Your Questions
Your Questions
Q: Dr. Eppley, I would love some information on the crescent knee lift. I have attached pictures of my knees.
A:Thank you for sending all of your neat pictures. Unfortunately, I question how good of the candidate for a kneelift procedure you are. The knee lift is a classic example of understanding the concept of being careful about trading off one aesthetic problem for another. The obvious trade-o the knee lift is that of the scar. One has to be certain that they don’t choose an aesthetic problem that they may dislike just as much if not more than the original problem. Because of this scar concern most successful knee length patients have a lot redundant suprapatellar skin folds. While you certainly have some of that it is not excessive like many of the knee lifts that I have done. How well the scar would do in your case and whether you would consider that better than what you have now is the unknown question. Given its location and visibility one has to give careful thought to this consideration
.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there. I was doing some research and I came across your website. I have a misshaped head, very flat on the back and a little lob sided. I would like to know if and what my options are in order to fix this. Thank you in advance and I look forward to hearing from you guys 👍
A:Thank you for sending me your pictures. You have a common back of the head flatness which often has some asymmetry to it as well. Both back of the head issues are ultimately addressed by a custom skull plant-based on a 3-D CT scan of your skull. While there are limits as to how much the scalp can stretch to accommodate an implant I do not see that as a limiting factor in your case is illustrated in the attached imaging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am getting a double jaw surgery for my underbite next year and my surgeon has told me he thinks i need some sort of zygomatic augmentation to make it all look the best. Do you think i’m a good case for a zygomatic implant? Targeted to improve lateral and anterior projection for ear and flat midface. (and more obviously).
A: Rather than take any word or opinion as to what is best for you, you need to have imaging done to show the effects of any facial structural change and see what you think. You wouldn’t have double jaw surgery without some preop simulations then why would you have zygomatic augmentation based on someone else’s perception of aesthetics.
Remember that most surgeons are technicians who do operations…the more the better. Executing an operation is a different skill set than knowing if it is a good operation to do.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in the chin reduction surgery. I would like to ask more questions.
A: Your chin is long because it is horizontally short. It needs to be brought forward and vertically shortened by a sliding genioplasty procedure.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Can I see how custom facial implant designs would look on me by 3D modeling before my surgery?
A: While implants are designed using the patient’s 3D CT scan there is no accurate 3D modeling of the potential changes that may occur in any implant design. That is a common misconception about custom implants. No one has ever established a database to create these predictions accurately. These can not be extrapolated from cephalometrics, facial proportions or any imaging program.
As a result you use the patient’s desired Photoshopped/imaged changes and create an implant’s footprint and its dimensions based on experience.
But yes all such work can be done virtually and that is always how I do it.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m currently doing myofunctional therapy and I was recommended to get a marpe device, which I have a consult for next week. I’m not sure if I will be getting it, but I was wondering how this could potentially impact the midface implant?
A: No matter what they say a MARPE device is not going to stimulate forward midface growth in any appreciable way if at all.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, As you can see my ipd is wide. Does Dr. Eppley perform some sort of z-plasty or medial canthoplasty? Where the tendons are reangled or made longer in any way? Is there any way to reduce or fraud the eye spacing? Also would a lateral canthoplasty be possible for me? My downturned eyes bother me.
A: I know of no soft tissue technique that will make the eyes look closer together. Soft tissue corner adjustments can be effective for making the eyes appear further apart but not closer together.
Conversely, soft tissue adjusgtments or lateral canthoplasties can effectively lift up the outer eye corners. Depending on the amount of movement needed a lowe eyelid space graft may also be needed for a sustained change.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Regarding cheek shaving Is this only good for reducing zygomatic protrusion and does it necessarily have to do so? Is this a good procedure good for giving an illusion of higher set cheekbones?
A: Cheek reduction by shaving is almost always an ill-advised procedure as it has a minimal effect and runs a high risk of soft tissue cheek sagging.
No form of cheekbone manipulation can create a higher cheekbone look. That requires an augmentation approach.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a fairly deep labiomental groove (~6mm) and acute labiomental angle (~100 degrees). I also have a noticeably recessed (about 5-6 mm behind bottom lip) though still prominent chin. I was hoping to do a sliding genioplasty but don’t want to seriously worsen my labiomental angle and depth. I had three questions (feel free to answer any or all): (1) can vertical lengthening, combined with horizontal advancment, minimize changes to the labiomental angle in genioplasties? (2) does labiomental depth matter on its own for aesthetics, or only the angle? and (3) if you feel the answer to q1 is yes, do you have reccomended ratio of vertical to horizontal advancement that you feel maintains the inital angle? Thank you in advance for any reply or assistance you can provide.
