Your Questions
Your Questions
Q: Dr. Eppley, The main issue is I feel it’s abnormally large head which disproportionate to the rest of my body, in addition to my face being too round and full which I believe significantly distorts my features. I’m 37 years old… 6’1, 275lbs, but even before I gained this weight, I was an avid weight lifter and I incorporated cardio into my workouts. For years I maintained a weight between 235lb-245lbs; however, the weight in my face never seemed to significantly fluctuate as I would have liked. So now I feel surgery is my only option. Essentially, I want a slimmer, more sculpted face. I don’t know if my goals are realistic, and exactly what procedures I would need, but I’m sending pics of myself and the look I’m hoping to achieve.
A:Thank you for your inquiry and sending your pictures. I think we have to acknowledge that you achieving hey look that is similar to the ideal pictures is not achievable as they have completely different faces, body type and wait. But there is nothing wrong with having goals. The real question is what can be done with the anatomy that you have. When it comes to your head shape the most practical improvement would come from narrating the sides of your head so they are less convex and more of a straight profile. When I say practical I am specifically referring to the lack of any visible scars to achieve that change. In the shaved head male one must be very cautious about scars and their length and location as scars are an aesthetic trade-off that must be balanced against what is the statically again. At least the temporal reduction procedure for head narrowing is essentially scarless.
From a face standpoint it appears in all of your pictures that you hold your jaw down and forward in what is a common jaw thrust maneuver as patients feel that that makes them look better. Besides creating a more defined jawline it also helps lengthen the face or deround it. This deliberate jaw positioning is really a test of the effects of facial lengthening.. Thus it appears that a custom jawline implant to make that type of permanent change without having to create it as well as some cheek defatting would be the most successful procedures to slim or deround your face.
To evaluate these concepts in more detail I need facial pictures from three different angles, front side and three-quarter view in a non-jaw thrust position, to do predictive imaging the effects of the procedures that I feel would most benefit you.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For many years I could only wear a hat because of these deformity. Do you think there is a way to fix it without making it look feminine?
A: Thank you for your inquiry and sending your pictures. I believe what you are referring to is the large brow bone protrusion that you have. When it comes to brow bone reduction, while itis most commonly associated today with forehead head feminization in the transgender patient, in my experience about 50% of the brow bone reductions I have ever done are in men. There are different brow bone reduction variations in male brow bone reduction versus transgender brow bone reduction. In the transgender patient the goal is to make it completely flat which is more consistent with that of the female forehead. In the male the goal is not to make it completely flat but to reduce it enough so that it no longer looks Neanderthal-like or overly protrusive. In essence in the transgender patient the goal is to create a different gender appearance. Conversely in the mail it is about reducing an abnormal protrusion of the brow bone and to make it look more normal in projection.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q; Dr. Eppley, For ,my custom jawline implant design ,my questions are:
Questions
- What is my skull’s current bigonial width-to-bizygomatic width ratio, and what do you think will be the ideal ratio for me? What percentage does the current implant design change this ratio to? I’m hoping for the ratio to land somewhere in the 90-95% range, but I’ll defer to you on what will look the best. I think the back corners of my jaw are close to an ideal width in their current state and only need a minor augmentation, but I’d be interested to know your opinion on this. While we don’t want to add so much width that it looks weird or unnatural, we do want to add enough width to make a noticeable positive impact, *especially* in the areas nearest to the chin.
- What is my skull’s current Frankfort mandibular plane angle, and what do you think will be the ideal ratio for me? What angle does the current implant design change this angle to? I’m hoping for something in the 22-25° range, but again, I’ll defer to you. I think my current jaw angle is far too high, and the current implant design appears to me like it might not lengthen the ramus enough to adequately lower this angle, but again, I’ll defer to you on what is ideal for me.
