Your Questions
Your Questions
Q: Dr. Eppley, Hi there I am interested in getting more information on your back lift surgery and, potentially, your waist line narrowing procedure and a rhinoplasty revision. I have horizontal stretch marks on my back that I would be looking to cover up with the vertical scar as I understand skin must be excised with the procedure. Is the vertical line typical in your back lift surgeries? Further, with the waist line narrowing procedure, I would like to discuss the risks associated with this procedure. Finally, my plan is to have a rhinoplasty revision which I understand sometimes involves using ribs depending on the procedure. I’d like to have the information to form a plan appropriately while weighing the risks associated with all procedures. I have already had a few cosmetic procedures. I look forward to speaking with you soon.
A:The vertical backlift is an excisional concept for lower torso/waist narrowing when excess back skin in particular exists. The indications for the procedure is if such excessive skin is from weight loss or liposuction….although some may just have it naturally. It differs from the more common horizontal or bra line lift which removes skin horizontally across the back which has a very different torso tightening effect. Through either type of backlift rib removal can be performed.
The key question in your case is what is your primary objective? While horizontal skin stretch marks may get removed in the process that would be an incidental effect and that alone would not serve as the reason to do the surgery given the scar tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in the one port endoscopic removal of a forehead lipoma. May I know how long the cut will be to remove it?
A: It is 2.5cms long for endoscopic forehead lipoma removal.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I happened to be at the dentist today and captured a panorex image of my chin. The center and to the left of center is where I feel a firm lump. I wonder if the more hyper dense area could represent that. I know it’s not a diagnostic image, but the general margin seems interesting. It’s interesting that the bottom of my chin looks bumpy because it feels bumpy. I wonder if this is where the residual chin implant material is.
A:A panorex x ray is a bit of a distorted image (like a globe that has been spread out to be a map) but the gross irregularities that appear are real given the prior surgery as all implants cause benign bony changes. A 3D CT scan would be the most informative but since we are going open it up anyway that will be the definitive assessment of what is there. (removal any residual implant material and smooth out the bone)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a custom skull implant. I have a few quick questions about it:
1. Do you provide any kind of guarantee or certificate after the surgery, regarding the quality and long-term durability of the implant?
2. Is it possible to stay and recover at your clinic for about 4 to 6 days post-surgery before returning to home?
3. Would it be fine if I decide to come alone? I don’t really have anyone I can trust with me in such a delicate situation, so I’d be traveling and recovering by myself.
A: In answer to your skull implant questions:
1) This is a solid silicone material, not like a gel-filled breast implant, so there is no question about its long term structural sbtability.
2) Patients usually stay overnite in the surgery center the first night after the surgery. They then stay at a local hotel for however many days they need before they go home.
3) Patients most commonly come alone so that would be our normal experience.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my goal is to drop down the brows to reduce upper eyelid exposure and make the brow shape more like a straight line rather than an arch at the corner, is that possible ? Also the incision could be made from the top of the skull at the hairline with small incision not the whole front line skull incision?
A: Brow bone implants can help lower the brows somewhat but not usually a major amount. The same applies to changing the natural shape of the eyebrows. You do brow bone implants for the primary reason of brow bone augmentation. Any other potential benefits (brow lowering and straightening) are a bonus if they occur.
Brow bones implants are placed using an endoscopic technique and the implant is introduced through a small incision behind the hairline. It is always necessary to secure the brow bone implant into place and this is most common done through small upper eyelld incisions to check the tails of the implant position as well as place a 1.5mm small screw on each side for fixation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, Doctor Eppley. How long after reversing my sliding genioplasty can I get a chin implant?
A: I would wait at least three or four months to let the chin bone heal.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
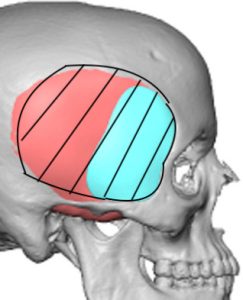
Q: Dr. Eppley, I just want my head shape to appear normal.
A: In looking at your head asymmetry it is a bilateral diametric problem, meaing the right side of your head is smaller while the left side is bigger. Thus to treat it successfully the conceptual approach is that the right side needs to be augmented while the left side needs to be reduced. (see attached picture with the purple be the augmentation while the red is the reduction) The specifics of those changes await to be determined by a 3D CT scan assessment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to ask a few questions about skull implants:
• What material would be used for the implant?
• How durable is it long-term?
• What is the price of the surgery?
• And how long would the recovery take? I need to plan my return home accordingly.
