Your Questions
Your Questions
Q: Dr. Eppley, I’m 31 years old, I come from Poland, my problem is plagiocephaly. I have been looking for a solution to this problem for many years until I finally found your website. I’d have a few questions;
– on what basis do you create implants, is it a 3D computed tomography of the skull?
– is it possible to make such an implant to order so that I can perform the implantation procedure in Europe?
A: In answer to your skull implant for plagiocephaly questions:
1) You have correctly surmised that such skull implants are created by a 3D design process.
2) I only design and make implants in which I surgically place them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, 3 months ago I had ear reduction surgery, but I’m not entirely satisfied. My ears are still large, especially in proportion to my face. Could a second surgery improve the appearance of my ears?
A: I would agree that your ears are still a bit big because it is the concha that is the remaining largest part of the ear. While I do not know what exact ear reduction techniques were used the standard approach uses a high and low method which leaves the concha (central part of the ear) unchanged. Such an ear redeuction approach is very effective in many large ears, but in the large concha ear, it often leaves it still looking large and often disproportionate.
That being said you can not repeat the exact same ear reduction approach as the first time as the limits of that method have been reached. Changing to a central conchal reduction ear reduction technique is now what is needed if any further reduction in ear size is to be achieved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I went to South Korea for a genioplasty because I wanted a more narrow face as I felt my face was very circular and doing so achieved a nice front look but made me lose my side profile and cause extra loose skin kinda around giving me a bulge and double chin effect.
Really would like to get my side profile that is more western back if possible. Tried a facelift but it just didn’t work that well on tightening the skin.
A: The origin of the loose tissues around your chin is because the bone structure has been reduced and now there is too much soft tissue chin pad for the amount of bone that is there. This is not a real soft tissue excess, but an iatrogenic one, so it is no sjurprise that any form of a lower facelift could not improve the problem. (a very ill-conceived concept from the surgeon, that may help the jaw angle area but never the chin) The key to improvement is that some chin support has to be built back to pick up the loose tissues. Whether that its best done by adding some form of an implant or moving the chin bone requires that I see your postop x-rays so I can see what the modified chin bone looks like.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, . I have been following your work for years now since I am very unhappy with my lower jaw line. I had two surgeries, which in my opinion went very poorly. I have a strong chin asymmetry now, and a slight asymmetry of the jaw angles.I f inally found a new surgeon and a company to get PEEK wrap-around jaw implants in Germany. I wish I could get them at your institute, but considering the additional flight costs, hotel cost,… I probably won’t have enough money.
My question now is, if you would offer to help in designing the jaw implant? I would be very happy to get your insights about lateral and vertical projection of the jaw angles, what to pay attention in the chin area, etc.
I saw multiple before/after fotos of patients who got wrap-around implants by that surgeeon and I feel the results are lacking,
A: I only design implants in which I implant since there is a correlation between the implant design and the success in properly installing it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am French and I write to you because I would like to know if you perform surgeries for plagiocephaly in adults or if you could know a doctor who could do it.
A: Plagiocephaly corrections in adults are procedures that I commonly performed, typically custom implants fo rthe flat back of the head or on the forehead. Although there are other plagiocephaly procedures that can be performed as well besides these two most common ones.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
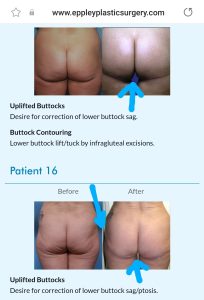 Q: Dr. Eppley, I am interested I lower buttock lifts. I am attaching some photos from your website where the butt seems lifted and not squared or boxed and flattened. I also like that you remove enough of the diaper bulge and create space between the thighs for a more youthful look. Would that be what I could expect?
Q: Dr. Eppley, I am interested I lower buttock lifts. I am attaching some photos from your website where the butt seems lifted and not squared or boxed and flattened. I also like that you remove enough of the diaper bulge and create space between the thighs for a more youthful look. Would that be what I could expect?
Thank you for taking time to give a clear description of what needs to happen. I do have some areas in the butt that are dented and as you can tell, my one butt cheek is smaller.. Would this be filled with my own fat to create a more uniform tight small round bottom?uare
A: A lower buttock lift/tuck is not a straight line excision as it inner and outer ends must curve up a bit. There are limits to these inner and outer extensions however. While carrying the excision on the inner side it must not get too close to the labia to avoid scar contraction on them. The outer end of the excision is limited by not having it go too far to the sides so that the scar line is visible.
Certainly at the same time fat injections can be done to try and improve buttock size asymmetries or any indentations.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 40 year old transgender woman and I wish to have hip implant surgery. My plastic surgeon here tells me that he has never done hip implant surgery and advises me to come to you who has experience in this field. All the more reason for the risk of complications that he wouldn’t know how to best manage.
