Your Questions
Your Questions
Q: Dr. Eppley, Hello, I live in Scotland and I want to have surgery because I am not happy with the shape of my skull. But I have a question, is the back of my skull high or the front low, what do you think is the problem exactly?
A:The interpretation of a head shape is very individualized so either approach (sagittal reduction or forehead augmentation) is an option. Looking at either potential change should help you determine of either skull reshaping approach is an improvement. (see attached imaging) There is no question in just looking at the magnitude of the ‘deformity’ the backward forehead slope/brow bone protrusion is the more significant of the two.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I found your page when searching for testicle enlargement. I’ve been on testosterone for about a year and have noted a significant decrease in the size of both of my testicles during that time.
I have heard of two possible procedures and would like to get information on both.
First is an implant that wraps around the testicle and is filled with silicone.
The second is testicle removal and replacement with an artificial testicle. I realize that this will eliminate my body’s production of T but my level was nearly at the bottom of the scale before I started T replacement therapy. Since I’m doing that already I don’t have any problems with this option.
At this point I’m leaning more toward the second option since the end result is similar and it just seems more reliable over the long term to me.
Just some background information. I’m 67 years old in good health. I have HBP and high cholesterol and take amlodipine, metoprolol tartrate, and simvastatin which control both well.
A:At age 67 there is no question that a solid testicle implant is what you would best suit your situation. The only question is whether testicle removal is really necessary with the placement of the implants. That would be driven by what size testicle implants you desire. In most acses of older men with testicla atrophy the testicles are left in place and larger implants are placed which naturally pushes the testicle out of visibility. (displacement effect) If there is not a big difference between the size of the implant and the testicles then testicle removal would be needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q:Dr. Eppley, Is itpossible to contour the body further through liposuction.
In this context, I have a question: Is it possible to define the midline of the abdomen more prominently using liposuction? Or to make the abdomen appear more contoured overall through liposuction?
Please find three reference images attached, including a recent photo of myself.
A:You are specifically referring to abdominal etching, a liposuction technique where lines are placed through linear fat removal. Since you mentioned the ‘midline of the abdomen’ this means midline vertical linear liposuction to make a vertical indentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have been at a stable weight for years and I don’t smoke. I lift weights 4 times a week. I had 5 children at 10 to 11 pounds each. I grew up not wearing sunscreen so age, pregnancy, weight loss, and sun damage caused me to have loose skin. I’ve been told I can’t have a BBL because there is not enough fat.
Would you be able to help me? Not sure if I need a lower buttock lift only or if implants are necessary. I look okay in photos- which is why I sent them- but definitely not in a bikini or naked. I was excited to find you online because you are exactly whom I was looking for- your skills fit what I’m wanting.
I look forward to hearing from you.
A:The key to understanding buttock reshaping procedures is what areas they affect. Per the diagram implants affect only the top ½ or 2/3s of the buttocks while lifts/tucks affect only the bottom third of the buttocks.
That being said when you look at your buttocks, while they are a bit flatter in projection, there is significant ptosis or sag at their lower pole and I would view that as the bigger of the two issues. Thus lower buttock lifts are more indicated for you and you do that first and then see what you thinl about implant augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Will my surgery leave a scar?
A: The question is not whether surgery will leave a scar, as every incision does, by how significant will that scar be.
There are a wide number of factors that influence the appearance of an incisional scar from how the incision was made, what was done through that incision, the technique of wound closure and the skill of the surgeon doing it, skin type and pigment and where on the body was the incision located.
Scars shold never be considered invisible, just at well levek of inconspicuous will it be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m curious about your thoughts on the correction of low set ears for individuals with disorders like Turner or Noonan syndrome. Attached is not my photo, but a photo of another woman with similar neck/facial structure as myself. I’m aware of otoplasty for things like ear pinning and other ear deformities (my ears are constricted as well as low set), but I have yet to see anything in the literature or otherwise for repositioning ears heightwise. Is such a correction possible? How would you do it, if so? Thanks for your time!
