Your Questions
Your Questions
Q: Dr. Eppley, I have a patient who had chin surgery and had a problem with her lip not closing properly. She is interested in going to the USA for further treatment.
She would like more information to help her make a decision, for example:
- Can this condition be cured?
- How confident in your ability to treat this condition?
- Estimated cost?
- When is the earliest time of appointment for surgery?
This email has attached patient information without identifiable personal information for your consideration.
A: Thank you for your inquiry and sending all of the patients information which is very comprehensive and complete. Given the patient’s prior reductive chin surgery it is not surprising that lower lip incompetence has occurred. This is a very common history for it. Between scarring mand the loss of bony support. The treatment for lower lip incompetence is challenging. In terms of obtaining consistent, successful results. This is particularly so when the size of the chin bone has been reduced.
In answer to your specific questions;
1) The chance of complete cure of lower lip and competence is not high. It is best to view the outcome as improvement. A complete restoration of the lower lip position as to what it was prior to any chin surgery is unlikely. Early surgical results are always favorable. But long-term results at 3 to 4 months out is the real outcome of the surgery and it rarely is as good as it looks in the first few weeks after the procedure.
2) As a result my confidence in a highly successful outcome is low.
I make these comments based on an extensive experience with this problem and the surgery to treat it. I would not want any patient as to the outcome. Some patients do have very good results while others do not. It remains a bit of a paradox to preoperatively determine whom those more favorable patients might be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to know if it is possible to reduce the height of the head by reducing the size of the forehead bone, as well as reducing the size of the sides. I would also like to know if it is possible to change the general shape of the head and restore those areas that need it.
A: Thank you for your inquiry and sending your pictures. In answer to your questions:
1) The most important area of skull reduction would be its height or what you have called the height of the frontal bone. The question is not whether it can be reduced but will the thickness of the bone allow for a visible height reduction. Only a 3D CT skull scan can answer that question accurately. We would need to measure on that scan the thickness of the bone and see how much can be safely removed. There is the issue of whether a scalp incision and resulting scar across the top of your head would be a worthy trade-off if improvement could be adequate. But that question is secondary to will the bone thickness allow for it.
2) The sides of the head are an easier decision to make as the temporal muscle will almost always allow for the convex side of the head to be made straight. But that is a question that can be confirmed by the 3D CT scan.
These two head shape issues are intertwined as if you reduce the sides of the head without making any changes to its height it will look even taller. So the determining issue is the viability of the height of the head reduction.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Can you also ask the doctor that since cheekbone reduction involves the use of pins/screws and plates to secure the cheekbone, can these get knocked loose if there was blunt force facial trauma?
A: Hardware loosening in cheekbone reduction osyteotomies is generally a risk that would most likely occur if substantial facial trauma was sustained in the early healing phase. Once the bones are healed, hardware would be very unlikely to become dislodged by trauma.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I came across your articles last night and was stunned at the depth of your knowledge and expertise. I look forward to being in contact! Procedures/areas of interest (individualized pricing/imaging for each as well as combined would be greatly appreciated but I understand if that is asking for too much): Lip reduction/augmentation – Desired result: more balanced lip size, more defined shape at neutral facial expression Brow bone augmentation/Lateral canthoplasty – Desired result: Hunter eye look you describe. More masculine and appealing upper third/eye area. Custom infraorbital-malar implant – Desired result: higher cheekbones, more definition and masculine look. Custom mandibular implant – Desired result: Emphasis on chin augmentation, adding squared shape and projection both downwards and from the side profile. Widen jaw angle. Not opposed to the idea of buccal area work or chin/jaw/neck lipo if you feel it would enhance/more efficiently achieve the desired results. Thank you so much!
A: Thank you for your inquiry and detailing your numerous facial enhancements. That is a long list of options and the prudent way to approach it is to first create a priority list of the most important to least important and then pass that along to me with some facial pictures (front, side and ¾ views) so I can do some imaging a potential changes in these areas. The priority list will also allow us to answer your cost questions, and based on assessment of your pictures, I would have a better idea as to exactly what the details of those procedures would be.
When, considering a potential facial reshaping makeover establishing the patient’s priorities is the first productive step.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m wondering what skull reshaping options there are for plagiocephaly. I would be interested in augmenting the back right side of my head, slight augmentation on the top left side, as well as bridging what I would describe as a divot/dent at the top just above the forehead, as well as reducing the top right forehead and right side a bit due to being pushed forward. I would be interested in the best implant options for the augmentations, as well as the feasiblility of bone burring etc for the reduction.
