of the osteotomy line acting like a hinge. It is held in its lowered position by a small spanning titanium plate with screws. While it can be vertically lengthened by any amount, it usually takes up to 8 to 10mms to see a significant external chin lengthening change. With a bony gap of up to 10mms, I prefer to graft that gap to allow for maximal bone healing between the superior and inferior bony chin segments. This is most needed in the central area where the gap distance is the greatest. Graft options include tissue bank solid or corticocancellous bone particles.
The chin osteotomy can also be done as an isolated vertical lengthening which is indicated when the lower third of the face is disproportionally deficient even if adequate chin projection exists. Just like cutting the chin bone and moving it forward, it can also be cut and vertically lengthened. Also known as an opening wedge bony genioplasty, the chin is opened with the back ends of the osteotomy line acting like a hinge. It is held in its lowered position by a small spanning titanium plate with screws. While it can be vertically lengthened by any amount, it usually takes up to 8 to 10mms to see a significant external chin lengthening change. With a bony gap of up to 10mms, I prefer to graft that gap to allow for maximal bone healing between the superior and inferior bony chin segments. This is most needed in the central area where the gap distance is the greatest. Graft options include tissue bank solid or corticocancellous bone particles.
Sliding Genioplasty + Chin Implant Combinations (Extraordinary Chin Augmentation)
Extraordinarychin augmentation is defined as when the dimensional changes needed exceed whatever is possible using standard performed chin implants or within the bony contact limits of a bony genioplasty. As a result extraordinary chin augmentation requires either combining an implant with a sliding genioplasty or the fabrication of a custom chin implant.

 While a bony genioplasty and a chin implant are typically perceived as completely independent procedures, there is no biologic reason they can not be combined if the patient’s dimensional needs so require. Having done many such combination chin surgeries it has not shown any increased risks of complications behind what whether procedure alone has. The key is to make the bony genioplasty the workhorse of the procedure to keep the ‘implant load’ low on the tight tissues of the overlying soft tissue chin pad.
While a bony genioplasty and a chin implant are typically perceived as completely independent procedures, there is no biologic reason they can not be combined if the patient’s dimensional needs so require. Having done many such combination chin surgeries it has not shown any increased risks of complications behind what whether procedure alone has. The key is to make the bony genioplasty the workhorse of the procedure to keep the ‘implant load’ low on the tight tissues of the overlying soft tissue chin pad.
Sliding Genioplasty in Obstructive Sleep Apnea

 A sliding genioplasty can also be one type of surgical treatment for obstructive sleep apnea (OSA). Because the genioglossus muscle is attached to the back part of the chin, a sliding genioplasty is one technique for genioglossus muscle advancement if the aesthetics of the chin is favorable to a large horizontal chin movement. By moving the chin bone forward with the genioglossus muscle, there will also be some forward movement of the base of the tongue if the bony chin movement is significant enough (10mms or greater).
A sliding genioplasty can also be one type of surgical treatment for obstructive sleep apnea (OSA). Because the genioglossus muscle is attached to the back part of the chin, a sliding genioplasty is one technique for genioglossus muscle advancement if the aesthetics of the chin is favorable to a large horizontal chin movement. By moving the chin bone forward with the genioglossus muscle, there will also be some forward movement of the base of the tongue if the bony chin movement is significant enough (10mms or greater).
When obstructive sleep apnea is severe, maxillomandibular advancement is the most effective method of enlarging the nasopharyngeal airway. Often these forward bone movements need to 7mm to 10mms of both jaws coming forward. If the entire lower jaw is initially short enough, a sliding genioplasty can be combined with a maxillomandibular advancement to open up one’s airway as much as is surgically possible.
CHIN REDUCTION
Chin reduction, while less commonly performed than chin augmentation, is also an important form of chin reshaping surgery that can improve one’s profile. It involves changing the size and possibly the shape of the chin in order to make it appear smaller. It is far more commonly performed in females than in men. It is beneficial to those who have a large chin that looks disproportionate large compared to the upper two-thirds of the face. A chin may look too large in two dimensions, either being too long vertically or projecting too far forward horizontally. In some cases, both dimensions of the chin may be enlarged but usually one dimension is largely at fault.
All chin reduction methods require careful attention to how the bone is taken down and how the soft tissues surrounding the reduced bone are managed. If the soft tissues are stripped off the bone and the bone underneath them reduced in size, do not expect the soft tissues to reattach and shrink down in size. The soft tissue chin pad has limited ability to become less in size through soft tissue contraction. Because it is stretched over a bony projection the soft tissue chin pad has a tendency to ‘ball up’ rather than lay down smoothly over a reduced chin bone size.