A: In answer to your skull augmentation questions:
1) Custom skull implants are made of solid silicone.
2) This is a material that is non-biodegradable and will last long past a patient’s lifetime.
3) Skull implant recovery is largely about swelling of the head and sometimes the face which takes 10 to 14 days to largely resolve. One does not wait until the swelling has resolved to go home. Most patients head home in 2 to 3 days after the surgery a female with hair can camouflage much of the swelling. There are also no sutures ro remove as they are all dissolvable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello.I have read your case study about Tragus Cartilage Reshaping after Facelift (https://exploreplasticsurgery.com/case-study-tragus-cartilage-reshaping-after-facelift/) I had the same experience after my mini Facelift and now after 1 year my tragus is still deformed and it seems permanently changed. I was wondering if there is someone you can reccomend here in Europa that can form my tragus back to my original form surgicaly? I have uploaded before and after picture of my tragus.
A: While I am certain you could have it done in Europe I would not be able to tell you whom could do it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am investigating the possibility of having an occipital skull reduction. I’m aware that an MRI is required to investigate this possibility further, and private scan clinics in Canada still require a Dr.’s referral to complete this scan. I will also have to travel to a different province to have a scan completed. I am wondering if your clinic will be able to provide a referral in advance of me requesting a consultation, or if a consultation is required first.
A: We can only provide referral letters to established patients…and it is a CT scan not an MRI.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, the problem with my head shape is that it is small from all sides and is inclined inwards from all sides(front ,back and sides)
so the pics you have attached are an augmentation from all sides i guess .
but i would at least want an augmentation from forehead and two sides to have a wider head and flatter forehead.
I am attaching your first proposal you suggested me and needed to know the following
1. my question is if we have to go for three sides augmentation do we still require two stage surgery.. I mean do we need tissue expander surgery in that case..
2. are these augmentation for life time .
3′ please also guide the procedure on how we can move step by step to move further.
A: 1( As long as the implant volume does not exceed 150ccs, regardless of its surface area coverage, a first stage expansion will not be needed.
2) Such skull implants are solid silicone so they are structural stable for a lifetiime.
3) The key to the whole process is a getting a 3D CT scan which serves as the platform on which the implant is design.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I previously had chin reduction surgery, which left my chin too short and pointy, especially when I smile. To improve it temporarily, I had fat grafting and filler placed in my chin area about 2 years ago. While that helped a bit, my chin still looks short and feels unnatural, and I would like to restore its original shape through reverse genioplasty or a custom chin implant, depending on what you think is best.
A: To restore the shape of the chin after a reduction performed by a t-shaped bony genioplasty there are two options:
1) Recut the chin bone to shorten it and widen (it was narrowed by a central wedge if bone removal and extend down a bit longer) it which will need at least some cadaveric bone graft to do so.
or
2) custom chin implant
If you look at the dimensional changes needed (wider and shorter) it would seem that doing #1 is more appropriate since an implant can not make the chin shorter only wider.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, hello there. Please can you tell me how much experience the surgeon has in the following surgeries and approximate prices? Pelvic Plasty Clavicle Shortening Lower rib removal Thank you
A: I performed the 1st rib removal surgery in the US ten years ago and have done hundreds of cases since.
I am only one of three surgeons in the world that perform clavicle shortening osteotomies and have over 150 shoulder reduction surgeries.
I am the only surgeon in the US that is authorized to perform the Pelvic Plasty procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My 23 month son has untreated moderate plagiocephaly. I saw you had done an implant for a child in the photos. I am wondering the process, age and if the procedure needs to be redone as a young adult?
A: Skull implants for plagiocephaly are only done on patients 16 years and older.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there! I was wondering how many vertical backlift surgeries you have done since this one posted on your website in 2022? Also wondering where you are based? I am interested. Thanks
A:Over the past 3 years I have done eleven of them, four with rib removals and seven without. The key qualifier is how much loose back or torso skin one has as demonstrated by the pinch test.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I got chin lipo done with you guys a few years ago. I would like to sharpen my jawline even more and am interested in submentoplasty surgery. How much is the submentoplasty surgery?
A:The intent of a submentoplasty is really to help the neck (cerviciomental) angle. I don’t see it as a method to make the jawline more pronounced. It is very difficult, if nit impossible, for most patients to reduce their way into a better jawline.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I wanted to enquire regarding some facial cosmetic surgeries. I was interested in buccal fat removal, cheek and chin liposuction, and possibly jaw + chin implants.