A:Thank you for your inquiry. All of your skull shape concerns that you have described are common in plagiocephaly. As you have mentioned in your inquiry the two deficient areas can be successfully augmented by custom skull implants based on your 3-D CT scan. The more protrusive right forehead can also be reduced by bone burning. How much reduction needs to be done and can be successfully completed would be determined by measurements on your 3-D CT scan.
The question is not whether all of these skull areas can be treated with overall improvements. The two pertinent questions are how much effort do you want to put into it (cost) and how much scalp scar burden can you tolerate to do so. These two questions are the defining parameters for your consideration in the treatment of your plagiocephaly. The latter question requires a virtual consultation to clarify. The first question will be outlined by be addressed. A very helpful thing to do when one has a multi-area skull shape concerns is to establish a list of priorities from the most important to the least important. As I have just mentioned the question is never whether you can do all of them but what is the effort versus reward ratio.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Dr. Eppley, Do most cheekbone reductions result in a bony union? Are there some that result in a fibrous union?
A:With plate and screw fixation there is a high probability of bony union. Without it a fibrous union will usually result. Whether it really matters that a bony union results in a midface bone which is a non-moving structure and has no masticatory function can be debated.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my eyes are pretty far apart and my bizygomatic width is narrow-average. This throws off my face a ton. Is there any way to widen the cheekbones with implants? If yes, how much mm width could you possibly get?
A: Increasing bi-zygomatic with is done by zygomatic arch augmentation using custom made implants. The amount that the zygomatic arch can be augmented is essentially unlimited as defined by the size of an implant that can be placed and what almost any patient would need. I have augmented the zygomatic arch in some patients by as much as 1 cm per side which would likely be way beyond what is your aesthetic needs would be. Most patients likely would only need 3 to 5 mm per side to achieve their facial widening objectives.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Injectable filler found during chin implant surgery can be removed, and will not sit on top of the augmented chin and cause overprojection?
A:Filler that presents itself in surgery would be removed because it is visualized. Any non-visualized filler would remain and would need to eventually dissipate by the normal resorption process which is highly accelerated by the trauma of surgery in the overall inflammatory healing response.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a buccal fat removal with liposuction almost 5 months ago and I ended up like this. I need to know how this can be fixed.
A: Submalar hollowing caused by buccal at removal is treated by a fat injection approach in the majority of patients. This offers the least invasive approach with the understanding that the survival of fat injections is not completely predictable. The other alternative is the intraoral placement of a dermal – fat graft put back directly into the buccal space. This is the least common approach as it is more invasive than requires and excisional harvest site. That is a more viable option in your case them and many other patients by an intraoral cheek procedure that you would be doing anyway. I am not saying that this is the ideal procedure in your case, just that in doing cheekbone reduction osteotomies the buccal space could be conveniently visualized.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Please Dr. Barry Can we ask please that question which is With Which kind of Breast Implant’s type is can someone achieve XXXL sizes with Overfilled Saline or Expanders please  ? Thank you
? Thank you
A: Silicone gel breast implant sizes are now available up to 1430ccs.But perhaps the question may be can one go from no implants to an XL implant volume in one surgery….that would be very unlikely for most women.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,What kind of Breast Implant’s type can someone achieve 2000cc or more cc with Overfilled Saline or Expanders or has to be ordered Custom size Silicone gel Implants like 2000cc Custom Silicone gel ones or more?
A: There are no custom made silicone breast implants which is not allowed per the FDA. Thus the only way to get to 2000ccs by tissue expansion and overfilled saline breast implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am inquiring about rib removals 10-11-12 or only 11-12? Does it matters how old i i’m because I’m gonna turn 20? I don’t know if you speak Greek but I send a little bit of Greek to see if you are from Cyprus.
A: I am neither Greek nor Cyprus but I do love halloumi cheese!
Age is irrelevant when it comes to rib removal surgery. What matters is one’s body type and are they favorable for good results from the surgery. In that regard I would need to see some pictures of your torso/body.
What you are asking is the difference between Type 1 and Type 2 rib removal surgery. Type 1 is where subtotal removal of ribs 11 and 12 are done. Type II is subtotal removal of ribs 10, 11 and 12 are done with a slightly different incisional location.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a young male experiencing significant psychological distress due to the shape of the back of my head. Specifically, I have a prominent occipital bone (possibly an occipital knob or bun), which creates a visible bulge at the back of my skull. This prominence causes me extreme self-consciousness in public, especially when viewed from the side. It affects my confidence, posture, and quality of life. I’ve tried many non-surgical solutions — like posture correction, adjusting hairstyles, and wearing hats — but none have fully hidden the bulge.