I’ve attached pictures of my body so you can see the disparity in my hip-to-shoulder ratio. For me it is not easy to come all the way to America to have this surgery and for this reason I speak to you very clearly and exhaustively in order to make the most weighted decision possible.
I want a hip implant that has AT LEAST 6 cm of outward projection. I’m not interested in seeing the edges of the prosthesis (and therefore that it is known that it is an implant) and I’m not even interested in the vertical and horizontal size of the prosthesis. The really important thing for me is that the prosthesis has 6 cm of projection.
A: You can not have hip implants that have 6cm projection as that is a complication just waiting to happen. Your hips tissues are too thin to support anything but the thinnest of hip implants. What you are desiring can not be safely achieved.
Hip implants have a fairly high rate of complications due to the more superficial tissue location in which they have to be placed so patients have to be selected very carefully to try and lower those risks. There are two major risk factors, 1) thin patients with little subcutaneous fat (inadequate soft tissue cover) and 2) implants that are too big. (too thick for the tissues to adequately support them) Both of these hip implant considerations are judgment issues with no absolutes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, If I had forehead augmentation, then hair transplants afterward over the augmented area, would the augmentation decrease the chance of success hair transplantation? I’m thinking about decrease in blood supply. Also, if there were shock hair loss above the augmented area, would the augmentation make it less likely for that hair to grow back? And does this all depend on what augmentation material was used. Thanks so much!
A: The hair follicles are in a more superficial scalp area than the implant down at the bone level. So one can safely have a hair transplant after having a forehead implant. The implant does NOT result in less blood supply to the scalp since it is placed under all the scalp layers. This effect does not change based on the implant material.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Looking to have my lower sagging skin removed and a lift for a high placed, round, full, perky butt. Thank you.
A:You are referring to your banana roll lower buttock sag which can only be treated by a lower buttock excisional lift…of which you are a good candidate and for a problem in which there is no other effective solution. The objective of that surgery is to get rid of the lower buttock overhang of which the tradeoff is a scar line at the new infragluteal crease. I would not necessarily call a ‘highly placed round full perky butt’ an expected outcome of the surgery. Getting rid of the overhang and tucking the bottom of the buttocks in does help create a shorter and rounder appearance to the buttock but that is because it shortens the elongated appearance of the buttock due to the overhang.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve also tried dermafillers and I liked the way it looked but I think I’d prefer implants but I’m not so sure, my main concern is the paranasal and i want more of a full look in the front view io my face, i circled my main concerns.
A:The midface areas you have circled do reflect a central midface deficiency for which implant augmentation would be a better long term option than injectable fillers. When it comes to your midface augmentation with implants the only question is whether standard or custom implants would offer the better aesthetic outcome. The custom implant approach is always better with such a large surface area of bone coverage.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had bilateral testicular implants several months ago – 4.0 cm by 3.0 cm – cosmetically for atrophied testicles with testosterone replacement therapy. I stated my preference for large implant size but was not given a choice. The procedure and recovery went very well. The scrotum was pretreated with Botox for tissue relaxation and the implants are easily mobilized (I continue to do traction 3 times daily with full mobilization in the scrotal sac.)
Ideally, I would like to electively upgrade to the 7.5 cm implant length. Am I a candidate even though dual prosthetic implants were not placed at the first implant as a tissue expander?
A:You should be good for at least 6.5 or 7cms with the existing implants acting as a bit of a tissue expander.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I was wondering I have some cartilage on one of my ears that I wish to be trimmed. It’s the portion of cartilage that in middle of helical rim and sticks out past the rest of my ear. Can you perform this under local anesthetic and use dissolvable stitches? And can yuu do this from back of ear not on front where visible? Thank you.
A:The answer to your three questions is yes to each one of them. Then procedure can be done under local anesthesia, the incision would be on the back of the helical rim and small dissolvable sutures would be used.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I was diagnosed and told to seek a craniofacial surgeon in regards to facial asymmetry that’s caused a number of problem for me. I was told I have a craniofacial deformity and an under developed skull on one side. It’s apparent to see and I wonder what my options are to have this corrected and if your clinic could be of any help?
A: The role of 3D CT scanning in facial asymmetries is to determine whether what is seen on the outside has a skeletal basis from which a treatment plan can be devised to treat it. But the first determination in facial asymmetries is for the patient to provide a list of their external facial concerns and list them in their order of priority of concern. Then and only then is the scan used to see what the correlation is between the two. Not seeing any pictures of you does not allow this correlation between your external concerns and what is seen on your 3D CT scan.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a middle aged man who had cheek bone implant about surgery about 30 years ago in my early 20s . I had the implants removed about a year after the surgery as I felt they were to big. Unfortunately my face sagged when the implants were removed. I have learned to live with it as I did not know there was a remedy. As time goes by my face obviously has sagged more with age. I read that you can re suspend the tissue with a mitek suture.