A:I can certainly see what you are trying to accomplish….take a rounder facial shape and change it into a more defined one. A good guideline to remember in facial reshaping is that one can not reduce their way into a better facial shape, augmentation is the primary method. Meaning the fat removal procedures you have mentioned, which are all needed, are ancillary to improving your facial shape. Facial augmentation, such as that of your jawline, is the primary driver of change.(see attached imaging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a dent on the left side of my head, as a result of a head operation a year ago and the skull has been installed, but I have a small dent on the left side because my head muscles have shrunk, can the dent be repaired?
 A:This is a classic indentation from temporal muscle atrophy after a craniotomy. The muscle volume has been lost as the muscle has shrunken down after being elevated to do the bone flap. And even though the muscle was resuspended the muscle shrinks because its point of bony origin has been disrupted. Because the muscle has shrunk its size/volume can not be augmented. It now requires an implant to be paced on top of the muscle under the scalp to fix the temporal concavity. There are numerous implant material to do so. The implant footprint would probably look similar to the attached diagram with 5 to 6mms thickness.
A:This is a classic indentation from temporal muscle atrophy after a craniotomy. The muscle volume has been lost as the muscle has shrunken down after being elevated to do the bone flap. And even though the muscle was resuspended the muscle shrinks because its point of bony origin has been disrupted. Because the muscle has shrunk its size/volume can not be augmented. It now requires an implant to be paced on top of the muscle under the scalp to fix the temporal concavity. There are numerous implant material to do so. The implant footprint would probably look similar to the attached diagram with 5 to 6mms thickness.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My current chin implant is a size medium, and does have wings. My main concern when I got it was to not look jowly, and for a more even look.. it is rounded- unisex, which I’m not sure why he picked medium or unisex?? I included pictures in the inquiry, but here are more.
A:He picked it because he was not thinking of any of those issues. Some surgeons tend to use one implant style for all patients. You are assuming most surgeons are artists….that is a generous assumption. Most are technicians robotically doing the same style implant for everyone. Hopefully what the patient needs is what the surgeon likes or knows how to do.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi! I was wondering if you do surgery to enlarge your tongue?
A:I do not. I am not even sure how it would be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I get a rhinoplasty at the same time as my cheek and jaw implant surgery? Or is it too much surgery at one time?
A: It is not rare for a patient to have rhinoplasty with their cheek and jaw implant augmentations. The question is not whether it can be done but whether the patient wants to do it.It is done for the obvouis reason…convenience and efficiency.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to know Dr Eppley’s thoughts on whether or not I can get fillers first to see what projection increase is more desirable for me. Since this is going to be a revision chin surgery I want it to be done once and I don’t have to second guess what I want. Can you let me know if this is something that doesn’t interfere in his way of the revision. Having considered that I will get the fillers that last the least amount of time. So we don’t have to postpone the surgery too far in the future from now
A: There is certainly no harm to ‘test’ chin augmentation using injectable fillers. While it is not necessarily a 1:1 correlation between the effect of fillers in the chin soft tissues and the effect of an implant on the chin bone there is no adverse effect by doing so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello doctor I wanted to ask you how much does the procedure for correcting a flat head cost and what is required for this how long does the operation and recovery take?
A: You are referring to a back of the head custom skull implant. This implant is made from a 3D skull CT scan that the patient obtains where they live.
The operation for skull implant placement is 90 minutes done under general anesthesia. Recovery is largely about swelling which takes 10 to 14 days to significantly resolve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello! hen I was born my mother said that my head was not fully formed and that she used to put pillows around my head. I didn’t put much attention to it then since I was a boy and didn’t pay attention to my looks. When I see my head today from different angels it looks different (according to me) on the each side. I wonder what the cause to that could be since my head a couple years ago looked normal from all sides. I will drop some pictures below. A pic for left and a pic for right side, and finally a pic of me when I was younger. Is it all in my head or is there actually a change in my head and if so what is the cause/what can be done to fix it?
A: It is difficult in pictures to say what differences exist in head shape between the two sides and I certainly can not say what exists today is different from years ago. The definitive answer about any head shape concerns can be definitely answered by a 3D CT skull scan which will remove all speculation about what its shape is.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, Dr. Eppley. I had a sliding genioplasty of 5mm forward 8 weeks ago. My face was already long, which I remarked to the surgeon many times, Now my face looks so much longer and I honestly hate the result and wasn’t what I expected at all. A) Is the length of my face going to decrease significantly from here? B) If I decide to move forward with a reversal, is there always laxity, fullness and damage to the soft tissue (I’m only 24 years old)? C) One of my problems is that my lip became thin, is a reversal going to make the lip worse or spoil any chances of the lip getting back to its normal size? Thank you so much, Doctor.