Goals:
We want the implant to “unround” my face and optimize the masculine balance of the lower face, rather than purely maximizing the size of it—all the changes should look very masculine, but also very natural, balanced and proportionate—while we don’t want to undercorrect and not add enough, we also want to avoid overcorrecting and adding *excessive* bulk. The implant should achieve 4 main things:
1)Significant vertical lengthening of my jaw: we want to lower the ramus and mandibular body to create a more masculine angle and shape. I’ll leave it up to you exactly how much to add vertically, but the result should look very masculine, yet natural.
2)Obviously by adding significant vertical length, we’ll also be adding substantial width, because of the outward sloping angle. We definitely want the implant to add an impactful amount of width, especially in the areas nearest to the chin—but let’s also be careful not to add *too much* width, because I don’t want it to look excessively bulky or boxy. Again, we want the width to look very masculine but natural.
3)Significantly widen the chin in the front, creating a strong, square chin with defined angles. The widening of the chin needs to be significant enough to stretch the skin and get rid of the puffy “carp-like” look in my lips and cheeks.
4)Horizontally lengthen the chin 4-6 mm, for the same reason—to eliminate the carp lip. If the implant adds a few mm of vertical chin length as a mere byproduct of the wraparound, I wouldn’t be opposed to that either.
A: For the purposes of custom implant design clarifications;
1) Implant designing is not like orthognathic surgery which extensively uses cephalometric landmarks. Thus we do not use any of these measurements, ratios or numbers to make a custom implant as the end goal is to make an external soft tissue change. This is not a measurable process and until someone establishes what the impact is of augmenting bone to its soft tissue effects this will continue to be more of an art than a mathematical science.
2) Implant designing must factor in a major consideration of which a patient would not be aware…. the ability to accurately and safely place it. This consideration has major influences on the design and is one that I would only be aware.
3) The first implant design is a good approximation of what the final implant design would be since I made it based on the general goals of what can be accomplished. From a chin standpoint there can be no changes to this first design given the soft tissue restrictions imposed by the prior vertical lengthening bony genioplasty. I am not even sure if those implant dimensions will even fit but I am willing to leave it that way as should some implant reduction be necessary it can always be done in surgery. I would rather keep that amount of chin implant volume in the hope that I don’t have to modify it.
4) There is some room for additional implant volume back in the jaw angles as indicated in the attached diagram. However this is the maximum amount but I am willing to do.
5) I can certainly appreciate all of your well described goals but they defy any specific measured way to achieve them. And even if we knew exactly what those measurements would be they would have to be modified if they exceeded my design specifications to be able to be surgically placed anyway. Thus we are really creating an implant design that is driven more by soft tissue limitations as well as what can be placed as a one-piece implant.
6) That being said the overall implant design is certainly going to get you closer to your stated jaw augmentation goals but how close they will do so remains an unpredictable outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in skull reshaping surgery for my 12 month daughter.
A:In the skull reshaping procedures that I perform these are for adults not infants and children.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Does the mouth widening surgery also give a wider smile and Is it possible for me to see some after pictures with the scar healed.
 A:By definition if you make the mouth wider at rest it will also get wider when one smiles.
A:By definition if you make the mouth wider at rest it will also get wider when one smiles.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m 22 years old and I’m looking for help with facial asymmetry. I have one eye slightly higher than the other, uneven cheeks and smile lines, and a mouth that shifts when I talk.
I’ve been told this is natural and can’t be fixed, but I believe it affects my confidence and quality of life. I’m interested in understanding whether facial balancing surgery or structural correction could help in my case.
I have had facial asymmetry since childhood. I feel that one side of my face appears straight, while the other side looks slightly curved — similar to how hands look when raised in prayer, with one side more inward or rounded.
This difference becomes more visible when I talk or smile, as my face shifts more to one side. I believe the issue may be due to bone structure or muscle imbalance.
Could you please tell me if this kind of facial asymmetry (possibly involving zygomatic bone or jaw alignment) can be corrected through surgery or other treatments?