I’m interested in a permanent surgical solution to reduce the protrusion. I’ve seen that there are procedures like “occipital bone reduction” or “skull reshaping” using burring techniques. Could you please let me know if you offer this surgery?
A: Thank you for your inquiry and sending your pictures. What your picture show is overall occipital bone enlargement rather than a specific knob or bun. At least that is the way it appears in the side view picture. You have correctly identified that skull bone during reduction is the technique used to treat it. The question is not whether it can be so treated but how effective would it be given the thickness of the occipital bone. As a result X-rays are needed so that the occipital bone thickness can be measured from which I can make a determination as to how much reduction is possible and would the surgery be worth it (make a visible difference). A playing lateral skull x-ray is the minimum imaging needed. Ideally a 3-D CT scan would provide the most comprehensive data and ability to do a complete analysis of the entire back of the head bone thickness.
I am very familiar with this type of skull reshaping surgery since I am basically the one who invented it and has the most worldwide experience in doing it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
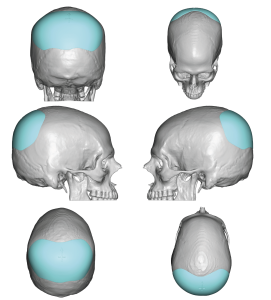
Q: Dr. Eppley, Based on what you described — that it is a pseudo sagittal crest caused by side deficiencies — I would like to ask your opinion on what you think would give the most balanced and natural-looking result.
I am looking for an improvement that makes the top of my head appear smoother and more even overall, not just a small reduction in the crest.
In your experience, would parasagittal augmentation alone be enough, or would a combination of crest reduction and augmentation be best?
A:As the attached imaging demonstrates, in which only bilateral parasagittal augmentation was done, the achievement of a smoother more even top of the head does not require any bone reduction at all. This imaging illustrates that what you have is a true pseudo sagittal crest, it only looks that way because the bone next to it is deficient.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Do you have a surgery that can reduce the skull circumference? Thank you
A:In answer to the question if is there a surgery that can reduce the skull circumference the answer is maybe. While such procedures as temporary reduction do an excellent job of changing the shape of the side of the head and occipital reduction procedures also do a very good job of reducing excessive backward projection I do not judge their results by a measured reduction in head circumference. While some head circumference is undoubtably achieved the purpose of the surgery is to make a visible head shape change which is always more significant than any linear measured reduction.
This is a general statement and how any of it applies to you requires patient specific information, including pictures, to provide an informed response.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, This is regarding Occipital Skull Reductions: It takes how many days to cool the pain after surgery.
A:In almost all skull reduction procedures postoperative pain s not a major issue. The bone itself has little feeling and the overlying scalp is often for a period of time after the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, just wondering if I would be a good candidate for frontal bossing (forehead horns) and hair like lowering surgery?
A:Thank you for your inquiry and sending your pictures. I don’t think there is any question with the prominence of the frontal bossing and the high hairline that the combination of a frontal hairline advancement with bony reduction of the bossing/horns would be the appropriate procedure. Either one without the other would not be as effective. The key to this combination is the frontal hairline advancement in which the amount that it can be advanced depends on the natural laxity of the scalp. In other words how much can the scalp be released and brought forward. Also how much frontal advancement do you desire or, to put it another way, how much frontal hairline advancement do you feel makes the procedure worthwhile? In that regard I always ask patients to draw a line on the upper forehead as to where they would like the frontal hairline to be. Based on that information then we can start to answer the question if it possible and would it require a one vs a two stage procedure (i.e., a first stage scalp expansion) to do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is there any way to widen lips surgically without leaving scars?
A:No. Mouth widening exerts its effects by external skin removal, relocating the corner vermilion-cutaneous junctions. Thus the external excision leads to a fine scar line around the corners.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in your chin augmentations. I was wondering if derma filler needs to be removed before the procedure, it is not a lot. And if this is possible to be done during the augmentation.
A:I do not usually recommend or feel the need for removing injectable fillers from the chin in any form of chin augmentation surgery. It does not interfere with the surgery and often, if it is placed out of the bone level, it will be discovered in surgery and will be removed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I just wanted to see if this was possible. My lower facial third is 79.4mm. My middle is 60.3mm. My top is 47.6mm. I was to decrease my bottom lip to chin which is at 52mn by 10mm. With a slight burr shave backwards 2mm. I had a sliding genio double jaw surgery several years ago that corrected my underbite but left my lower chin still big and overly projected. I’m aiming for a heart-shaped lower face, so I’d like to reduce my chin vertically by around 9mm and have the chin tapered in width to create a clean, V-line look. Also, if possible, I’d like the chin to be set back just a little — maybe a few millimeters 2-4 — to help with projection. I feel like it slightly juts forward and would look more balanced if it sat closer in line with my lips.