A: The most effective treatment for cheek sagging after cheek implant removal is the placement of new cheek implants not cheek tissue resuspension. That is a poorly effective procedure for cheek ptosis.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a customized one piece jaw and chin implant. I have an existing chin implant which has held up very well with military activities. I am an infantryman so it’s the rough and tough exposure. I’ve gone through wrestling classes with it and it hasn’t given me any problems, I’m wondering if this full piece would have similar resilience to stress. Let’s say I get punched in the face, I’m not going to have a piece of loose jaw under my skin hopefully. Appreciate your feedback.
A: As a general rule the best way to avoid complications is to not change something (chin implant) that has never yet had a problem. While I think a custom jawline implant would hold up as well as your existing chin implant, there are no guarantees that it will.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 42 year old female who is considering doing a high smas face lift to help correct some mid face hypoplasia and cheeks that have dissented. Saw a surgeon for this and was about to book but my friend sent me your article about custom implants. I was told I have a recessed upper jaw by an oral surgeon.
I want to know which is a better choice for my situation – high smas, custom implants, or both. I’d like an option that lasts me at least 8-10 years that looks natural and youthful.
A: I am not sure how a midface can be effectively lifted when the bone support is lacking as there is nothing to hang the tissues onto or maintain its position. Midface tissues naturally descend prematurely when there is lack of bone support. The correction of midface hypoplasia is to add support which will naturally provide a lift. A lift without bone support is a wasted effort particularly in a young person.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in your forehead implant procedure, and I had sent you photos, I forgot to clarify a doubt I have, in relation to the photos I attached, is it possible to perform such a pronounced increase without modifying the temporal area? I would not like to enlarge that area because it is already large, if the projection of the implant is approximately 20 or 25 mm thick, how unnatural would it be without temporary implants? Would it be very marked?
I am sending you a picture of me, one of how I would like the result without temporary implants, and another of the idea I have of how it would look without the lateral implants. I thank you for your kind attention and information!
A: In answer to your forehead augmentation questions:
1) No one needs a 20 to 25mm forehead augmentation. That is way over estimating how much is needed to achieve a vertical forehead slope change. It is probably closer to 12mm to 15mm max.
2) With any forehead augmentation when the slope is lessened the width issue of the forehead is often overlooked. Small amounts of forehead slope change may not require the augmentation to go beyond the bony temporal lines. But in more major changes like the one you are considering that would be a must otherwise your forehead would look like a dolphin!. Thus the question is not whether a major forehead augmentation needs to cross the bony temporal line but how far it needs to extend into the temporal region to avoid an unnatural forehead shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, custom jaw implants – how does you go about making them? Is 3D imaging provided at your facility or you refer patients to a local imaging facility? If so, can imaging be provided the same day as consultation or I have to prolong my stay for a few days? What is success rate of these procedures in terms of surgery and post-surgery complications?
A: In answer to your custom facial implant questions:
1) The patient gets their 3D scan at a local facility, we provide the order for it.
2) Designing custom facial implants is a process that involves imaging goal setting using the patient pictures and online engineering with 3D Systems company.
3) Facial image goal setting can be established once patient pictures are obtained, whether that is done before a virtual or office consultation or after.
4) While custom facial implants have a high success rate, as they achieve facial changes that are not possible by any other method, it does involve an implant which has its own unique risks of potential revisional surgery. In custom facial implants my experience has been that up to 1/3 of the patients will undergo some form of revisional surgery, almost always for aesthetic reasons.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a couple of questions for that I was hoping you could answer about testicle implants:
1) You mentioned an expectation that the scrotum would initially be tight following the surgery but would “relax” or “loosen” over time. Can he provide any more detail of what I should expect in that respect? Is there anything that can be done to help along that process?
2) You mentioned a risk of wraparound implants detaching. I would be curious in knowing the actual percentage risk of detachment in cases like mine.
A: In answer to your testicle implant questions:
1) It usually takes 2 to 3 months for the scrotum to stretch and fully relax. Because the scrotum is in a gravity dependent position time is favorable for this relaxation process.
4) Up to 1/3 of wrap around implants will have the complication of detachment (separation) either in the short or long-term. Thus it is not an insignificant risk of it happening.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I’m particularly interested in if it’s possible to reduce my skull width/size to within a cis female range.