 For horizontal chin reduction it is tempting to use an intraoral approach and just burr down the front of the chin. But this is often ill-advised and is a potential cause of soft tissue chin ptosis. The soft tissue chin pad may simply falls slide off of the reduced bone. At the least if this approach is taken for a small reduction of a few millmeters, a strong mentalis muscle resuspension is needed for chin ptosis prevention. The safest and more effective technique for more significant horizontal chin reductions is a submental approach. Through an incision underneath the chin, the bone is exposed and the desired amount of excess bone removed. Because the attached soft tissues have had to be stripped off of the bone, they must be reattached tightly or sagging (witches chin deformity) will occur afterward. Excess muscle and skin are removed and sutures are used to reattach them tightly around the reduced chin bone. In essence a submental tuck is performed as part of the bony chin reduction.
For horizontal chin reduction it is tempting to use an intraoral approach and just burr down the front of the chin. But this is often ill-advised and is a potential cause of soft tissue chin ptosis. The soft tissue chin pad may simply falls slide off of the reduced bone. At the least if this approach is taken for a small reduction of a few millmeters, a strong mentalis muscle resuspension is needed for chin ptosis prevention. The safest and more effective technique for more significant horizontal chin reductions is a submental approach. Through an incision underneath the chin, the bone is exposed and the desired amount of excess bone removed. Because the attached soft tissues have had to be stripped off of the bone, they must be reattached tightly or sagging (witches chin deformity) will occur afterward. Excess muscle and skin are removed and sutures are used to reattach them tightly around the reduced chin bone. In essence a submental tuck is performed as part of the bony chin reduction.
 A chin that is too vertically long can be shortened by a wedge ostectomy of the chin. Through an intraoral approach, the chin bone is exposed and a reciprocating saw is used to remove a horizontal wedge of bone of the desired thickness. Usually it takes at least 5 to 6mms of bone removal if not more to make a real noticeable difference. Small plates and screws are used to hold the shortened chin bone together so that it can heal. The edges of the upper bone cut must be smoothed so it is not able to be felt through the skin. An alternative approach is an inferior border ostectomy done through a submental incision. This can also narrow the chin by lateral ostectomies as well. Good muscle resuspensions and soft tissue excision is the key to a successful outcome with this ‘down under’ technique. This is a good approach if there is already an excess of soft tissue tissue over the chin prominence on the underside of the chin.
A chin that is too vertically long can be shortened by a wedge ostectomy of the chin. Through an intraoral approach, the chin bone is exposed and a reciprocating saw is used to remove a horizontal wedge of bone of the desired thickness. Usually it takes at least 5 to 6mms of bone removal if not more to make a real noticeable difference. Small plates and screws are used to hold the shortened chin bone together so that it can heal. The edges of the upper bone cut must be smoothed so it is not able to be felt through the skin. An alternative approach is an inferior border ostectomy done through a submental incision. This can also narrow the chin by lateral ostectomies as well. Good muscle resuspensions and soft tissue excision is the key to a successful outcome with this ‘down under’ technique. This is a good approach if there is already an excess of soft tissue tissue over the chin prominence on the underside of the chin.
 The shape of the chin in the front view is affected by both its width and vertical length. While men may want a more broad or square chin, women often want a more narrow one. Female chins are often considered more attractive if it has a more narrow or V-shape to it. This can be done through isolated lateral ostectomies (tubercle reduction) or as part of a sliding genioplasty procedure through a central wedge resection technique.
The shape of the chin in the front view is affected by both its width and vertical length. While men may want a more broad or square chin, women often want a more narrow one. Female chins are often considered more attractive if it has a more narrow or V-shape to it. This can be done through isolated lateral ostectomies (tubercle reduction) or as part of a sliding genioplasty procedure through a central wedge resection technique.