A: While you have numerous facial asymmetries, as you have mentioned, most of them do not justify surgical intervention as they can not be completely corrected. I don’t think surgery is worth the effort. The exception is your twisted smile which is the result of congenital paralysis of the left marginal mandibular branch of the facial nerve. Your left depressor anguli oris muscle does not work which is why the left lower lip is higher than the right at rest and pulls up even higher as the right lower lip when smiling pulls it to the right. While you can never make the nerve work to activate the depressor muscle you can do a vermilion advancement of the left lower lip to partially camouflage the severity of the smile asymmetry by evening out the amount of vermilion show at rest.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I have a prominent zygomatic arch that extends outward due to acromegaly. From beneath the eyes to the ear. Is it possible to push this bone inward without damaging the muscle attached to it?
A: What you are referring to is classic cheekbone reduction osteotomies…which is essentially zygomatic arch osteotomies to move the entire bow of the arch inward. This does not adversely effect the temporalis muscle which passes underneath the arch or the origin of the masseter muscle which attaches to its side.
Before such surgery it is prudent to get a 3D CT scan to plan the osteotomy bone cuts.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in XL breast augmentation 2,000 cc’s +. I’m a man, so am I a potential candidate?
A: Whether one be a male or female you can’t go from 0ccs to 2,000ccs implant volume in one procedure. The tissues simply will not immediately expand/stretch to accommodate that implant volume.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m trying to understand how the umbilical float procedure is typically consented to. When performing an umbilical float, is the informed consent modified to reflect this technique, or is the procedure generally performed under the standard mini abdominoplasty consent without any changes? I would appreciate any clarification Dr. Eppley or his team can provide.
A: I don’t know the basis of your question but in my practice the decision of using an umbilical float technique (if indicated) in a subtotal or mini- tummy tuck is preoperatively made. That decision may be based on the patient’s preoperative desire (scar avoidance), the desire to keep umbilicus at its current position (no lowering) and/or an understanding of the relationship of skin removal and the impacts on it from either the umbilical transposition or float techniques.
Dr Barry Eppley
World Renowned Plastic Surgeon
Can I Get Midface Implants If I Have Severe Maxillary Bone Loss From Removing All Of My Upper Teeth?
Q: Dr. Eppley, I’m 38 and had all my top teeth pulled for a full arch implant but I needed to go away for 4 years and experienced extreme bone resorption atrophy and increased underbite and now am not eligible for traditional teeth implants.. but my face lost volume in a crazy way I have bad bone density and my nose started sinking in my face and I have Huge nasal labial folds and my face doesn’t look right I am miserable.. can you guys help?
I’m thinking premaxilla face implants but I dunno I’m worried my bone density is an issue.
A: With severe maxillary bone loss midface implants have a much higher risk of complications due to reduced mucosal soft tissue coverage.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I recently had custom cheek implants make of PEEK with a custom guided genioplasty. I have no pain on the left side or sensibility issue. However, the right side is still numb from the lower eyelid to the upper right lip, and i can’t really move it or smile properly. I was told that it was normal at 10 days post-op, however, i still feel some strange pulsating sensation that are not very painful but still disturbing, again only on one side, it comes and goes. Moreover, the “custom” genioplasty left my chin asymetrical (please find the attached pictures. After reviewing the CT scan, I saw that one of the two screws was not put in the intended original place, but closer to the center. Could it be that the screw is in a dangerous area like the sinus cavity ? Is it normal to still be numb, and how can I see the implants on the CT scan?
A: I can not ethically comment or provide recommendations on surgical management or outcomes when the patient is under active care by the surgeon who performed the procedures..
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Would I need significant lengthening that needs surgery (>6mm) or an implant can suffice to address my concern of a smoother side profile and mental crease removal/smoothening?
A: I think what you mean is whether you need vertical bone lengthening, which is needed for chin length increases greater than 7mms. When less than 7mm is needed then this can safely can be done by an implant.
That determination requires a more indepth assessment and imaging of your pictures. But my initial impression is that 5 to 7mms of vertical length is needed.
But no matter what you do the labiomentla fold can not be ‘removed or completely smoothed out’. That is not an achievable outcome. It can only be partially reduced in depth.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I had a chin implant, which did provide some chin projection improvement, but did not achieve my ideal goals. Will a custom chin implant do better?
