Your Questions
Your Questions
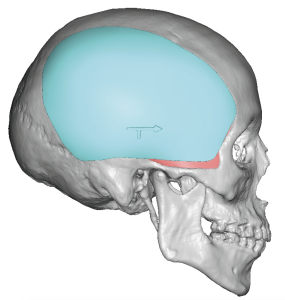
Q: Dr. Eppley, my surgeon told me about Dr. Eppley, that he could possibly help me with my jaw asymmetry. I have hemi-mandibular hyperplasia on the left side. I attached a photo I took of one of my x-rays. I was wondering if it was even possible to “move” the “hole” on that side of my jaw, the mental foramen? Its placement is so low that a previous doctor couldn’t shave off enough bone to make it even with the other side. That is the after x-ray of when I had my jaw shaved. He was only able to shave off a few millimeters. Thanks for your help,
A: Like all mandibular hyperplasias all structures in the elongated side are lower, most pertinently the intrabony course of the inferior alveolar nerve whose exit from the bone is the hole to which you refer (aka mental foramen). The course of the nerve in the bone and the mental foramen are fixed structures that can not be moved unless one can accept permanent numbness of the lower lip on that side…which I doubt would never be a good tradeoff.
The key to attempting inferior border reduction on the elongated side is a preoperative 3D CT scan with nerve imaging from which the exact amount of bone that can be safely removed can be determined. ‘Eyeballing’ or guessing in surgery what is safe to remove is not the most effective strategy. Even by guessing what I think can be removed (see attached picture) it is more than just a few millimeters.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got jaw and cheek implants (and a genioplasty) and they made me look like I gained weight by pushing my masseter muscle or cheek fat out. It is especially prominent when I smile. Can this be fixed without replacing the implants? I’ve had one surgeon suggest buccal fat removal and another suggest a masseter shave. I also believe I have masseter dehiscence on one side which may be exacerbating the issue.
A: Thank you for your inquiry and sending your pictures to which I say the following:
1) Since surgical procedures are done in the static mode (non-smiling) there is no way to predict before surgery as to what the aesthetic outcome may be.
2) That being said you were less than an ideal candidate for jaw angle implants but the design that was chosen was bound to create the exact effect you now have. (round and heavy) That is not a jaw angle implant design I would ever use as its round and high shape has its greatest effect on pushing out the central muscle mass. Such implant designs are great examples of the material chosen for the implant (metal) is design limited. A big round jaw angle implant in your facial shape has done what could be predicted.
3) While I could tell much from a single front view smiling picture, the placement of rigid metal implants in the jaw angle area has increased risks of postoperative masseteric muscle dehiscence.
3) While you had a vertically short chin and a more flat mandibular plane angle choosing to vertically elongate the chin by a lengthening bony genioplasty was an appropriate treatment selection. But in the face of jaw asymmetry (left side longer than the right) it is not clear why your external result is what it is. I would need to see static before and after pictures to provide a more definitive answer, as well as a postop 3D CT scan, to provide a more definitive answer to that question.
4) In regards to your cheek implants that is a classic example of choosing an implant design that is not best for your face and, quite frankly, is not best for most male faces. In fuller face in particular a high cheekbone implant design is best to avoid increasing sub cheekbone fullness.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I previously had double jaw surgery and V-line surgery that I regretted. After that, I underwent reversal double jaw surgery and received a custom jawline implant to restore my appearance, based on my before-and-after surgery CT scans. These procedures improved my appearance and reversed the changes to a certain extent, but my face still isn’t exactly the same as it was before. Does this mean that even with CT scans and a custom jawline implant, my appearance can never be fully restored to how it used to be?
A: There is a lot of information about your case I do not know but as a general statement,it is fair to say you can never go completely back home. It doesn’t matter how close you get the bone to it’s original state there are irreversible changes to the soft tissues from the surgeries that can never be completely overcome.,
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q:Dr. Eppley, I underwent bilateral implant placement earlier this year with Torosa medium-sized saline implants while retaining my native testes. Although congenitally undersized, the native testes remain functional. The current implants have not provided full displacement, resulting in a persistent “three-ball” appearance and asymmetry. I’d like to discuss surgical options to correct this mechanical issue and achieve a more natural, balanced result through larger implants.
A: With essentially the same size implants to that of your natural testicles the inability to hide your natural testicles would be expected. You are going to need custom implants that are certainly larger than the maximum standard 5.0cm testicle implants are currently available.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For the plastic surgery as Temporal Arteries Ligation, how much time it takes to get the surgery done, and what is the recovery time.