A: The surgery for improvement/correction of low set ears remains currently elusive for me. I have tried numerous techniques all of which have not been successful. The issue is that the ear is pinned in its loctation by the external auditory canal cartilage. I suspect that the canal cartilage could be transected and rotated to provide some improved positioning but even that would not provide a major superior relocation of the external ear.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Do you guys offer orthognathic surgery to correct the asymmetry of the jaw or implants? What are the costs of both with the xray that I sent?
A: The first question is what do you need and what is the best approach for your jaw asymmetry? That would require more information to make that determination. But as a general statement most jaw asymmetries are best treated by a custom jawline implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Across the old implant design, CT scan, and picture, are you able to assess whether I have masseter muscle dehiscence? Is it possible that I don’t, and that my current implants poke out without having “broken” the masseter?
If I do have jaw dehiscence, how can that affect the visual outcome of the new implants? (Must I expect repeated implant reveal?)
Does the new implant design need to take any of this into consideration?
A: The scan is not going to tell you whether you have a soft tissue problem like masseter muscle dehiscence without a special 3D scan that uses soft tissue windows. That is more of a clinical diagnosis, meaning if you bite down where does the bulge of the muscle….over the lower jaw angle or higher up? Having had a combined SSRO with immediate placement of jaw angle implants that is a primary set up for muscle dehiscence.
Implant reveal, or breaking through the muscle, is when the muscle sling is intact but the implant design. square out the angle too much, and the implant is sticking beyond the posterior of the muscle. (like your existing implant design. You have to remember the shape of the follows the shape of the bone. Since all jaw angles are rounder in shape a square jaw angle implant shape can do exactly that.
The current implant design reflects your preference for the shape of the jaw angles not mine. I would not have it so square but have tolerated a shape I am not fond of, due to the risks of muscle dehiscence or implant reveal, because it would probably not being any worse than what exists now because of the encapsulated implant pocket.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, i want to ask is any way to elongated medial canthus???im not an Asian i dont have fold i only want to elongate medial canthus.
A: You mean elongate the inner corner of the eye, not the medial canthus. This is done by a Y-V lengthening procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to get an opinion on what I think should be done my concerns are mainly relating to midfacial hypoplasia – I have a skeletal Class 3. I am thinking if Jaw Surgery would be enough with Custom Implants or if I need a higher Lefort like Lefort 2 – first – I am also concerned about upper maxilla and nose. I am also concerned about the steep mandible that I have which I believe should be slightly corrected in the jaw surgery ( CCW). What do you believe overall is the best approach to my case?
A: I would agree with the concept that any jaw surgery is done first (if indicated) and any bony deficiencies above the LeFort 1 level are dealt with secondarily by custom implant designs. Never try improve bony deficiencies above the maxilla by any type of osteotomy designs. Those LeFort osteotomy designs are made for major skeletal deficiencies, usually of a syndromic origin, not more modest aesthetic deficiencies.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How much does the occipital surgery cost and when can I return to work?
A: You did not specify what type of occipital surgery….occipital reduction or occipital augmentation….nor what type of work you do. But in either case as a general statement I would say one week.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a bridge augmentation only rhinoplasty. it seems like a simple procedure to me but i’ve never seen a surgeon heighten a radix as much as i’d want but that may be more because of patient wishes rather than their inability to do it. i added surgery goal notes as well. one other thing i wanted to add is i want a tapered bridge in a ‘ ) ( ‘ shape (refer to image 2) rather than just a straight rib graft ‘ | | ‘ in image 2 the second photo is an image of my persian friend. people say her nose is way too big but that’s exactly what id want from my rhinoplasty! i feel like we have somewhat similar nose shapes. looking forward to your response 🙂
A: When you put together all of the features of this very specific nose shape (which is not easy to achieve) you are talking an implant approach, specifically a custom nasal implant. (performed 3D designed siliconje or hand carved ePTFE) While rib grafts are the most common techniques for bridge augmentation the one thing they can’t do is make the bridge wider. (it may even make it thinner) Also no standard nasal implant will achieve it either as they also will not make it wider all the way down to the tip.
