How Can A Custom Skull Implant Be Designed To Include The Forehead, Brows and Temporal Areas?
Q: Dr. Eppley, I am interested in your skull reshaping procedures. I am a young male, and the shape of the upper third of my skull can be described as narrow. Specifically, my frontal bone is narrow. This includes my supraorbital rim, my forehead, and the very top of the frontal bone which forms the top of the skull.
So I want to widen this area. I envision a customised implant broadening the supraorbital and the very top of the lateral orbital rim; through to forehead widening; and finally a widening of the top of the skull. In order of priority; the most important aspect for me is the supraorbital rim, because this frames the eye area.
The second aspect of my frontal bone is that is quite rounded and feminine. What I mean by this is that the lateral areas of the frontal bone sit too far back relative to the centre of the frontal bone. In other words, the sides of the frontal bone ‘fall away’ too much, which is a feminine aesthetic. Masculine frontal bones have a much smaller discrepancy between the anterior position of the centre of the frontal bone, and the anterior position of the lateral portion of the frontal bone.
I know that this procedure is theoretically possible, but I anticipate several issues, which I will now enumerate:
1) How does one widen the frontal bone beyond the anterior temporal lines without creating problematic aesthetic issues? What needs to be done to accomplish this, without it looking unnatural? Surely the position of the temporalis muscle is a limiting factor here?
2) How does one compensate for the concavity that will be created in the temporal area? If the brow and forehead are widened, with the temporal area remaining the same; there will be a visible concavity in this area which may look unnatural
3) If a combined temporal-frontal bone implant is used, how does one maintain the natural delineation between these two areas? Blending the two regions into one monolithic region would be an aesthetic limiting factor for me, because the majority of people have some visible distinction.
4) I believe in an aesthetic that preserves the harmony between the width of the various facial structures. Observing many aesthetic faces, there is usually no issue if the zygomatic bone is wider than the mandible or maxilla. However, the relative widths of the frontal bone and the zygomatic bone is usually a significant factor. In my opinion, that is because the two bones are directly connected at the lateral orbital rim. Widening just the frontal bone here would create disharmony between these two bones. So I am interested in your opinion regarding concomitant widening of the entire lateral orbital rim and the zygomatic bone (chiefly the zygomatic arch and the part of the zygoma just beneath the eye). In your experience, would this be aesthetically feasible, and what issues might you anticipate with this?
I do apologise if I have taken up your time with these questions. Understanding these issues in detail is crucial for me to consider getting this custom skull implant, and I hope you can help me out here.
Thanks.
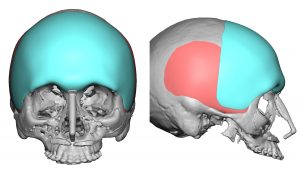
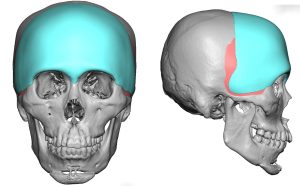 A: Thank you for your inquiry and your very articulate and intellectual description of your aesthetic head shape concerns, objectives and the aesthetic challenges that come with trying to rectify them all in a proportionate and harmonious manner. I will answer your questions in detail but have attached a few prior patient custom skull implant designs in the spirit of ‘a picture is worth a thousand words’ that have addressed similar patient concerns.
A: Thank you for your inquiry and your very articulate and intellectual description of your aesthetic head shape concerns, objectives and the aesthetic challenges that come with trying to rectify them all in a proportionate and harmonious manner. I will answer your questions in detail but have attached a few prior patient custom skull implant designs in the spirit of ‘a picture is worth a thousand words’ that have addressed similar patient concerns.
1) Any implant design that needs to go past the bony temporal line will sit on top of the temporalis fascia/muscle.
2) Depending upon how much the implant design crosses the temporal and how much forehead width and frontal augmentation is needed, the implant design may have to cover the anterior temporal region to prevent creating unaesthetic temporal hollowing.
3) In men you design as part of the implant a temporal line of transition between the forehead and the temporal area. (subtle raised ridge) In women this is not necessary.
4) While you can extend an implant design down along the lateral orbital rim and cover the temporal area as well, you can not cross onto the zygomatic arch. There are rigid attachments of the periosteum of the zygomatic arch over which courses the frontal branch of the facial nerve. Elevating this periosteum off of the zygomatic arch will injure that nerve and cause permanent paralysis of the forehead muscle elevators which are responsible for eyebrow movement. As a result any augmentation of the zygomatic arch must be done with a separate implant from a different point of access.
Dr. Barry Eppley
Indianapolis, Indiana



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237