- How many days do I have to stay in the USA, If there is a return consultation, or am I able to leave as soon as the surgery is done.
- Once the procedure is done, does it last forever, or the arteries becomes to appear again and naturally with time.
A: 1) 1.5hrs, there is no real recovery from a physical limitation standpoint.
2) You can return home the next day.
3) The long term results are fairly stable, few patient ever develop any recurrences.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hey, I wanted to consult on an eye procedure performed by a Turkish surgeon. He performs a procedure called “bella eyes” which is essentially an endoscopic dynamic technique canthopexy with a brow/temple lift. Access is made through two incisions in the hairline, allowing the surgeon to have access to the deeper tissues and muscles with an endoscope.
These are the results I favor I haven’t seen results close to this with a normal cantho. I feel like the lift the surgeon performs essentially streches out the outer corner of the eye. Problem is, these patients had a negative tilt. i have a neutral/positive tilt, i want to keep it neutral but just stretch it out/elongate it more. The surgeon insists on having a lift. I was wondering if Dr. Eppley could essentially perform a “lift”, but rather doesnt lift it but rather streches it out more horizontally. I want to prevent too much uplift because my tilt is already desirable and tilting it up even more may look uncanny.
A: That procedure works because of the lift, not so much from the lateral canthopexy. No form of a lateral canthopexy can stretch out the eye corner laterally without the lift so shown.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley I’ve had a rhinoplasty with tip rotation before etc., which made me happy with the tip, however i have a problem that my nose is too long, the distance between the end of my nose (alar base, nostrils?, alar rim) and the top of my lip is too short, i like my lips the way they are and don’t want to change anything about them. Now to my question, is it possible to position the nostrils higher up on the face? like literally reposition them higher by 1.5-2mm? When I lift the skin above them the nostrils follow up to the exact position I want them in, and i guess the tip of the nose could be adjusted again, I have never seen this happen in a rhinoplasty or even in reconstruction or repositioning cases of the nostrils or alar base, which is why I‘m asking. I have included example photos of a hypothetical before and after. Thank you for your time and I hope to hear back from you soon!
A: While the nostrils can be lowered ny skin removal from the upper lip, the nostrils can not be raised without adding skin or removing part of the lower nostrils.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Hi, I am seriously interested in skull reshaping. As i have suffered mentally with the shape of my head for almost all my life and I am now 40. I wondered what would be the best option in terms of implant’s to the sides of the head just behind and above the ears. My head is small and narrow in this area and I would like to increase the sides width to have a more wider head. I don’t think it would need much, I have fairly short hair which I tend to fluff the hair a little above the ears to make it look a bit more normal. So in short I have a small and narrow head particularly just above the ears.
 A: Thank you for your inquiry and sending your pictures. By your desccription and pictures you are describing head widening or submuscular temporal implants. (see attached implant design example) They are placed from an incision in the crease of the back of the ear which heals inconspicuously. The usual widths are 5 to 7mms which would certainly be consistent with ‘not needing much’.
A: Thank you for your inquiry and sending your pictures. By your desccription and pictures you are describing head widening or submuscular temporal implants. (see attached implant design example) They are placed from an incision in the crease of the back of the ear which heals inconspicuously. The usual widths are 5 to 7mms which would certainly be consistent with ‘not needing much’.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had fat graft to the chin a year ago and totally dislike the result. And was wondering if there is a way to reverse this. So my concern is at i had graft directly to the chin. And now it looks really ugly, like it protrudes my lips and nose and make my chin have a round balloon shape.
A:There is not. Once fat is in the soft tissue chin pad it can not be reversed. And don’t try liposuction as that will only make the problem worse. You will simply turn a round balloon shape into a round and irregular/non-smooth balloon shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, on first glance do i look like the right candidate for infraorbital rim implants and fat grafting around upper and lower eye area? for an overall fully harmonised face as i think that area slightly breaks harmony.
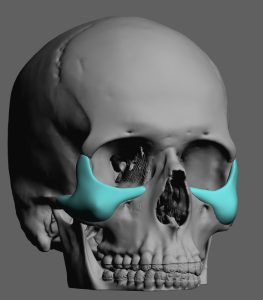 A:Thank you for your inquiry and sending your pictures. When you have a significant orbital rim skeletal deficiency fat grafting has no role in its augmentation. This requires a custom infra lateral orbital rim design to provide adequate augmentation to treat what is a 3-D orbital rim recession. Fortunately you have fairly good lower eyelid position although a spacer graft of the lower lid would be helpful to extend the augmentation as highest possible up to the lash line where implant cannot reach.