A: In answer to your questions:
1) Any amount of vertical chin lengthening when done with horizontal chin advancement will help mitigate any deepening effect on the labiomental fold.
2) The appearance or depth of the labiomental fold is one of personal aesthetic taste. But most people, regardless of gender, do not like an excessively deep one.
3) An equal amount of vertical:horizontal lengthening (45 degree) or greater will usually keep the labiomental fold depth from getting any deeper.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there. I was doing some research and I came across your website. I have a misshaped head, very flat on the back and a little lob sided. I would like to know if and what my options are in order to fix this. Thank you in advance and I look forward to hearing from you guys.
A: Like all mishappen heads that have deficiencies (flat areas that lack projection/more rounder contour) augmentation is needed which is done by a custom skull implant designed to do so. How that applies to you requires evaluating pictures of your head taken from different angles that show these contour deficiencies.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Repaired Cleft Lip Vermilion Realignment and Insurance Inquiry Dear Dr. Eppley and Team, My name is Jessica and I am reaching out to request a consultation regarding a potential lip procedure. I am an adult with a repaired bilateral cleft lip and am currently seeking options to correct residual asymmetry and misalignment of the vermilion border. I have reviewed Dr. Eppley’s experience with lip advancement techniques, including the gull-wing approach, and I believe his expertise aligns with my needs. In my case, the concern is primarily reconstructive and stems from prior cleft surgery, rather than a purely cosmetic desire. I would appreciate the opportunity to schedule a consultation to discuss: • Whether vermilion border realignment via a gull-wing lip lift would be appropriate in my case.
A:Thank you for your inquiry and sending your picture. Amongst all cleft lip deformities the bilateral cleft is unique in that in almost all cases there is a fundamental shortness of skin between the nose in the upper lip as the pro-labial lip segment is fundamentally short/deficeint. As a result this would negate the use of any type of lip procedure whose result is dependent on skin removal such as a subnasal lip lift or vermilion advancements. While a central vermilion advancement would create more of a cupids bow shape this would also shorten the skin segment of your upper lip in an unnatural way as that skinned segment is already marginally adequate in length.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
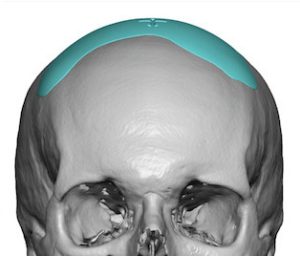
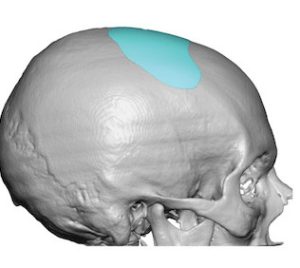
Dr. Eppley, i have a very flat forehead and protruding brown bone, the front top of my head is also flat.
A:With a flatter forehead and upper top of the head (these two always go together) this can make the brow bones look artificially protruding. Whether the brown bones should be reduced can be debated but the major benefit comes from augmentation of the flatter for head in front top of the head. (see attached imaging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I just want ur opinion as somebody who’s is attuned to facial aesthetics. I have vertical optical dystopia where my eyes are uneven, you confirmed this earlier this her. It’s hard to gauge from my own perspective. Do you think something like an optical rim augmentation would have a significant and noticeable benefit to my looks?
I just want to know whether you think it would be a worthwhile benefit to my looks? I want to become as good looking as I possibly can. I’m not sure how sigbicant my VOD is or how much a correction would knelove me, but I would really appreciate your professional opinion. If I get this survey done it would be with you. I would be interested in a virtual consultation with you to get your insights,A:In most cases of vertical orbital dystopia a combination of procedures are necessary to provide adequate improvement of the entire bony and soft tissue Perry orbital complex. That’s improvement of vertical or rectal dystopia is often not as simple or straightforward as it seems from the procedures needed to correct it. In your case however you may be the one rare example where bony augmentation of the infraorbital rim and anterior orbital floor could be effective on its own. To make a more complete assessment of this possibility I would need to see pictures of your face from different angles so I can get a true appreciation of the soft tissues around the as well as how different it is from the opposite eye. These pictures should be in the non-squinting facial posture is that distorts the eye area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello doctor I hope you’re doing well I was wondering if you provide any surgery for a barrel chest deformity for more feminine contour without and bulge or excessive broadness as it’s causing me significant social embarrassment and dysphoria thank you so much.