 The most challenging of all chin reductions is one that requires a 3D dimensional reductive change. The combination of horizontal, vertical and width bone reductions challenges the enveloping soft issues to adequately shrink down around the extensively reduced bone. For this reason the submental approach is preferred so the resultant soft tissue excess can also be addressed as well.
The most challenging of all chin reductions is one that requires a 3D dimensional reductive change. The combination of horizontal, vertical and width bone reductions challenges the enveloping soft issues to adequately shrink down around the extensively reduced bone. For this reason the submental approach is preferred so the resultant soft tissue excess can also be addressed as well.
Chin Ptosis Correction
Sagging soft tissues of the chin, also known as a witch’s chin deformity or chin ptosis, is the result of a loss of attachments. One cause is that of aging, particularly in the person who wears dentures, where the jawbone has resorbed down to the point of loss of the upper mentalis muscle attachments. In the younger patient, however, the most common reason is that of prior chin implant removal or bony chin reduction. (particularly if done by an intraoral bone burring technique.
Correction of the witch’s chin (chin ptosis) requires the resuspension of chin tissues onto the bone or the removal of the overhang and a submental tuck. In the aged chin, in particular, the amount of chin projection is usually satisfactory. It is a matter of improving the soft tissue attachments to the bone. While I have done numerous types of intraoral soft tissue resuspension techniques, the long-term success of that procedure in my hands has not been good. It is such more successful if some chin augmentation is needed as the implant provides a shelf of support.

 Otherwise I prefer a ‘down and under’ approach of removing loose skin and muscles from a submental incision and tightening it on the underside of the chin. (submental tuck-up) That is much more predictable because it removes what is loose rather than trying to suture it back up.
Otherwise I prefer a ‘down and under’ approach of removing loose skin and muscles from a submental incision and tightening it on the underside of the chin. (submental tuck-up) That is much more predictable because it removes what is loose rather than trying to suture it back up.
The chin ptosis that occurs from an implant removal poses different considerations. Does the patient still want increased chin projection or not. If not, a submental tuck-up approach is done. Often a scar already exists under the chin and it is merely lengthened a bit. If more chin projection is still desired and the patient is equivocal about other implant, then a bony genioplasty may be done. The bone is moved (which helps support the sagging soft tissues) and the mentalis muscle and chin tissues is reattached on top and behind it to the fixation plate that is used. A chin implant can still be used in this case but a limited submental tuck-up will likely still be needed.
LABIOMENTAL FOLD REDUCTION
The labiomental fold,is the horizontal indentation or crease below the lower lip. It is caused by the insertion of the mentalis muscle on the upper chin bone and corresponds to the depth of the intraoral vestibule on the inside of the lower lip. It is a fixed anatomic point whose most frequent relevance is in how it is perceived after chin augmentation. Regardless of the method of horizontal chin augmentation it is an unavoidable consequence that the labiomental fold is going to appear deeper as the soft tissue chin pad beneath it moves forward. How much ut may appear deeper depends on the magnitude of the horizontal chin augmentation. Only vertical chin lengthening or combined vertical-horizontal chin movements (45 t0 90 degree lengthening) can leave the labiomental fold depth unchanged.

 Labiomental fold reduction can be done by a variety of volume addition techniques provided that the shape of the fold is a broad concavity. Injectable fillers and fat, and even implants (lip implant), are the most frequently used methods. Such injections can be concurrently done with any of the chin augmentation or reduction surgeries.
Labiomental fold reduction can be done by a variety of volume addition techniques provided that the shape of the fold is a broad concavity. Injectable fillers and fat, and even implants (lip implant), are the most frequently used methods. Such injections can be concurrently done with any of the chin augmentation or reduction surgeries.
However when the depth/shape of the labiomental fold is inverted injection technique are not going to push it out. This requires a complete release of the fold and a larger volume displacement method of which an introra, approach for the subcutaneous placement of a dermal-fat graft works best.
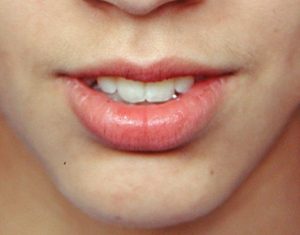
CHIN DIMPLE AND CHIN CLEFT SURGERY
Dimples and clefts of the chin are the only surface contour features of the soft tissue chin pad which are frequently confused. A chin dimple is a circular indentation in the center of the chin pad. Conversely a chin cleft is a vertical groove in the chin pad located at its lower edge. Such dimples and clefts can be slight in appearance or remarkably deep in others. Both appear much more frequently in men than women but only occur in the minority of the population. They are the result of a soft tissue defect and not due to a deformity of the underlying chin bone.