A:Thank you for your inquiry and sending your pictures. When you have a significant orbital rim skeletal deficiency fat grafting has no role in its augmentation. This requires a custom infra lateral orbital rim design to provide adequate augmentation to treat what is a 3-D orbital rim recession. Fortunately you have fairly good lower eyelid position although a spacer graft of the lower lid would be helpful to extend the augmentation as highest possible up to the lash line where implant cannot reach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Just a question…what’s the different between solid silicone to PMMA for augmentation of the head?
A: For aesthetic onlay skull augmentation PMMA vs Custom Silicone implants are the two options which have the following properties:
 PMMA Bone Cement
PMMA Bone Cement
- moldable putty created in surgery which sets into a rigid plastic material in 10 minutes
- once set it is unchangeable in form
- must be shaped blindly once placed under the scalp thropugh small scalp incisions…as a a result prone to asymmetries and edge irregularities
- controlled shaping of the material can only be done through an open coronal scalp incision
- can only be placed on bone, can not cross the bony temporal line onto the muscle
- limited skull augmentation effects (60ccs or less in volume)
- can not be revised secondarily, must be fractured and removed
- lower material cost
 Custom Skull Implant
Custom Skull Implant
- preformed shape by 3D custom design process
- can be modified intraoperatively if needed I(rare)
- can be placed on bone as well as muscle permitting large surface areas of coverage
- more significant skull augmentation effects (100cc to 300cc volumes)
- easily removed, modified and/or replaced
- higher material cost
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a consult with a maxillofacial surgeon early next month. Even with this, I feel my midface will remain flat. Is there anything that can be done for this region post double jaw surgery?
A: This is a common issue even after DJS. This is the role of custom midface implants, whether that be as a total mask or cheek/paranasal implants, which cabn provide the additional projection which the bone movement ca. not create. For some midface deficient patients the role of DJS is to ultimately lessen the volume load of implants needed if they can not eliminate their need completely.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had an Intraoral chin reduction in 2023 & am seeking a way to tighten up the excess skin left after my surgeon burred down 6mm of bone. After my surgery I now experience sagging skin on my chin that I didn’t have before. I wasn’t happy with the look of the skin on my chin after the surgery so my surgeon did a submental chin tuck in office, but I still feel like there’s skin sagging. I do have a scar underneath my chin. Would I still be able to get a submental chin “tuck” with a previous scar? I’m not exactly interested in more bone work being done, or getting a secondary chin reduction because the first time I was disappointed. I attached a photo of a Lateral Ceph taken this year. This Xray was done 2 years after the surgery.
A: The intraoral chin reduction you had produced exactly the outcome one would expected when its bone support is reduced….an excessive /droopy soft tissue chin pad. The submental chin tuck was the appropriate solution but it was inadequate because it was under done. Since you already have the a submental scar there woild be no reason to not take advantage of it and have a second submental soft tissue reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like a consultation to address moderate skin laxity (mainly due to aging) on my lower buttocks. I am not interested in implants. I’m interested in subgluteal excision and/or spiral thigh lift. or a combination of both. I have spent more money than I care to think about on Morpheus 8, Emsculpt and Radiesse fillers all of which did little to nothing to help. I am too thin for a BBL.
A: Thank you for your inquiry and sending your picture. The only effective for a lower buttock tissue overhang with a defined infragluteal crease is excision. It can be lifted away with an implant, reduced by liposuction or improved by any form of transcutaneous energy-based device treatments for skin tightening or fat reduction. The tradeoff for the definitive treatment is the infragluteal scar.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Im interested firstly in jaw side reduction as I have squared jaw I wanted to the sides to be shaved a bit to reduce that bulkiness and for more symmetrical face while keeping the masculine look.I know its not common for men to reduce their jaws but i feel mine is too big and doesn’t fit my face I need a slimmer jaw while keeping the masculine look.