A: In answer to your postop sliding geniopalsty questions:
- At 8 weeks after surgery what you are now seeing is 90% plus what the final result will be.
- There is a risk of soft tissue laxity if the sliding genioplasty is fully reversed. Subtotal reversal will lessen that risk.
- Sliding genioplasty reversal is unlikely to make the lip any thinner….but it will also not make it any thicker.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q:Dr. Eppley My testicles have shrunk as I was put on testosterone in my 20’s but into has caused major shrinkage. Im now 65. They are like raisins.. Can you leave them intact and install 2 prosthetic implants below the original instead? Average cost? Id prefer not to use free floating medical grade silicone injections. Thank you
A: With very small testicles the side by side testicle implant displacement technique works vey well with a low complication rate (infection) The key question is what size the testickle implants should be. For an adequate displacement effect I wood recommend at least 5.5 to 6.0cm implant sizes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I had a sliding genioplasty and a revision done with a bigger plate at your office along with a chin implant. I am currently admitted to a hospital waiting to get clearance for an MRI but they will not proceed unless I provide them with a response from your office about the material of the plates and screws and brochure of the brand of plates and screws since MRI can seriously displace some metals.
A: All metal fixation hardware used in the face and skull today is made of titanium, a. non-ferromagnetic metal. It has been that way since MRIs became clinically used to avoid the risk of any risk of magnetic attraction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, is it possible to get a little bit of the brow bone shaven off with an endoscopic procedure with a small incision in the hairline? I see pictures of then entire scalp being lifted, or they go in via the eyelid, those look too extreme.
A: Brow bone shaving can be done through a limited scalp or hairline but not endoscopically as power instruments can not pass through an endoscopic approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 30 year old male with a 23.5″ head that looks huge for my 5’8″ body. I’m interested in reducing the frontal bossing, lowering the hairline, and having a hair transplant if it’s feasible.
A: Head circumference aside I think the primary problem is the frontal bossing which is magnified by the high hairline. This is a challenging problem in that both issues must be dealt with for an effective improvement. Unfortinately a ‘scarless’; hair transplant alone to move the frontal hairline forward will likely be be inadequate as the density of hair that can be placed and how far forward it can advanced will simply not be enough….and that leaves frontal bossing unchanged.
Normally I would be very cautious about a frontal hairline advancement in a male with a high hairline because of the obvious scar line and you never know just how much forward movement the scalp will permit. Also the greatest movement needed of the hairline is where it is most recessed (temporal hairline) so a frontal hairline advancement does not solve the hairline shape…it moves it all forward along the similar pattern that it has. But if one needs frontal bossing reduction there is no other good incisional choice to do it so that may tip the balance in favor of it for its dual benefit.
That being said my advice is:
1) I would certainly also consult with a hair transplant specialist to get their thoughts about the frontal hairline since this is not my area of expertise.
2) It is prudent to assess the frontal bossing with a 2D CT scan to measure the bone thickness to determine if adequate bony reduction can be safely done.
3) I have attached an image of what I think can be realistically achieved by a combined frontal hairline and frontal bossing reduction. (if the bone permits) The purpose of the image is not to show you exactly what the result would be. Rather it is done for the purposes of howing what I would expect the least result to be….as that should be the trigger for surgery. (not what one may ideally want as who knows if that is ever achievable)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if a hemi-coronal approach for anterior temporalis reduction leaves noticeable scarring and can be combined for a brow lift without altering hairline. (I was considering this anyway).
 A:There is no question that a hemi-coronal incision provides adequate access for an anterior temporal muscle reduction. I have attached a patient who had this approach a year ago who did use that same incision for a browlift secondarily. Now he did not care about the hairline or the scar since he wears a hair piece. And you would need that incision at the frontal hairline for the browlift so the frontal hairline does not move. But the purpose of the picture is to show a similar scar on a shaved head.
A:There is no question that a hemi-coronal incision provides adequate access for an anterior temporal muscle reduction. I have attached a patient who had this approach a year ago who did use that same incision for a browlift secondarily. Now he did not care about the hairline or the scar since he wears a hair piece. And you would need that incision at the frontal hairline for the browlift so the frontal hairline does not move. But the purpose of the picture is to show a similar scar on a shaved head.
Dr. Barry Eppley
World-Renowned Plastic Surgeon