A:The barrel chest deformity is not a problem yet amenable to any form of known aesthetic rib modification surgery. Theoretically ribs can be shortened higher up on the rib cage then is traditionally done for other purposes. But whether that would be truly effective and worth the surgical endeavor with a longer incision on the side of the chest wall to do so yet remains untested
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would like to change the shape. I’m not sure what is the best option? The top of the head has a dip and is flat, not sure if could be burring or implant. Front forehead is also too large.
 A:Thank you for your inquiry and sending all of your pictures. You really have a combination of two skull shade issues. The first is the classic coronal dip that can occur across the top of the head along the coronal suture line. This is treated with a sin custom scholar implant that goes from side to side to provide a dip correction. This is placed through an extremely small 2 cm scalp incision. The other problem, as you have mentioned, is that the forehead is a bit pronounced and you have prominent bony temporal lines along the side of the forehead that go up to the coronal dip area. This is a reductive problem, done by burning, and while effective, presents a major aesthetic concern in that the scalp incision needed to do it would be considerably larger than that of the skull implant placement and for most me who shave their heads would probably be viewed as an aesthetic trade-off that may not be worth the benefits.
A:Thank you for your inquiry and sending all of your pictures. You really have a combination of two skull shade issues. The first is the classic coronal dip that can occur across the top of the head along the coronal suture line. This is treated with a sin custom scholar implant that goes from side to side to provide a dip correction. This is placed through an extremely small 2 cm scalp incision. The other problem, as you have mentioned, is that the forehead is a bit pronounced and you have prominent bony temporal lines along the side of the forehead that go up to the coronal dip area. This is a reductive problem, done by burning, and while effective, presents a major aesthetic concern in that the scalp incision needed to do it would be considerably larger than that of the skull implant placement and for most me who shave their heads would probably be viewed as an aesthetic trade-off that may not be worth the benefits.
Thus while both skull reshaping procedures could be done and presents a minimal aesthetic liability the forehead reduction is very different.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr.Eppley, I had double jaw surgery back in 2019, and after the swelling had gone down, i noticed that my chin “button” or so my orthognatic surgeon called it, was able to be moved around easily, and protruded way too much, and when I smile, things look even worse, it gives a “witchy” look. I never had this before double jaw surgery. He moved both my upper and lower jaws forward, and i believe he shaved down the chin a small amount in order for me to not look too projected in that area… but now I’m left with this fleshy portion that I want removed. He told me it was near impossible and it would look worse than before if I had it removed or liposuctioned out, it would sag more. But now I see your website, and it seems possible? I’m in Canada, and don’t see anything on Submental Excision/Tuck for Hyperdynamic Chin Pad Excess available in this country…. Thanks so much for your response in advance on what I can do
A:Any time intraoral chin burring reduction is done laxity of the chin pad and ptosis often results. This is why this is a relatively poor choice for many types of chin reduction. You are correct in that this is remedied buy a submental approach to chin pad reduction by excision. This is a common and effective procedure and the stated concerns about it being impossible or would look worse than before are said based on a lack have any knowledge we’re experience with such surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, The custom silicone skull implant is not soft when a hand presses on it? I am asking because the silicone implants look hollow and soft on the website and the Instagram account.It is not clear to me how the silicone can feel just like bone?
A:Like wall paper on a wall, it is flexible by itself but when placed on the wall it feels just like the wall. 9acquires the same feel mas what it rests on) You have to evaluate it in the situation in which it is applied not in isolation or free standing. It is no different than silicone chin and cheek implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, what happens when a skull augmentation procedure is two-staged as in my case? Would I be staying in the hospital this whole time? How is the scalp expanded? Would the whole procedure leave any visible scars? And where?
A:A two stage skull augmentation requires two separate surgeries spaced 8 to 12 weeks apart. The first stage is the placement of a Scout tissue expander in which the patient goes home the next day. The patient inflates their own tissue expander over several months to get to the desired volume of Skull augmentation they want. We provide all of the supplies and instructions to do so. The second stage is where the tissue expander is removed and the larger skull implant is placed. The patient usually stays overnight and will go home within 3 to 4 days after the surgery.
There will be a necessary incision for the placement of both which is done through the same one placed on the upper back of the head and usually 7 to 8 cm long. The scalp scar usually heals very well and is a minimal aesthetic trade-off.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am researching looking into Testicular implants due to testosterone therapy. My balls are very small due to the therapy.