A: You are referring to a lateral corticotomy of the ramus of the lower jaw, often referred to as jaw angle shaving. The shape of the ramus remains the same but the thickness of the bone is reduced 40% – 50%. The procedure is performed through an intraoral approach under general anesthesia as an outpatient.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello,I was obese for most of my life. In the last 2 years I have lost over 90lbs and am just a few pounds away from my goal weight. Being obese all those years pushed against my xiphoid process and now that the weight has been lost it protrudes a lot, sticking out further than my chest and stomach. I believe the procedure I need is called a Xiphoidectomy.
A: Thank you for sending your pictures. That is an impressive xiphoid prominence, one of the most impressive I have seen. It can be treated by removal (xiphoidectomy) or xiphoid infracture (xiphoid osteotomy). In most cases the xiphoidectomy is done. In more uncommon cases due to an adherent attachment of the diaphragm and ossification of the cartilage an infracturing may be performed with plate fixation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my skull has been misshaped since birth; the exact reason has never been medically diagnosed. Once delivered, I had a bruise on cheek, swelling, and head shape that was not symmetrical that the doctors said would fix itself as I aged. My inquiry is in regard to a custom implant for the “flat side” and skull reduction for the side that bulges. I had a surgeon look at the possibility of a custom implant, but he was uncomfortable with skull shaving since that was not his expertise.
A: Thank you for your inquiry and sending your picture and 3D CT scan. Yours is certainly not the typical plagiocephaly which is a common cause of flatness on one side of the head and a protrusion on the other side. Regardless of the cause the approach of custom implant augmentation on the flat side and bony reduction on the protrusive side would be a logical approach to which I would makle the following two comments:
1) When designing a custom skull implant that crosses over the bony temporal line onto the side of the head you have to factor in the thickness of the temporal muscloe which sits on the bone in that area. If not one can inadvertently make the flatter side more full than the protrusive side.
2) When considering bony reduction of a protrusive skull area considerations are how thick is the bone, how much bone thickness can be safely removed and what is the incisional tradeoff for what ajmount of bone removal. This is why it is important to do a color mapping bone thickness of the protruding area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to inquire about the procedure for custom wrap-around testicular implants. I currently have two testicles, each approximately 7 ml in volume. I previously underwent an unsuccessful procedure in which implants were placed in front of the testicles; however, they were later removed for aesthetic reasons.
A:In a scrotum that has prior surgery you are not a great candidate for the wrap around implant concept which has its own risks of postoperative implant disengagement from the testicles. That risk escalates considerably in prior implanted scrotums and those are risks I will not undertake.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I had a consultation with you about 5 years ago, and I’d like to follow up about a specific cranial contour plan. I’m interested in reducing or shaving down the frontal sides of my forehead (the areas that slightly protrude) and then adding volume to the back of my head to create a smoother, more balanced overall shape. Could you please let me know if this combination can be done in one procedure, and whether the occipital augmentation would be with a custom PEEK implant?
A:Good to hear from you again from five years ago. To specifically answer your skull reshaping questions:
1) the combination of side of the forehead reduction with occipital augmentation would be done as a combined single operation.
2) all forms of aesthetic head augmentation are done by the 3-D design skull implants. Almost all of these are composed of a solid silicone material as that offers the most precise design with feathered edges that can be placed with the smallest scalp incision. That feels just like bone when it is placed on bone. Custom PEEK is not a material that is FDA approved in the United States for any form of aesthetic craniofacial augmentation per the manufacturers. This is a different story in Europe and other places in the world. But even if it was available in the United States the cost to manufacture it would be four times higher than silicone and it would require a complete coronal scalp incision from ear to ear to place due to its inflexible construct. But even if f all of that was not a problem for the patient I still would not use it as it is not possible to manufacture PEEK with super fine feathered edges which is extremely important in skull augmentation as any rounded edges are eventually going to be felt in the shaved head patient are going to be seen.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My midface is a bit flat. Would I benefit from a LeFort 2 or 3 osteotomy?