A: When considering different implants for an improved and more desired augmentation effect you have to know exactly what the implants are and where they are on the bone. Thus a 3D CT scan is most beneficial as it will clearly this important information. In your first surgery the surgeon guessed what will work. You don’t guess the second time as you have more information that can clearly be identified.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I was born with a webbed neck. But don’t have any syndrome that caused it, i really hate the way it looks and am trying to find options to get it done with surgery. First the only option was to have scars on both sides and i chose not to do that, then i saw your surgeries where the scar is at the back, what didn’t look bad, but i was wondering if a surgery like that would be possible for me. Hope you could answer that, thanks
.A:Thank you for sending your neck pictures. Your neck appearance is fairly classic particularly for non-syndromic neck webbing. Most neck webbing i see is not associated with a genetic proven syndrome such as Turner’s or Noonan’s syndrome. As you may well have read there are different techniques in the treatment of neck webbing which primarily can be differentiated by those that are performed laterally on the side of the neck and those that are based more posteriorly on the back of the neck. While there can be debates about which produces a more effective and sustained correction of the neck webbing it is probably true that a direct lateral approach is a bit more effective. But the visible scarring for many patients may not be a worthy aesthetic trade-off. Thus I have always used a more posterior approach to keep the resultant scars more on the back of the neck as opposed to the sides. With the posterior approach there is always going to be some amount of relapse which is maximized in the first few months after the surgery. This is usually in the amount 30 to 50% from that scene immediately after the surgery. For most webbed neck patients this is acceptable and they never move on to have a secondary revisional procedure which can maximize the results using the existing scars from the first surgery. This is the trade-off of the posterior approach. As you can see by this description no form of webbed surgery is perfect and each type has their advantages and disadvantages. I, and almost all patients, would prefer the option that better hides the scars. Once the scars are on the side of your neck with the lateral approach, no matter how they are revised, they are always going to be very visible.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in rhinoplasty to correct nasal asymmetry.
A:Thank you for sending all of your nasal pictures. I am going to assume that you have never had any prior nasal surgery and this is either the natural result of your facial development. While fundamentally what you see is nasal asymmetry there is also some development differences between the two sides. This is particularly seen in the nostrils where the right nostril is smaller and more highly position than that of the left. As a result in straightening the nose through basic cartilage and bony repositioning techniques the left nostril will also have to be reduced to better match that of the right side. This will be particularly needed given that there will be a right shift of most of the nose This will automatically make the right nostril smaller and the left nostril bigger, hence the needed left nostril narrowing needed with the overall procedure. The best nasal asymmetry results come from an open Septo rhinoplasty procedure. Whether you may also want narrowing of the nose particularly in the tip is a personal choice which you have not mentioned up to this point.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in custom temporal implants for head widening. My questions are:
1) Do you factor in the implant’s design the amount of postoperative swelling that will occur?
2) What is the usual thickness of head widening temporal implants?
3) Can you make an implant design and then show me what it will look like on myself?
4) Can I see before paying for the surgery what my implant design would look like?
5) Can you predict how much temporal fullness will be lost when the swelling subsides?
6) Can I connect the previously placed custom skull implant on the top of my head with these new custom head widening temporal implants?
7) how can I be assured that after the swelling subsides I will have the head widening amount that I want?
 A:I can answer all of his questions in advance of our virtual consultation.
A:I can answer all of his questions in advance of our virtual consultation.
1) Since these are custom implants they can be designed with any thickness dimensions as long as they can fit or be surgically placed. For the purposes of factoring in the effects of postoperative swelling one simply has to guess how many more millimeters that would be an implant thickness. There is no exact science as to how to factor in for postoperative swelling. To me what that means is maybe an additional 2 mm of thickness.
2) Since these implants would be submuscular a safe temporal with is 5 to 7 mm maximum.
3) There are no tools to accurately show people what their postoperative results may be. All we can do is use preoperative Photoshop to determine the patient’s goals. Ai is not going to be helpful as is there is no database of information about the effects of implants on an external appearance.