I have not seen a side view picture to see what how much height is needed at the radix which is the highest and widest part of his type of bridge augmentation. My preliminary estimate is that it would be at least 7mms.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to schedule a consultation in regards to my nasolabial folds, specifically if I would be a good candidate for excision. I am 30 years old. Thank you.
A: I would never consider nasolabial fold excision at your young age, the scar would never be worth it. You have to consider why they are there…significant facial lipoatrophy. (no subcutaneous fat) You consider augmentation and I don’t mean fat injections which will never work in your face.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is the only way to achieve jaw augmentation an incision outer of the mouth area? What about 3 pieces implant? The incision will be visible?
A: Custom jawline implants are placed as one solid piece, which is what you want for their linear effect, through three small incisions. Two inside the mouth back on the cheeks opposite tyhe 2nd/3rd molars and one small one under the chin.
While the intraoral incisions can be replaced by external ones behind the jaw angles that would leave external scars…which for some men may be acceptable but not for females.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had Medpor jaw angle implants of the lateral style with 9mm width placed 7 months ago, as well as a 7mm forward and 4mm down genioplasty. The left side was placed a little too low, though, and I felt that the genioplasty advancement was too big, so I went to another surgeon to attempt to reposition it and reduce the genioplasty. The genioplasty was reduced successfully, but somehow my left jaw angle was repositioned even lower! You can imagine my horror when I roughly measured that one side was about 1 cm lower than the other!
I am already scheduled to have my jaw implants removed, and it will be 72 days between the revision surgery and the implant removal. I am not so much worried about the right jaw implant, since it only provided lateral augmentation, but I am very worried about sagging from the larger jaw implant. My surgeon said that it will likely sag, but it will be minimal. I have thick skin, and I never had a particularly defined jawline to begin with. What should I expect in terms of soft tissue response. Are there any soft tissue management strategies you would recommend, such as liposuction or fat grafting?
Thank you very much
A: You take out the jaw angle implants first and then see what happens. No one knows how the soft tissue will respond and what, if any, soft tissue problem may ensue. Trust the healing process and don’t get ahead of yourself. Quite frankly these questions are more appropriately directed to the surgeon who is doing the procedure who has full knowledge of your case.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I have a webbed neck and would like to learn more about the surgical procedure. I have not been diagnosed with Turner’s Syndrome, however I was also never tested. I am very self-conscious about it and would love to improve the look and functionality of my neck. I look forward to speaking with you soon.
A: Webbed neck surgery is done to improve the appearance of the webs. It does not, however, improve the function of the neck. (e.g., range of motion) To demonstrate what degree of improvement in the neck webs that could be obtyained I need a straight on picture that shows the webs on both sides of the neck in the front view. The current picture does not do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My head big size 61 sm. Can it be reduced?
A: The question is not whether it can be reduced but whether it can be done enough to justify your efforts and goal. In reality skull reduction is best suited for spot area reductions rather than a major overall head size reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 42yo Male to Female Transgender Person. Im intrested in your Scrotoplasty. Do you also offer Orchiectomy Surgery ? As atm im using Androcur as a Testosteron Blocker.
A:Testicle removal can be done with scrotoplasty although if the eventual goal is to have SRS (sexual reassignment surgery) then this procedure would be unnecessary. The transfemale that may be considering such a scrotoplasty usually is not progressing onward to SRS.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to get the rib removal done, I’m wondering if I’m a good candidate and if I’d be one of those patients that would have a dramatic difference or subtle difference. I’ve looked into getting a BBL but I’m hoping maybe a rib removal will slim my waist enough where I wouldn’t care to enlarge my hips. My waist currently is about 25in and my hips are about 33/34. I would like my waist to go down closer to a 21/22 so wondering if that’s possible with my anatomy.