A: With the large chin bone reduction numbers you have described you are not factoring in what happens to all of the overlying soft tissues with such a significant chin bone removal is done (aka loss of support). No matter how that amount of chin bone is done, whether by intraoral wedge removal or a submental inferior border chin shave the residual soft tissues are going to be a potential problem. I would agree that with the prior procedures a submental chin reduction approach would be the most effective because the residual soft tissue chin pad access could be effectively managed. However the key to that being successful is closer to a 4 to 5 mm of vertical reduction with 2 mms of horizontal projection reduction. This is a good example of when it is wise to except less of an aesthetic outcome than you ideally want to avoid other aesthetic issue trade-offs. In this case it is about controlling the length of the submental scar for the soft tissue chin pad reduction
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hey, I’m about to schedule a MARPE producer; could you check with Dr Eppley to see if my mid-face implants will interfere at all with that?
A:Common question and they will not. While MARPE through the use of mini- bone anchors helps expand the palatal arch such a change is slow and does not place any midface implant at risk. Conversely the midface implant will also not affect the ability of MARPRE in its palatal expansion process.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How many months after the mouth widening surgery can you get the revision surgery. And what can you do to get the best results if I am prone to mild hypertrophic scaring. Would I benefit from this kind of procedure? Is it possible to get an after pictures of a patient with hypertrophic scaring and revision?
A:Thank you for your inquiry and sending your picture. Based on this picture that the average with of the mouth is usually at the horizontal level of the vertical line drop down from the pupil of the eye I can certainly see why you would have an interest in mouth widening surgery. Based on your skin type you are not really at a risk for hypertrophic scarring as a Caucasian. But the mouth widening procedure by being done at the corners of the mouth is prone to scar widening in any patient of any skin pigment. As a general rule you don’t want to undergo scar revision shouldn’t be needed for 4 to 6 months after the procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in getting a cheekbone reduction surgery for my wide/high cheekbones. However, I am concerned about the strength of the zygomatic bone after the reduction surgery. I participate in many non-competitive contact sports, such as kickboxing and soccer. If I get cheekbone reduction surgery and, after full recovery, I get struck by a ball in the face during soccer or a punch to the face during a kickboxing sparring session, would that compromise the integral strength of the cheekbone?
A:While cheekbone reduction surgery does cut the bone and move it inward at both ends once the two ends are fully healed there is no clinical evidence to indicate hat it makes it weaker or more susceptible to fracture from facial trauma. Given that cheekbone reduction surgery is done almost exclusively in young patients, both male and female, I have yet to see any reports of a secondary fracture from facial trauma in these treated patients. I think the anatomic reason is that once the cheekbone has been moved inward there isn’t much subzygomatic space in which to move further.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a cosmetic concern with my skull. It lacks a bit of volume at the back of my head (a bit flat), has a small bony ridge at the top of my skull, and a slight depression on the front right side of my skull. I wanted to know if flexible implants could be placed in my skull and skin…to smooth out the irregularities? I’d like to know what the budget would be, and how much downtime would I need?
A: Such described skull shape issues are very common in my experience for which custom skull implant designs are the optimal way to treat them. For now I will assume that the small bony ridge, the back end of this sagittal crest, does not need to be reduced. That is what we will base the initial cost estimates of the surgery on. When it comes to downtime from skull implant surgery the recovery can be a remarkably quick because the skull bones are not functional moving bones. Thus recovery’s Is about the swelling of which the majority has gone down significantly to have a more normal appearance in public in 7 to 10 days after the procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to you today to inquire about a personal condition and the possibility of surgical correction. I have a skull deformity characterized by indentations on both sides of my parietal bones, located on the upper back portion of my head. This condition makes the back of my head appear pointed.
I am very interested to know if a surgical procedure exists that could correct this and restore a more conventional head shape. If so, I would be grateful for any information you could provide regarding the potential risks associated with such a procedure, as well as an estimate of the associated costs.
For your reference, I have attached CT scan images of my head to this email.
Thank you for your time and consideration. I look forward to hearing from you at your earliest convenience.
 A: Thank you for your inquiry and sending your 3-D CT skull scans. Such skull indentations are not uncommon in my practice experience and the use of custom skull implant designs is the best way to successfully treat them. While the specific skull implant design in your case is yet to be determined the attached image gives you a general concept of that implant augmentation approach for your type of skull deficiency.