4) The only method to show a 3D implant design/rendering is to actually engage the implant design process with 3D Systems. They are the company that does all of that implant designing but they don’t do so until they are paid.
5) There is no known method to tell you how much fullness will be lost after the swelling subsides.
6) You can always in the future add volume to the front or back of your head with additional implants, that is not an issue and can easily be done with additional implant designs. The problem is if you try to connect the front or back to the sides where the implant must sit above the muscle on top of the fascia where implant edging and chronic fluid collections are real postoperative possibilities.
7) There are no strategies for maintaining postoperative width fullness. You pick a number that you want the implant to be and you hope when it is all done and said that it largely achieved what your with desires are.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My hope with reaching out to you, would be that you can help me find my way back to my old self. I had a deep plane facelift that took all of my volume and left me looking much older even at a full year if healing. I am interested in a custom cheek implants. I do not want an apple cheek. I have also included attached images (which are most likely phoroshopped) of the desired aesthetic look I would like to achieve. If at all possible, I would like my old self back.I do not want filler, nor fat grafting. I had micro and nano fat with the deep plane, which now gives the appearance of jowling, as my cheeks have lost volume, so it looks like areas are sagging and hollowed out, this is in my orbital area as well. I will forward those pictures revealing the poor result. Please help!
A:Thank you for your inquiry and sending all of your pictures. This is an unfortunate outcome and I can certainly understand your concerns and objectives. The soft tissues of the cheeks have lost projection (technically not lost volume, just that the volume has now been displaced laterally, strerched ad compressed by the tighter overlying skin) You are correct in that any type of soft tissue augmentation is destined to fail because the pressure of the tighter tissues will be hard to give any adequate push outward with a soft material. Only an implant off of the bone Canal provide they needed secondary projection.
The concept of the cheek augmentation that you are now seeking is largely bone based. The traditional apple cheek augmentation effect is more soft tissue based where much of the augmentation is below the actual cheekbone. You are also correct in that only a custom cheek implant design can reliably affect this type cheek projection change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What are your thoughts on the incision for the mouth widening surgery being done inside of the mouth. I know there is an option for lip corner lift and was wondering if the same could be done for this procedure.
A: To be effective mouth widening requires skin removal as it is a relocation of the vermilion – cutaneous border further out on the side of the face. Thus any attempt to do intraoral mouth widening is not going to work.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How soon post Radiesse filler can I get the jaw augmentation done? Is there a waiting period (I got it in April).
A:I am not concerned about existing filler as it does not interfere with the custom jawLINE implant design or surgical placement. Whatever filler is present will quickly be resorbed due to the swelling and inflammation from the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
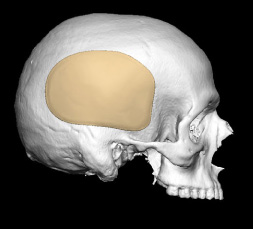
Q: Dr. Eppley, I don’t like the protruding forehead/frontal bossing and the prominent occipital protuberence… if they could be rounded a bit i hope it wud do a good job in both shape and reducing size. Thank you
A:Thank you for sending your pictures. The question is not whether the occipital prominence and the frontal bossing can be reduced… as they can. The most important issue is surgical access to do so. Typically the occipital prominence is approached placing asmall horizontal incision on the lower end of the occipital bone at the bottom of the prominence and this heals extremely well. The frontal bossing of the forehead is usually approached with a frontal hairline incision which also can heal very well. The other option is halfway between the two with a long scalp incision from the top of one ear to the other to approach both areas. Besides the undesirable length and location of this incision it also does not provide the best access to the occipital prominence.
Both procedures can be performed during this same surgery under general anesthesia. The exceptional prominence reduction is first done in the prone position and then you would be turned over while asleep to do the frontal Boston reduction in the supine position.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve been struggling with the shape of my pelvis, and I came across your page regarding iliac crest reduction. I’m currently considering pelvic contouring surgery, and I would like to ask you a few questions. As a woman, I’m concerned that my pelvis appears high and narrow, giving it a more masculine look. Would it be possible to shave or lower the upper part slightly to create a more feminine silhouette?