A:Thank you for your inquiry and sending your pictures. Your question is a good one in that with your body type (tall and thin but with a vertically long buttocks) you could go either direction of a BBL or rib removal. I don’t think either one is a bad choice. Whether rib removal results are subtle or dramatic is open to personal interpretation. But what I can say is the following: 1) Dio I think your waistline results will drop from 25″ to 21″… no (tall and thin patients do get the best results but that would be expected too much in my experience) and 2) an expected change in your waistline shape I have shown in the attached image prediction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I had a couple questions about my eye area:
1. The first two pictures show my current eye area completely relaxed. Do I have ptosis of the upper or lower eyelid? If not, would ptosis surgery or any other procedure work to lift my lower or upper eyelids a bit?
2. One of my desired outcomes is moving the inner corners of my eyes a couple millimeters inward, as shown in picture 3 as a slight morph of the second picture. I notice I get this result when I pull very slightly with my fingers inward, and the eyelids still remain attached to the eyeball. This makes me think I have loose skin or medial canthal tendons. I have seen mixed opinions online, and you stated in a post that this would be difficult to achieve without risking scarring. Suppose we didn’t really care about scarring. I have seen procedures designed to achieve this effect, such as C-U plasty (picture 4), which cuts the medial canthal tendon and moves one end inward, as shown in picture 6, and W-V plasty, which simply removes some skin to tighten the area. These generally are designed to correct telecanthus. Would one of these procedures, or any other ones that tighten skin or the tendons, realistically work for my case?
A :In answer to your eye reshaping questions:
1)Do you have true ptosis….not really. Maybe a 1mm. But one does not have to have true ptosis to have ptosis (upper lid elevation) surgery.
2) Lengthening the inner eye corner towards the nose is not done by any medial canthal tendon surgery or any of the procedural diagrams which you shown. (those are for webbing/hypertelorism surgeries) It is done by a tissue rearrangement technique known as a Y-V lengthening surgery. This has more favorable scar formation than its cousin, V-Y narrowing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I recently had bilateral mandibular angle implants done, and it’s been around 2 months today. However one side of my face is still extremely swollen and after reading your online forms where you state that in 3 months you should be able to see your final results. I’m getting close to that 3 month mark and one side of my face is still swollen and the other side is a little around and not sharp at all. Is there any hope of my angle implants Turing out the way I wanted them to be, nice and sharp.
A:The simple answer is no. What you are seeing at this point is about 85 to 90% of what it is going to be. So what you are looking at is the result of the style and size of the jaw angle implants, their positioning on the bone and the thickness of your overlying soift tissues. There are numerous factors that control what the final result will be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
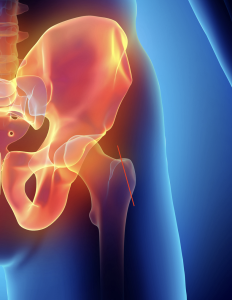 Q: Dr. Eppley, I am interested in hip reduction as per the attached diagram.
Q: Dr. Eppley, I am interested in hip reduction as per the attached diagram.
A:The diagram shows an incorrect approach to hip reduction. Hip reduction refers to the iliac crest which is the widest bony part of the hip/pelvis…which is possible. The diagram shows reduction of the greater trochanter of the femur…which is not possible due to the musculofascial attachments to it and that it is a leg bone not a hip bone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi would like to reduce the back of my head. Is it possible?
A: Yes it is. Such an occipital protrusion is almost always the result of having thicker bone. How much it can be reduced requires an x-ray to determine. Normally I would take your side view picture and show you how much reduction I think is possible but with you hairstyle I can not do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m looking to get surgery to help my eye area and have more almond shaped eyes, as well as get a more defined jawline, as well as any other surgeries you would recommend to elevate my appearance. I’m just looking for what procedures you would recommend.