A:Most testicles implants done for enhancement due to atrophy are done by a side-by-side custom implant technique. This is effective and lowest complication risk approach. As a general rule we want the custom implants to be at least 75% bigger in size/volume then that of the natural atrophy testicles. This is performed as an outpatient procedure under general anesthesia and the patient returns home the following day.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am indeed interested in the hip augmentation via implant. I seek is to add more width from a front/back view to my hips. Definitely give me your thoughts. Also, I read this on your website – “Secondly overall hip augmentation is the lateral zone from the iliac crest down almost to the mid-thigh area” and I believe I am looking for this exact option, which is a width increase in the entire hip complex. I also understand that there could be (and probably will be) implant edge visibility since I am so lean with very little fat mass. I already have all manner of shadows and protrusions due to my hip bones and muscles peeking out, so I’m not really too concerned with edge show. However I do train regularly (weight training), and focus on my glutes, quads, hamstrings, and TFL areas, and would love your input on how building more muscle might affect the look. I would assume that more muscle being under the fascial layer would just kind of ‘push’ the implant out a bit more. These are questions I might ask the Dr. when we have our consult. 🙂
A:Thank you for your inquiry and sending your pictures. When is a good candidate for hip implant augmentation if they meet the following criteria:
1) they have exhausted any autologous fat injection hip augmentation surgery or are not a good candidate for fat injections due to lack of fat,
2) they never have had any synthetic injectable fillers placed into the hips and/or buttock areas,
3) the zone of their desired hip augmentation area coincides with where hip implants can actually be placed,
4) they can except the aesthetic risk that most hip implants may have some degree of edging whose likelihood is based on the thickness of the subcutaneous fat layer over the implant which is placed on the deep temporal fascia,
5) that their desired amount of hip augmentation is not excessive as large hip implants are associated with much higher risks of complications beyond out of just implant edging. As a general rule that means the maximum thickness of the hip implant should be under 2 cm and preferably closer to 1.5 cm. (see attached imaging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q Dr. Eppley,I researched where I could get surgery to increase the si ze of my thighs and legs (with silicone implants). And I found you. What would be the total cost of plastic surgery? This is my hip and it bothers me a lot that my butt is V-shaped (due to liposuction) and my legs are thin and disproportionate to my hips and I would like to correct it 😕 thanks for your attention! God bless you
A:Thank you for sending your pictures and illustrating by the red lines the area that you want to augment. You are correct in that would be considered the lateral thigh area and or very low hip area. Technically anytime you get below the greater trochanter of the femur bone it is considered the lateral thigh area. You are also correct, are in the lack of any fat to inject, that implants would be the most reliable way to augment that area. The maximum width of the implants based on your drawing appears to be in the 2.0cm range. However that would also depend on your height and weight which is obviously not evident in the pictures.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m looking into getting a facial fat graft under the eye area. My question is, if I lift weights at the gym 1 week post op will this prevent the fat from engrafting? Can it cause the fat to die or move around? Please let me know.
A:The understanding of the biology of fat transplantation currently remains incomplete. It is not clearly known whether high levels of metabolic/physical activity after fat grafting positively or negatively impacts its survival. It certainly does not affect it’s location of where it is placed (will not make it moves) and I suspect it does not have any negative impact on how much of the fat graft survives.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For my right shoulder implant(s) for deltoid muscle atrophy which is better…measured custom or a D custom implant approach? Which one do you think is more beneficial. Cost is not an issue, I just want to know which is better and why.
A:3D custom body implants, designed by the patient’s 3-D CT scan, would provide an accurate estimation of size and volume of the lost muscle mass in the right shoulder. This would be the appropriate treatment approach if the patient wanted a very precise estimation of the volume and shape of the muscle mass to be replaced and wanted to be able to see that visually. This also refers to the type of patient that views their surgical reconstruction as a mathematical engineering project.
Conversely designing the muscle restoration implants for the right shoulder based on external measurements and prior patient implant designs with a similar problem is for the patient who can accept that such is surgery is an approximation update volume of muscle mass that needs to be restored and are happy with substantially reduced asymmetry and that perfect symmetry between the two shoulders cannot realistically be obtained. There’s also for the patient who has more economic constraints.
All of that being said the result differences between the two methods is probably not dramatically different.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve been looking into treatment options for my sunken under-eyes—potentially fat grafting?
A:Thank you for sending your pictures. You’re under eye hollowing, which primarily occurs along the infraorbital bony rim, can be treated buy a multitude of methods from fat injections to various implants placed along the bony rim. Each of these two fundamental approaches has their advantages and disadvantages. Injection fat grafting is by far the most commonly performed procedure for this problem and represents hey minimal invasive surgical procedure with little recovery. Its disadvantage is the unpredictability of How much fat survives and whether it will have a smooth contour. In other words irregularities or lumps and bumps are well-known to occur from fat grafting underneath the lower eyelid and upper mid face skin. The use of the implants to build out the informant to ram is a true surgical procedure and with that a more significant recovery of swelling and some bruising. There is a range of different implant options from tissue bank dermal grass to various forms of implants including custom-made implants. They have the advantage of adding a permanent volume with a much higher likelihood of being smooth throughout the augmented area.