A: Thank you for your inquiry and sending your 3-D CT skull scans. Such skull indentations are not uncommon in my practice experience and the use of custom skull implant designs is the best way to successfully treat them. While the specific skull implant design in your case is yet to be determined the attached image gives you a general concept of that implant augmentation approach for your type of skull deficiency.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I have a question. Im very unsatisfied with my upper head. My forehead is very thin at the top and extremely rounded. Can I make it wider. If yes how.
As you can see If I Take my Hair Up I have a thin egglike head. The Pictures doesnt do this Justice. In reality its even thinner. It bother me so much.I would Like to have the forehead wider on the upper left right corners
So ist could be more balanced to the face and doesnt Look Like a thin egghead ist Something Like this possible. Any Risks?
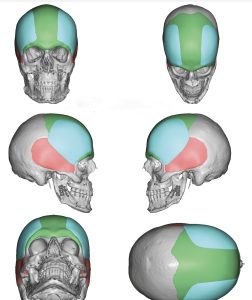 A:Thank you for sending pictures of your forehead. Now that I have a clear understanding of your specific narrow for had concerns the attached images show the type of custom forehead widening implants that are needed in your case. Ignore the green coloring of the underline for head bone which is done to show the contrasting difference in that the implant colors.
A:Thank you for sending pictures of your forehead. Now that I have a clear understanding of your specific narrow for had concerns the attached images show the type of custom forehead widening implants that are needed in your case. Ignore the green coloring of the underline for head bone which is done to show the contrasting difference in that the implant colors.
In my extensive aesthetic skull implant experience the most significant risk of the surgery is aesthetic in nature and with this type of implant in particular that of implant edging. When you expand or widen the bony temporal it is necessary for the implant to cross over that line onto the deep temporal fashion to make that type of change. Usually that risk is low and an important part of the implant design to have feather edging and to not try to make it excessively wide. You would be surprised how much 3 to 5mm of projection at the expansion point does on a bilateral basis. In other words your original estimates of 1 cm, provided you mean that on a bilateral basis and not on each side, is probably an accurate estimate of what is needed to make an effective change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if it was possible to combine 3 cranial implants in 1? Forehead, occipital and parietal instead of 3 different procedures or 3 different implants? If so how much would this type of procedure cost usually? Thanks a lot in advance. If the patients scalp can manage it, would it usually be combined into 1 singular implant instead of 3 pieces?
A:To answer your skull implant questions, whether you would need to separate forehead occipital and parietal implants or whether they would be combined as a single implant is yet to be determined. That is more of an aesthetic question based on the volume of each implanted area and do they need to be connected for a smooth skull contour. But whether it is a single larger implant or three separate implants they certainly would be done in a single surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, is it possible to remove the gap I have in the glabellar area?
is it possible to make it look like that guy? what bothers me is that hole in between my eyebrows.Thanks.
A: If the deep frontonasal angle is the primary issue that is always going to require a bone graft or implant to help push it out. Reduction of the brow bone protrusion at the frontal side of the angle is complementary to that effect. ..meaning it helps open up the angle as well.
But will it ever look like your ideal mage….no. Your anatomy is way different.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Please see pics of my legs. I would like both thigh and calf implants. The calf implants are to be long to give my lower leg thickness as my present calf muscle is very short
For the thighs it overall thickness
My legs are too skinny . I am 5ft 6in.
Will implants with fat graft be the solution?
A: Thank you for your inquiry and sending your leg pictures. I think when it comes to the concept of increasing overall leg thickness that implants are really spot augmentations, or in the legs, a linear line of augmentation. They do not per se create overall thickness, although they can create the perception of a thicker or bigger leg, because of its linear line of augmentation.
When it comes to your calfs with the muscle, being short, or limited to the upper half of the leg, that implant augmentation needs to be longer than the muscle. The only way that can be done is to have an implant that is placed above the muscle on top of its fascia at the subcutaneous level. Fat grafting is not an option for you, since I doubt if you have enough fat reserves to harvest and fat survives very poorly in the lower half of the leg anyway.
Although your thighs have not been included in your pictures, thigh implants are restricted to the rectus femoris and vastus lateralis muscle unit on the anterolateral thigh.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Could I get a wider forehead with only fillers?
A: For a significant and smooth forehead widening fillers will not be effective. That is simply not the role that the use of an injectable soft filler is meant to do.
But there is always one way to prove or disprove whether fillers will work…try it and see.
Dr Barry Eppley
World Renowned Plastic Surgeon