A:It may be the way the picture was taken but it appears you have upper eyelid ptosis with the right eye having more ptosis than the left. Almond shaped eyes are created by elevating the outer corners and the lateral 2/3s of the lower lid by lateral canthoplasties combined with lower lid spacer grafts. In some cases an infraorbital implant may be beneficial.
The optimal method for improved jaw definition is a custom jawline implant.
Using just the front view pictures you submitted I did some initial imaging but I would need a side and oblique view pictures to ultimately define your jaw augmentation goals
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to seek your expert advice regarding a challenging situation I’ve been facing with my blepharoplasty results. I initially underwent the procedure with an American surgeon, who informed me that scarring was inevitable. However, I was not prepared for the outcome of developing atrophic scars.
To address these concerns, I opted for a revision blepharoplasty with an oculoplastic surgeon in the UK. Unfortunately, the results were not as I hoped. While one scar has widened and atrophied worse than before, the second scar was traumatized when it reopened, leaving it very wide and aesthetically displeasing. Despite undergoing laser treatments for the past year, I have not seen any noticeable improvement.
This situation has left me feeling extremely self-conscious, and I am unsure of the best way forward. I would greatly appreciate your professional opinion on potential solutions for these scars, as well as any recommendations you might have for improving their appearance.
Thank you in advance for your time and expertise. I look forward to hearing from you.
A:The success of almost any scar revision depends on how much loose tissue is present and the laxity of the surrounding tissues. When wide scarring develops after an excisional procedure (now loee of skin) in a limited space area (e.g., the eyelid) the success of a scar revision is going to be limited and could even make the scars worse. You have unfortunately proven that concept by the revisional surgery you had. While unpleasant and unsatisfying the surgical motto of… past behavior is a good predictor of future performance...should be well heeded. Or to phrase it another way as another surgical motto….if it was an easy problem to fix it would be so by now. While I think the revisional surgery was worthy of trying, its outcome tells you that for now anither revision is not going to work. In time with the benefit of aging and the creation of more and relaxed tissues another scar revision could actually be successful.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I get a skull implant where bone grows into it and replaces the implant material?
A:There is no skull or face implant material in which bone will grow into or over that becomes integrated into one’s tissue. It is a great augmentation goal but for now that remains an elusive biologic outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, If i was looking at a chin implant , jawline implant and mid face implant does that require multiple visits? Thank you
A:I assume the question is whether these implant surgeries can be done together or do they have to be done separately. (jawline and midface implants) That is a personal choice., It can be done either way. If you are certain both are needed then most people would do them all together in the same surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am i 38 yo male with asymmetry on the right side, my left side mandible is fine but the right side angles away and i’d like to have it corrected. I’d need an implant only on the one side. Let me know what is possible. thx
A:Such jaw asymmetries are treated by a custom implant designed from a 3D Ct scan of your face. So the treatment of such facial asymmetries can be improved without just trying to ‘eyeball’ the problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I’m MtF and I’m interested in more information on iliac implants. Thanks!
A:The first place to start is to determine of you are a good candidate for this unique type of hip augmentation. (iliac crest implants) To do I would need at least a front view of your hips to do some imaging of potential changes so you can see what it may look like.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,I am a male looking to improve my facial definition, so as to shape it into a more stereotypically-masculine face. I have already performed buccal fat removal and a chin implant, which I am happy with, but would like to further improve my facial definition.
A:With a lean face and prior procedures you have a good foundation for further facial masculinization results. You are a good illustration that a ‘little bit in the right places’ (the five corners of cheeks, chin and jaw angles) can create a good composite effect. I have attached some initial imaging to begin the thought process as to what to change and by how much.
Dr. Barry Eppley
World-Renowned Plastic Surgeon