The debate, of course is which one is better and that depends on both the patient’s anatomy and the patient’s preferences. The ethnicity of your facial bone structure is such that you have a flatter midface projection and, as a result, would be better served long term with a more assured permanent augmentation approach. The debate then becomes what type of material is best to use. From my experience this comes down to whether the patient wants to use something off-the-shelf or whether one wants to use a custom implant approach. That would be dictated by the patient’s preference and economic considerations.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, In general, I feel like my head is too small for my body (I’m 5’7’’ and about 150 pounds).
It’s kind of flat at the top and at the back, I feel like it lacks that roundness and volume at the top, I try to cover it with hairdos, fangs and such, I look more harmonious when I add more volume there.
As for the back of my head, it just seems as if the parietal bone simply didn’t develop enough in length and my head seems way too short, which doesn’t help the way my chin projects either.
A: By description and your pictures, you are describing a classic female top crown in back of the head, augmentation, basically between the two hairlines and the bony temporal lines to the side. Unless one only needs a few millimeters of implant thickness this would require a two-stage skull augmentation approach with the first stage being scalp expansion to accommodate a larger implant. This is particularly needed in blond and light brown haired Caucasian females, who often have the thinnest scalps which stretch the least.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a defibrillator but could I get breast implants under the muscle ???
A: When a patient is considering breast augmentation with an indwellng on demand pacemaker or a defibrillator the followiong three pieces of information are needed:
1) Medical/cardiac history
2) Operative notes from the device placement
3) AP/Lateral chest x-ray
From this information it can then be determined whether breast augmentation in general and what implant pocket location is possible can be determined.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can the Pelvic Plasty procedure give stability to a females hips? I want to know if it will alter my balance.
A: The Pelvic Plasty procedure is an aesthetic augmentation procedure of the hip bone (iliac crest) and the subiliac soft tissue hollow. It is not intended to be a functional procedure (stabilize the hips) but it also does not compromise hip bone stability either.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, may I ask what materials are used in 3D printing? Is it primarily silicone?
A:3D printing can use virtually any material so that should not be the basis for choosing an implant material. You choose an implant material based upon the most overlooked property by patients and surgeons alike… and that its ease of secondary reversibility/modification. When you look at the statistics of all types of facial implants the need for secondary revision and/or replacements approximates 40%. That shocking statistic, which is not shocking to those of us who do this work every day and most of these revisions or modifications or for purely aesthetic purposes, is a rank reality have any type of aesthetic facial implant surgery. Besides being able to achieve the desired aesthetic result you now can appreciate why the ease of placement, removal and/or replacement becomes the single most important implant material property.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I have had a sagittal bump reduction done in 2023. The bump gradually reocurred and reached the same extend 2 years after the procedure (pictures). If surgery was performed again: Is reocurrence as likely and are there any preventive measures?
A:Recurrence after a sagittal skull reduction, or any form of skull reduction, is not a postoperative phenomenon that I have ever seen. In looking at your pictures that is a fairly prominent bump which should be able to be completely reduced. The location of the scalp incision to do it is a bit unusual in my experience both in location and incisional length. For such a skull prominence to have ‘recurred’ it was either never really completely reduced and only long term swelling prevented it from being initially seen or it was adequately reduced and due to failure to place a sealing agent over the open reduced bone recurrence has occurred. However in looking at the shape of the sagittal bump ‘recurrence’ that looks like to me probably what the original sagittal bump looked like.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am looking for a specialist for a mentalis/lip resuspension after à terrible génioplasty years ago. But if you have a real beautiful solution to my problem ( I cannot close my mouth, the lower lip is far too low in the resting position etc…) Here are some photos.
A:Thank you for your inquiry and sending your pictures. The need for mentalis and chin pad resuspension almost always comes from prior chin surgery, albeit bone or implant related. I have performed many mentalis resuspension surgeries and it proves to be a challenging operation to achieve sustained uplifted results. It is done through a variety of intraoral resuspension techniques and, despite technically well executed operations, some patients do not maintain long term results. That being said there aren’t really any other options you Treat your problems than this surgery. It would be helpful to see hey lateral x-ray of your chin to show the shape of the bone in any hardware that may be present. This does not necessarily alter one’s candidacy for the surgery but it can provide some helpful insights as to what technical maneuvers need to be used.
Dr. Barry Eppley
World-Renowned Plastic Surgeon