A:The answer to what is possible begs the question of what is a female skull size/shape compared to what you have now? In other words can skull reduction surgery make enough of a visible difference to achieve a head feminizing effect from your perspective? If I has a better understanding, from a visual standpoint, of what you would consider as the desired change I could then answer the question of whether it is surgically possible. My suspicion is that it would take a 360 degree circumferential approach to achieve that effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a left rib flare birth defect. My 10th rib is totally twisted outwards at its tip which hurts when rotating or bending. Audible clicking sound, but no “sleeping syndrome”. I am in GE Germany and surgeons prefer conservative methods here. I wanted to know what was your point of view on my problem and if there is another solution than acceptance.
Thanks Dr !
A: The 10th rib flare can be reduced or eliminated based on how much of the rib can be safely resected. (in which a CT scan will provide that information) I would at least get that info and then see how much improvement can be achieved by rib removal surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have deep set, low brows and small eyes. I wanted to know if there anything that could make my eyes look more open.
A:There are two procedures that would open up deep set eyes in a female, brow bone reduction and a browlift. Whether an upper blepharoplasty as well would be helpful is also consideration.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had zygomatic bone repositioning. In the CT scan I’m wondering, why I do not see bone union in my maxillary region after zygomatic bone reposition (osteomy, delayed reposition). After surgery there is bone union on zygomatic arch, on the orbital rim, but maxillary region.
How it’s possible that gap has not reduced even a bit since surgery? Overally the whole bone complex is stabilised but I’m worried about those gaps on maxillary bone
I attached some pictured from different CTs. CT performed before miniplates removement – 2 years after surgery
I got tinnitus and ETD and I wonder if such gap can be bad for my health… maybe some bacteria from sinuses may transfer to other skull regions?
But once again, how it’s possible that gap has not reduced, like there is no bone. I marked (red line) the place where is very small distance between bone ends and still no union there
Or maybe there is a bone but too thin to be visible on CT? how to check that?
A: I don’t see any mystery here…. the thin bones of the maxilla and even the zygomatic body often heal by a fibrous union not a bony union. These are thin bones that don’t carry much functional loading forces so they are not going to heal like the thicker skull or mandible. There are no medical issues associated with this type of common midfacial bone healing pattern.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, what the risks in temporal artery ligation in stopping blood flow in this artery. In other words, what is impacted by loosing blood flow (forehead/scalp skin impacts, loose of hair, risk of stroke, other)?
A: This is a common concern that, fortunately, has no anatomic basis. The arteries that feed the scalp are not endpoints but actually connect with the arteries from the opposite side in what is called an extensive anastomotic network. Thus you really can’t shut off the blood flow to the scalp almost no matter what you do. It is these anatomic anastomoses which makes it necessary in temporal artery ligation to shut off the inflow and the backflow from the visible artery locations for it to work in decreasing their visibility.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Is an 8cm Clavicle Reduction feasible? Is it possible to get 2 Rounds Of Clavicle Width Reduction?
A: I am not sure whether with an 8cm reduction you are referring to one side or both sides combined. If you mean 8cm per side that would not be possible even with 2 rounds of clavicle reduction surgery. If you are referring to 8cms combined for both sides then it could be done with 2 rounds of the surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am wondering if you could kindly advise at what age is it possible to have treatment for a brachycephalic head shape? Is it possible to treat younger patients or is it advisable to wait until adulthood?
A: Anytime after puberty would be fine for aesthetic skull reshaping procedures as the skull is fairly mature by the teenage years.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Are skull implants permanent ? Any problems after the surgery and any precautions in one’s lifetime with them?
A: Skull implants are permanent and never need to be replaced. As long as one is happy with the initial aesthetic result there is no need to do anything with the implant for the rest of one’s lifetime.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to reshape a skull that is affected from Pagets disease?
A: I assume you are referring to reducing the exostoses or overgrowths that occur on the outer surface off the skull. Such exostoses are usually softer bone that is more vascular but they can be reduced. The more pertinent question is will they reoccur and/or are they more prone to reoccur because of the underlying pathology?
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am planning to have an approximately 2000 graft FUE scalp to beard transplant, covering basically the entire classic beard area. With you, we have met and planned for several facial cosmetic surgeries some day later this year TBD. (e.g including IOM implants and sliding genio etc)
For scheduling purposes, I am wondering if there is a number of months I should wait before or after the surgeries with you to get the beard transplant.
A: I would allow for 3 months either before or after any facial surgery for doing a beard transplant.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in undergoing reversal V-line surgery and would like to know the best approach for achieving a natural-looking jawline while still being able to participate in activities such as sparring in the future. I aware that custom jawline surgery is a common option, but I am curious if custom bone grafting would be a more natural and stronger option.
A: Onlay bone grafting is never a viable option for any form of aesthetic jaw augmentation for a number of practical and biologic reasons, most notably the high and irregular absorption of the bone grafts that will occur.
Dr. Barry Eppley
World Renowned Plastic Surgeon