 A: In the high and narrow pelvis you cannot make it wider or have a more feminine silhouette by shaving down the iliac crest. This will simply make it a bit less high but will provide no width to it. The definitive procedure is the application of a titanium iliac crest implant which is designed to do exactly what you want to achieve. This implant sits on the side of the iliac crest and its entire intent is to feminize the pelvis. (see attached diagram) Such implants come in a variety of widths from 15 mms up to 50 mm. The most common widths used is 35 mm but by your own description you may not even need that amount. More accurate sizing depends on knowing your height and weight as well as seeing pictures of the thickness of the soft tissues over your iliac crest. As the widths become greater this can in some patients cause a sub iliac hollow which is which is why in the complete Pelvic Plasy procedure the titanium plate is combined with an attached silicone hip implant. But as long as the width of the implant is not too great and one does not have a pre-existing sub iliac hollow the attached hip implant may not be needed.
A: In the high and narrow pelvis you cannot make it wider or have a more feminine silhouette by shaving down the iliac crest. This will simply make it a bit less high but will provide no width to it. The definitive procedure is the application of a titanium iliac crest implant which is designed to do exactly what you want to achieve. This implant sits on the side of the iliac crest and its entire intent is to feminize the pelvis. (see attached diagram) Such implants come in a variety of widths from 15 mms up to 50 mm. The most common widths used is 35 mm but by your own description you may not even need that amount. More accurate sizing depends on knowing your height and weight as well as seeing pictures of the thickness of the soft tissues over your iliac crest. As the widths become greater this can in some patients cause a sub iliac hollow which is which is why in the complete Pelvic Plasy procedure the titanium plate is combined with an attached silicone hip implant. But as long as the width of the implant is not too great and one does not have a pre-existing sub iliac hollow the attached hip implant may not be needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Apart from mouth widening surgery, I am also wanting to replace my breast implants, I currently have 950cc silicone implants and am wanting to have much larger silicone implants (1300 or 1400cc, Mentor have just released these size silicone implants.) Would that be possible to combine the two surgeries together?
A:Yes it would. Mentor now has silicone 1140, 1240, 1330 and 1430cc implants available.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Do you guys perform temporal “reduction” surgery
A:As the inventor of temporal reduction surgery I perform it regularly. How this may apply to you requires Picture assessment as well as a description of what your estimated goals.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’d love to better understand the scope of midface augmentation. Would any of the following effects be realistic?
- Smoothing or softening of nasolabial folds (see attached photos for current nasolabial folds when smiling)
- More defined hollow cheeks / less puffiness in the midface
- A slightly wider-looking mouth through midface skin traction?
- A more angular look from subtle skin elevation near the jawline?
A:In answer to your specific questions about midface augmentation:
1) Improvement of the nasolabial folds is not going to occur with any form of midface augmentation particularly when one is smiling.
2) Depending upon the implant design it may be helpful in creating some increased submalar hollowing/indentation. However the more a short approach to that outcome is really a reductive one based on cheek fat removal.
3) The mouth is not going to get wider with any form of midface augmentation. It does not create a midface skin retraction effect.
4) mid face augmentation is not going to create I more angular jawline look. That can only occur from a direct jawline augmentation approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I am wanting hip implants. Am I a good candidate? I would be coming from Australia. How long will I have to stay in America for?
A:My extensive hip implant augmentation experience I have learned tonight place too big of a hip implant to lower the risk of potential complications. Thus the attached imaging shows the amount of augmentation that I am willing to do. Your length of time here does not need to be more than five days although, one of the important elements of postoperative recovery is the need for drains. Those drains need to stay in 2 to 3 weeks. Thus you will be going home with drainss in which we will guide you through the process of eventually removing them at home at the appropriate time.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How much would I expect the cost to be for something like Custom Orbital Floor-Rim Implant in the Treatment of Aesthetic Vertical Orbital Dystopia, for my situation? My right eye would ideally look like the left once raised.