A:There is no indication for you, or anyone seeking aesthetic mid face augmentation, for a LeFort 2 or 3 osteotomy Those are operations that look great on diagram but in real life are not appropriate for the aesthetic patient. They are indicated for the syndromic craniofacial patient who has real facial hypoplasia problems where the magnitude of the surgery and its potential risk and complications are more acceptable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I had a chin implant done last year It was an. Omnipore medium/square implant . Immediately after the surgery I noticed asymmentry. The surgeon then suspected it was swelling and did nothing. I can definitely feel it being higher on one side than the other. Tilted angle from the middle. The surgeon says that the asymmetry is too little to do a revision for and that the outcome of a revision with the additional scarring will be too uncertain and risky. A second opinion confirmed it being placed higher on one side, but said the same thing about the outcome of a revision being uncertain. They only offered to do lipofilling on the smaller side. What do you think? Is replacing the implant the best choice in the long run or is the surgery too risky. Around here there is not much expertise in this, certainly not in polyethylene materials. I thank you in advance for replying
A:Thank you for your inquiry and detailing your chin implant issues. Fundamentally I don’t think one should confuse ‘I don’t want to or can’t do it‘ as opposed to ‘it can’t be done’. Most surgeons are not too keen on revising their own work unless they are forced to do it based on the magnitude of the problem. While it is true that in the placement of chin implants perfect symmetry is certainly not always achieved and that, in and of itself, is not rare. The real issue is not whether chin implant asymmetry exist or whether it can be corrected but how much effort does the patient what to put into that pursuit and what risks does one want to take in doing so. Porous materials like Omnipore are great biologically due to the tissue in growth IF one never has to revise or remove it. It is not a great material when that is needed and that will occur in 40% of all chin implants that are placed. It is not a question of whether your chin implant can be operated on in an effort to try and achieve better symmetry. But it requires dissecting the implant out, removing it in its entirety and then reinserting it. Besides the trauma of so doing the likelihood that the implant can be explanted intact without fracturing is low and it is always prudent when implants of this material are revised to have a backup on hand to use, and one might make the argue that is better just to put in a new chin implant anyway. As you can now see when revising a facial implant of this material the tissue ingrowth is not an asset but a liability.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, From what I’ve read, the closest description of what I’m experiencing is dynamic chin ptosis – my chin only protrudes when I smile or speak. I’d like to reduce that movement and am considering starting with Botox. Could you please advise where you would recommend the injections be placed and approximately how many units may be needed? Thank you so much 🙂
A:This is not a problem in which I would recommend Botox injections as I don’t think it will have a positive effect. This is caused by a more global facial movement pulling back on the chin revealing and displacing the extra soft tissue chin pad tissues. In essence you would have to paralyze your whole smile to have an effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I believe I am a good candidate for the lower buttock lift with the incision to re-create the bottom gluteal fold in a higher position. I would like to find out if this procedure would make my buttocks look higher by removing hanging lower skin off of buttocks, would it also decrease saddlebag look on sides of thighs, what typical recovery is like,
A:Thank you for your inquiry and sending your pictures to which I can make the following comments:
1) the lower buttock lift would make the fold slightly higher but, most importantly it would remove the overhanging lower buttock tissue.
2) What you definitely do not want as to extend the scar beyond the lateral extent of the existing infragluteal fold. Thus the lower buttock lift by itself will not improve the saddlebags. This issue is better traded by concomitant liposuction.
3) Recovery from a lower buttock lift is primarily that of limiting activities in the first month after the surgery that placed undue stretch on the infragluteal fold incisional closure. This is primarily strenuous activities relating to working out and other associated activities were bending over is greater then 45°. Sitting initially is a bit of a challenge but that is overcome by having a sitting position that does not create a back and leg angle at 90°.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got my hairline advanced in Turkey roughly 2.-2.5cm. I currently am very unhappy with my results. I never really intended on having a hairline advancement nor was this on my radar. I just wanted my brow bone shaved and the surgeon recommended I do this as well.
I’m very interested in your clinic because I read about the use of ballon/tissue expanders I want my forehead raised atleast 1.0cm-1.5cm if the full inch isn’t possible to restore my facial balance and my masculine identity.
A:Thank you for your inquiry and sending your pictures. When the frontal hairline is lowered this is done by forehead skin removal. With loss of non-hair bearing forehead skin the only way to partially reverse it is to expand the existing forehead tissues to create more skin to be moved upward. I would doubt that a full inch is possible and a more realistic outcome is in the one centimeter plus range.
The concept of s the forehead tissue expander is that it is initially placed, expanded for six weeks at home by you and then allowed to rest for another six weeks before doing the reverse frontal hairline advancement. Trying to shorten that expansion process risks as100% relapse within the first 7 to 10 days after the procedure is completed. While effective I think the hardest part of it is you have to walk around for three months with an obvious and unusual looking forehead.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My main concern is that my brows sit a little high and give me a softer, more feminine look. Ideally, I’d like to lower or reshape them into a stronger, more masculine angle if that’s technically possible. If it’s not feasible, that’s okay too — I’d just like your expert perspective on whether downward repositioning or an alternative adjustment makes sense in my case.