 Some would like their chin dimples and clefts to be reduced which are most commonly requested by females. The reduction of any chin dimple or cleft can usually be effectively done with the placement of injectable fillers or fat provided it is not excessively deep or inverted. The contour of the indentation will determine they effectiveness of an injection technique. A shallow concise shaped skin indentation responses well to injected volume displacements. Inverted dimples and clefts (v-shaped)( are more resistant to injection methods and require release and interpositional fat grafting, often with overlying skin closure particularly in chin clefts.
Some would like their chin dimples and clefts to be reduced which are most commonly requested by females. The reduction of any chin dimple or cleft can usually be effectively done with the placement of injectable fillers or fat provided it is not excessively deep or inverted. The contour of the indentation will determine they effectiveness of an injection technique. A shallow concise shaped skin indentation responses well to injected volume displacements. Inverted dimples and clefts (v-shaped)( are more resistant to injection methods and require release and interpositional fat grafting, often with overlying skin closure particularly in chin clefts.

 The creation of chin dimples and clefts can be done and requires tissue removal and skin fixation into the resected site. There are indications for doing so with both an intraoral and submental approaches. A chin dimple is created by an intraoral removal of a core of soft tissue underneath the desired dimple site with percutaneous skin fixation.
The creation of chin dimples and clefts can be done and requires tissue removal and skin fixation into the resected site. There are indications for doing so with both an intraoral and submental approaches. A chin dimple is created by an intraoral removal of a core of soft tissue underneath the desired dimple site with percutaneous skin fixation.

 Because of the more inferior location of chin clefts, a submental technique is needed. From this approach the vertical wedge of soft tissue is removed and the overlying skin sewn down to the bone. It is not necessary in isolated cleft creations to make a groove in the bone. When done in conjunction with implant augmentation it is necessary to remove a wedge of the implant to get to the bone for soft tissue fixation. This technique produces a subtle or shallow vertical cleft. For deeper vertical clefts an external excisional approach is needed which placed a fine line scar in the depth of the cleft.
Because of the more inferior location of chin clefts, a submental technique is needed. From this approach the vertical wedge of soft tissue is removed and the overlying skin sewn down to the bone. It is not necessary in isolated cleft creations to make a groove in the bone. When done in conjunction with implant augmentation it is necessary to remove a wedge of the implant to get to the bone for soft tissue fixation. This technique produces a subtle or shallow vertical cleft. For deeper vertical clefts an external excisional approach is needed which placed a fine line scar in the depth of the cleft.
AESTHETIC CHIN SURGERY Summary
Reshaping of the chin can be done by a wide variety of implant, bony changes and soft tissue suspensions/reductions. When choosing the chin shaping technique, a 3D approach to the problem and the procedure needed to treat it should be done and not rely on just a profile view alone. Implants, bony genioplasty and their combination can address any primary or secondary chin augmentation need. Bony genioplasty is an essential technique for most chin reductions. Soft tissue chin pad suspension or reduction can be part of a chin reduction technique or in the isolated treatment of chin ptosis. The soft tissue features of the labiomental fold and chin dimples and clefts can be adjusted using soft tissue excisional and fat grafting techniques.
In addition to helping chin augmentation / chin implant patients, Dr. Barry Eppley also offers a variety of surgical and non-surgical treatments for the face. He helps face lift, rhinoplasty and Botox patients achieve their desired facial contour. He is also a trusted cheek implants and custom implants provider.
Chin Augmentation – Before Surgery
The origin of the chin shortness is determined by looking at the face and neck as well as the position of the teeth. In the younger patient with a severe overbite (lower teeth behind the upper teeth), the chin position may be a reflection of an overall shorter jaw. In these patients, other treatment options may be considered (jaw surgery). Computer imaging in the profile view is extremely helpful in determining the value of chin advancement and how much advancement would be beneficial. In some cases, an x-ray in profile may be useful to look at the bone and the facial profile for treatment planning.
Chin Augmentation – Operation
Most chin implants are placed under IV sedation or general anesthesia as an outpatient. They are commonly placed through a very small skin incision under the chin where the bone is easily reached. Placing the implant through a small incision inside the mouth behind the lower lip can also be done. Chin bone advancement is always through an incision in the mouth where the bone is cut, brought forward, and fixed into its new position with a small plate and screws. Often times, chin procedures are part of other facial procedures including nose surgery and facelifts.
Chin Augmentation – After Surgery
A chin strap is usually used after surgery to control swelling and help the overlying tissues adapt to the implant or bone. Bruising is rarely seen but swelling is common. Sutures inside the mouth are dissolvable and do not need to be removed. Sutures in the skin under the chin are removed in one week.
Chin implants are extremely well tolerated and infection is very rare. When the chin bone is moved, there is usually a short period of lower lip numbness which completely resolves by one month after surgery.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237