A:First of all I do not know your ‘situation’ when it comes to your eye and asymmetry as I have never seen any pictures of your problem. Secondly in the treatment of vertical orbital dystopia a custom implant made to raise up the eye and infraorbital rim pi is rarely the sole solution to the problem. It is a foundational part of the VOD surgery but it is almost always requires other soft tissue adjustments to be done around the eye, the eyelids and brow, as raising the eyeball alone will change the lids-eye relationship in an unfavorable way. And the eyelids and brow do not move upward because the eyeball is raised. Thus it is very rare that a custom orbital implant alone will satisfactorily address the problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in a lip lift with lip reduction. Do you perform it with muscle cut under the nose too? My upper lip is already to forward and I want to avoid making it even go more forward after a lip lift.
I naturally have an upper lip that is somewhat projected forward(also had silicone injection years ago), and I’m concerned that a lip lift might increase that projection or cause the lip to appear overly everted.
I’m specifically looking for a subtle and natural result — with a shorter philtrum and better tooth show, but without making the upper lip stick out more.
Could you please let me know if your technique is muscle-sparing or including cutting,and if it avoids adding forward projection?
A:In a subnasal lift lift I never remove underlying orbicualris muscle. This not only deepens the nasolabial angle in an unfavorable manner but often causes prolong difficulty with smiling and other lip motions. Thus it is a skin only procedure in my experience.
The logic of why some surgeons remove muscle in the procedure is that it limits any postoperative relapse. While there is merit to that relapse prevention the trade-offs are not worth it in my opinion. Long term follow up has demonstrated that most primary subnasal lip lifts, depending upon how much skin is removed, will within the first six months undergoing 10 to 20% relapse of length. But this to me as a better problem then issues that can occur with muscle removal in the procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a few weird bumps on my upper head and I want them removed but how much would that cost.
A:I would need a much more description of the weird bumps (where, how many, what do they look and feel like) to determine what may need to be done to remove them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m in the UK and have been unable to find a surgeon to improve my orbital dystopia here to get an improvement in my eye asymmetry. Would I be able to send you a picture of my eyes & an image from my CBCT scan to see if you would be able to assist me? I am very nervous about considering surgery outside of the UK but would like to know if it’s at all feasible for me. I would like to get an idea of the cost of an infra-orbital rim implant (possibly combined with cheek implants). As if an implant is an option in my case I would be very keen to do so.
A:Thank you for your inquiry and sending your picture and 3-D CT scan. Almost every custom vertical orbital dystopia implant is a combination of the orbital floor, infraorbital rim, and cheek as the entire composite bone unit is situated lower. While this would be effective in your case based upon the amount of millimeters that the left eyeball is lower than the right, 5mm or less, it is important to understand that you cannot just move the eyeball alone as the eyelids are not going to follow it upward. Thus almost every vertical orbital dystopia patient requires concomitant upper and lower eyelid repositioning with their custom implant. Fortunately, your left eyebrow is minimally lower than that of your right and does not require management.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I feel like my hairline sits on top of my head because of these protruding bones in the frontal lobe. I even have a bony eyebrow ridge in the middle. Ideally I would like my forehead to be more symmetrical. Where my forehead could be lowered and I can wear lower haircuts
I have to grow my hair to hide my forehead and I want to feel confident having a lower hair cut
I would ideally like for it to sit lower with a more smoothed out forehead.
A: You have the classic forehead horns combined with a high hairline. The treatment of both are linked, meaning to get a significant forehead shape change the bony horns must be flattened and the frontal hairline advancement. The question is not whether the forehead bony horns can be completely reduced as they almost always can. The more significant question is how much can the frontal hairline be advanced, and straightened, which can never be truly known until one is in surgery performing it. The frontal hairline can be advanced, but its just a question of how much and can it really be made straight.
Dr Barry Eppley
World Renowned Plastic Surgeon