A:Thank you for your inquiry and sending your pictures. Based on my assessment of them I believe what you have is hey differential brow shaped where the tale of the brow is higher than they medial or inner brow area. If the outer half of the brow was more even with that of the inner brow area then I think you would be more satisfied with their shape. Unfortunately there is no reverse brow lifting procedure which could differentially lower the outer half of the brow area. What I would recommend is to initially with eyeliner fill-in the lower half of the outer brow area and see what that looks like. If you find that change successful then you have the options of either micro pigmentation or, more ideally, eyebrow hair transplantation. Either approach would allow for a more controlled brow reshaping
.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I feel self conscious about my profile, specifically the maxillary area and the more downward grown midface. I want to achieve more skeletal support to have a more modelesque appearance. I don’t know what can be done . I feel specifically on profile, my jaw is more rotated down and back and goes at a bad angle. I don’t know what to do.
A:Thank you for your inquiry and sending your pictures. The pictures are not of the greatest quality to make an ideal assessment or do any imaging. But what they demonstrate as best as I could see is that you have a classic conundrum in terms of facial projection. You lack ideal forward projection of the midface and the mandible. This can either be addressed by double jaw surgery or implant augmentations. Each approach has its merits as well as its indications. The logical first approach’s to get an evaluation by a maxillofacial surgeon to determine whether double jaw surgery advancement would be beneficial and whether you want to go to that effort. You only consider implants when you have made the determination that double jaw surgery is either not indicated or it is simply not a surgical approach which you want to do.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a plastic surgeon from Beijing, China. I read with great interest your article published in ASJ on hip augmentation with implants (Evolving Clinical Experiences in Aesthetic Hip Implant Body Contouring) and truly admire your design of the prosthesis. I am also considering performing hip augmentation surgery with implants for my transgender patients.
I have a question and would like to seek your advice: Beyond the mid to long-term postoperative period (i.e., beyond 3 to 6 months after surgery), can patients perform movements such as deep squats, cycling, or yoga? Will they experience discomfort or even compromised stability of the implants? I suspect that when hip flexion exceeds 90 degrees, the deformation of soft tissues around the implant area may exert significant pressure on the prosthesis. I would appreciate your insights on this matter.
A:Thank you for your thoughtful inquiry. In terms of long-term outcomes from hip implants I have no concerns that the patient will experience discomfort or compromised stability of the implants in any type of physical maneuver. However what is more pertinent is that in some movements such as signifincat hip flexion it may be possible in thin patients to see some of the outline of the implant as the soft tissues change or stretch over the implant in different leg positions. This is, of course, an aesthetic concern and not a functional one. But it is important to point out preoperatively that this will likely occur and is not a rare or unexpected outcome. It is just the nature of putting an implant in an area where the soft tissue cover will change with dynamic motion while the implant form will remain the same.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Interested in a 2cm forehead reduction.
A:The amount of frontal hairline advancement that can be achieved is controlled by the natural elasticity of the scalp. as it is the entire that actually shifts forward in the procedure. There is no accurate predicting before surgery how much movement can be achieved. Whether that would be 2 cms is unknown but that amount would not be expected for most patients.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have what I believe to be chin ptosis from a chin implant I received last year. The dr kind of refused to acknowledge the problem and instead replaced the implant with a smaller one and the issue remains. Is this something Dr Eppley could address? I had consulted a different surgeon and he’d recommended an oral maxilofacial surgeon but I hope it’s chin ptosis that can be repaired.
A:You are referring to a submental chin pad excision/tuck which is the most effective to chin pad laxity…which is not uncommon after chin implant removal or chin implant downsizing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Are you all able to also to do 3D models how the person will look after the face implants? Thank you.
A:While the concept of creating custom facial implant designs on the patient’s 3-D skeletal model and then knowing exactly what the aesthetic outcome is would be extremely helpful. However that technology with any accuracy does not yet exist. There is yet no known precise correlation between the push of implants on the bone and exactly how anyone’s very different overlying soft tissues will respond. Currently custom facial implant designs are done based on the patients desired the preoperative changes on their pictures via prediction imaging which serves as a target for the design. This works very well for most cases provided the surgeon is a tremendous experience in doing custom facial implants And has a good feel for how to make designs have a certain aesthetic effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon