Your Questions
Your Questions
Q: Dr. Eppley I would like to know how many centimetres each side may be lengthened using the bilateral lengthening technique. I heard it to be one inch on each side. I would like to gain two inches on each side. Would I need to have the procedure done twice to reach my goal? If so, whats my recovery time and how long will it take between surgeries?
A:To provide clarifications on the clavicle lengthening procedure;
1) The maximum clavicle lengthening per side with current technology is 15 to 20 mm (less than one inch)
2) clavicle lengthening can only be done one time and cannot be repeated twice.
Thus what you want to accomplish cannot be safely or effectively achieved with the current method of clavicle lengthening based on my experience.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if you could please provide an assessment, based on the photos attached, as to whether you think I would be a suitable candidate for a chin implant. I am considering a vertical chin implant from Implanttech, to add to both horizontal and vertical projections. The only concern that I have is that it may accentuate the labiomental fold which is already moderately deep in my opinion, as I do not want to end up with a witch chin. If not a chin implant, I will start considering sliding genioplasty instead as an alternative. Grateful for your valuable opinion. Many thanks in advance.
 A:Thank you for sending your pictures. When you have a primary vertical length deficiency of the chin, primary meaning that the need for vertical lengthening is greater than the need for horizontal advancement, this always poses challenges that most standard chin implants cannot overcome. While there is one style of standard chin implant, the vertical lengthening chin implant, it has imitations. It was developed years ago and extensive experience with it has demonstrated that in almost every case itx shape is going to have to be modified so that is not overly round. It also has a set amount of horizontal and vertical lengthening, which are equal, and as a result most of the time is also have to be modified to fit the patient. The standard vertical chin implant has its role in chin augmentation but the reason to use it is economic, meaning one chooses it not because it is the best approach to the problem but because it costs less than the better solutions.
A:Thank you for sending your pictures. When you have a primary vertical length deficiency of the chin, primary meaning that the need for vertical lengthening is greater than the need for horizontal advancement, this always poses challenges that most standard chin implants cannot overcome. While there is one style of standard chin implant, the vertical lengthening chin implant, it has imitations. It was developed years ago and extensive experience with it has demonstrated that in almost every case itx shape is going to have to be modified so that is not overly round. It also has a set amount of horizontal and vertical lengthening, which are equal, and as a result most of the time is also have to be modified to fit the patient. The standard vertical chin implant has its role in chin augmentation but the reason to use it is economic, meaning one chooses it not because it is the best approach to the problem but because it costs less than the better solutions.
In vertical chin lengthening the better approaches are either a bony genioplasty or a custom vertical lengthening chin implant. Each of these has their benefits and it is important to understand their differences. In the bony genioplasty the amount of vertical lengthening is essentially unlimited and there is never any concerns about the soft tissue chin pad following the bone downward. Its primary aesthetic limitation is that it cannot widen the chin or make it more square which for some men may be an issue. In a custom chin implant the amount of vertical lengthening achievable is in the 6 to 7 mm range because of the need for the soft tissue chin pad to be able to be redraped over the implant once it is released for implant insertion. In a custom-designed implant it has the advantages a precise control over the amount of vertical and horizontal changes as well as the shape and the placement a Screw fixation holes.
That being said and how it applies to you, based on my initial imaging which may or may not be an acceptable amount of change, you really have the option of either the bony genioplasty or a custom implant if you prefer to go to the best solution approach. Your chin augmentation dimensional needs fall within the scope of what both approaches can do with the understanding of the aesthetic differences between them
In regards to the labiomental fold it is important to understand that any form chin orientation done either by the bone or an implant is going to deepen it to some degree. This is unavoidable as the fold represents the insertion of the mentalis muscle which sits above the effects of any form of chin augmentation. The advantage of vertical chin lengthening is that it does help to mitigate the labiomental fold deepening effects. The deepening comes from the horizontal advancement and the vertical lengthening helps decrease that effect as it pulls the soft tissue chin pad downward. It would also be fair to say that the bony genioplasty more favorably decreases the labiomental fold deepening effect as it has a more downward repositioning of the soft tissue chin pad.
As an ancillary comment to the effect of chin augmentation in your case, you ideally would benefit from submental liposuction to optimally improve the cervicomental angle and avoid a double bubble profile result.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My lips (upper and lower) have been drying and cracking for long time now and the vermillion border is damaged . Topical applications dont help because the whole skin is eroded and turns sore and painful. without topical application it geta scabby and very tight i cant move then.
A:Thank you for your inquiry and sending your pictures. What you are describing is chronically damaged dry vermilion which can clearly be seen in your pictures of which the lower lip appears to be more severely affected than the upper lip. The surgical treatment is to remove the damaged part of the dry vermilion in a lip reduction procedure which is done for symptomatic relief rather than primary esthetic purposes. By so doing you will either improve or completely solved the problem based on how much of the Involved dry Vermilion can be safely removed. This is done at the expense of some reduction in your lip size as well as a fine line scar at the wet – dry lip junction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
 Q: Dr. Eppley, I am interested in making my jaw angles more angular like your attached result. How long is the recovery and how much pain is there?
Q: Dr. Eppley, I am interested in making my jaw angles more angular like your attached result. How long is the recovery and how much pain is there?
A:Thank you for your inquiry and sending your pictures. What you’re asking about his vertical lengthening jaw angle implants. This is the most common jaw angle implant style used in women. While any procedure that involves elevation of the masseter muscles over the jaw angle area causes some postoperative discomfort the bigger issue of which to be where is the significant swelling that will result and that it will take two to three weeks until your face look better with the full final result taking 6 to 8 weeks after surgery to be more fully seen.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I get mouth widening surgery?
A: Your mouth is a bit narrow but what really magnifies that is that the vermilion of the upper and lip thin out/disappear before it gets to the corners. This always makes the mouth appear more narrow than it really is. If the upper and outer vermilion is advanced this not only changes the shape of the lips but also makes them appear somewhat wider. (see attached imaging) The point being is not usually a good idea to try and widen the mouth there is a lack of vermilion at the corners. All this does is make the corners look like narrow slits. There is a balance between the mouth width and the vermilion fullness in creating a better looking mouth shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I think my forehead is very small and it bothers me a lot and I want to fix it and also the back of my head is flat and I wanted the doctor to look at it.
A: Thank you for your inquiry and sending your pictures. I can clearly see your fore head concerns. The forehead is short in vertical skin length and lacks bony projection. Probably the shortness of the forehead skin contributes more to the appearance of the small forehead Dan does the lack of bony projection but the two are linked particularly in terms of the approach to correct.
As you may know there are soft tissue procedures to shorten the vertical length of the forehead but there are none to vertically lengthen it. To gain any vertical length you must increase the bony projection/shape of the forehead which can only be done buy a custom for head/skull implant. Obviously the more you do so the more the skin stretches and creates a larger appearance of the forehead. But there is a delicate balance between too much implant projection and creating an unusual appearance. However the tightness of the forehead and scalp skin is going to limit how much for head augmentation can be achieved so this is probably not a significant concern. To evaluate what I think is realistically possible attached I have done some imaging looking at one amount of forehead augmentation to see what the effect is on the size of the forehead and the location of the frontal hairline.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had lip widening surgery done in turkey last November. I had my bottom lip made bigger and the corners of my top lip made bigger but not the vermilion so it looks a bit weird when I smile. My main concern is the corners of my mouth when I open my mouth wide. The scar tissue stops me from opening it properly and it looks weird so want to widen my mouth a bit I want to vermilion lip lift so my top lip is higher than the sides.
A:This is not a lip problem that I have great confidence I can provide the improvements you are seeking. Once you get scar issue near the mouth corners you have as good a chance of making it worse as you do in making it better.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a chin implant done four years ago. My lower lip has never regained full sense (feels like it was numbed at the dentist) and apparently the implant was just some sort of “stock” implant and not crafted to my jawline so I have to have filler put in on both sides of the implant to keep it from having a severe divot in each side. Wondering if it can be removed and replaced with a properly fitted one. I assume the nerve damage is more than likely permanent, unfortunately, but if not that would be fantastic news as well.
A:Thank you for your inquiry and detailing your chin implant surgical history. I obviously cannot speak to the style size or location of your existing chin implant on the bone. Although t is a fair statement to say that a custom implant design would better address placement and location of an implant on the bone and would blend better into it. It may also be possible that your mental nerve damage is due to the location of one of the wings of the implant right next to the nerve causing compression. By removing the implant this may help some of the numbness improve although that should’ve been done long ago for that to provide a good chance of nerve recovery. But in rare cases I have seen patient’s numbness improve in similar situations at postoperative time periods when you would think it would be very unlikely to occur.
The first place to start is to get a 3-D CT scan of your chin/lower face to evaluate your chin implant’s size style and location on the bone. This will provide significant insights into how to proceed forward.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, As U can see in the picture My lower face is very wide , I have had buccal fat removal and liposuction , after a CT scan, it was revealed that I have big mucosal space and my bone structure and size was normal width but the mucosal space is giving the wide face
I already have buccal fat removal, I just need to reduce the soft tissue of my cheeks.
A:Admittedly I have never heard of a ‘big mucosal space’ nor exactly what that means or how that would even be diagnosed on a CT scan.
That being said I think what you are asking about is a more complete soft tissue cheek reduction procedure. While a buccal lipectomy has benefits it is not a complete cheek reducing procedure and does not address the lower soft tissue components of the cheeks. To complete full soft tissue reduction of the cheeks perioral/lateral facial suction and a buccinator mucosal myectomy is what is needed to maximize whatever thinning of the tissues between the bony cheeks and the jawline can be achieved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
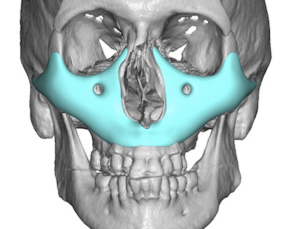 Q: Dr. Eppley, I’m considering getting a midface implant like this one on your website, and I was wondering what is the maximum amount of forward project you do in these cases, particularly in the paranasal region lateral to the nasal cavity since I feel that’s where my bone is most deficient.
Q: Dr. Eppley, I’m considering getting a midface implant like this one on your website, and I was wondering what is the maximum amount of forward project you do in these cases, particularly in the paranasal region lateral to the nasal cavity since I feel that’s where my bone is most deficient.
A:I have seen patients put as 9 mm i the paranasal region but this would be an exceptional amount in the rarest of circumstances. Much more commonly patients have 4 to 6 mm of projection in the nasal base area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am inquiring to see if I would be a candidate for mouth widening surgery as I have a very small mouth.
A:Thank you for your inquiry and sending your picture. Your mouth appears small in width for two reasons; 1) it actually is a bit small in width BUT 2) that is magnified by the complete lack of lateral vermilion height in the upper lip from the cupids bow out to the true mouth corner. As a result the actual mouth with is not truly being shown. The appropriate procedure for improvement is lateral upper vermilion advancements to have they visible lip actually extend out to the mouth corner and smaller lateral Vermilion advancements of the lower level next to the mouth corner so more of its actual with can be seen. This will make the mouth look wider even though actually the math corner has never been moved. This is illustrated in the attached imaging. You cannot do these procedures simultaneously with the true mouth widening as that would create adverse scarring around the mouth corners. But I think this provides a significant improvement that True mouth widening is not really needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to have chin implant removed that was placed submental 25 years ago (XL silicone) I know from reading your blog (most informative that I have seen) that there is no way to know the outcome of removal.The most important aspect of removal to me are function and motor skills opposed to cosmetic due to a family situation. I have more of a general question with the understanding that it would be more guesswork. My question is if I’m correct that mentalis reattachment stemming from the intraoral approach is the primary driver of lower lip incompetence in your opinion? I.e., with the submental approach for emoval,, it is more soft tissue and ligament stretch that may cause chin pad sagging causing a cosmetic deformity but if the mentalis is preserved there is a better chance of not having an effect on speech and motor ability? Thanks for the assistance you provide on the blog it is very informative & helpful – would certainly like to utilize you for this procedure as I think your credentials and experience are unmatched.
A:When considering the removal Chin implant that is associated with lower lip incompetence be aware that new matter how it is removed, intraoral versus submental, the lower lip incompetence is likely to get worse. This would be particularly relevant when one has an extra large chin implant. While you can go intraorally and remove it and do mentalis resuspension, the likely outcome would be no improvement in the lower lip incompetence at best and some increase in it at worst. Mentalis resuspension is not a predictable procedure but it works best when it is supplemented by some form of chin augmentation. But when structural chin support is being removed, AKA Chin implant removal, the operation is very likely to not be successful at all.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m hoping to get saddled infraorbital malar implants that fits my natural profile harmoniously giving me a fiercer look also maybe some zygo projection as well as long as it doesn’t make me look bloated.
A: For successful infraorbital-malar augmentation filler or fat injections are poor choices to do so. Effective skeletal augmentations require more stout and preformed materials.
Also I’d like to know if I actually need the implants or if my desired result is achievable through just under eye fat grafting and some fillers here and there
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am experiencing an issue with the shape of my skull, specifically a noticeable protrusion at the top of my head (the crown area). This bump is quite visible even when covered by hair, and it has been causing me significant psychological discomfort and a lack of confidence.
I have attached a photo to better illustrate my condition.
I would like to know:
Is this bump considered a normal variation, or is it a skull deformity?
Is it possible to surgically reduce or correct this protrusion for cosmetic purposes?
What type of procedure would be suitable for my case? And is it safe?
A: That is a classic sagittal crest head shape but the reality is that it is a pseudo sagittal crest, meaning it appears to be a high crest but it is the parasagittal areas at the sides that are deficient. These side deficiencies make the normal height of the sagittal crest appear too high.
That being said what technique you use for improvement depends on your goals. If you just need a few millimeters removed from the crest for a minimal reduction then you doing a crest burring reduction. But if a significant change is needed in the top of the head shape than parasagittal skull augmentations are needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, With hardware removal, will the chin-bone remain in the same Location? In other words, would the chin implant purely add additional Volume to my X-ray? Or would there be some give and take?
A: The chin bone is well healed at this point and the hardware now is not needed. Meaning the chin bone is not going to relapse any amount if it is removed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, At what age can the procedure for plagiocephaly be performed on a child? Would this permanently resolve the issue and grow with them or would they need more surgeries as they age? What does the recovery from this procedure look like?
A: Skull implants for aesthetic augmentation is not recommended in young patients that still have a lot of skull growth to undergo. For this reason such implants are not done until 18 years of age.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had surgery last year which included a brow lift and midfacelift, as well as shaving of the orbital rim. While I’m very happy with most of the results, I wanted to inquire about an implant to restore the orbital rim to my prior shape.
I feel the doctor shaved off too much and it gave me a very unnatural appearance. The eye is no longer framed by the bone and looks too lifted.
I tried facial filler to replace the volume, and was successfully able to restore it to its prior appearance. But I wanted to look into more permanent options, and can dissolve the facial filler prior to surgery.
I did speak with the previous doctor about my revision options, and his recommendation was a fat Transfer. However, I am apprehensive about this option because I’ve read that the results do not always heal evenly and I’d rather have something that will not change overtime with a density closer to bone.
Does the doctor offer any 3D imaging in which we can get an idea of the outcome of the custom implant?
A: Thank you for your inquiry, sending your facial pictures as well as detailing your surgical history and postoperative efforts. While I don’t know exactly the orbit rim area that was reduced. I am going to assume it was the lateral orbital rim based upon your circled areas. I could easily imagine that with a lateral orbital rim reduction, and then the lifting of the mid face tissues further up onto the cheekbone, this would create a lateral rim deficiency or indent. The lift magnifies the lateral orbitakl rim reduction not helps it.
Based on your successful improvement with injectable filler treatments of the indented area, a more permanent volume addition should be successful. The question then becomes how to augment that area. While it is always hard to argue with making a custom implant design, the lateral orbital rim is not a dimensionally complex area and very likely the reduction was no more than 2 to 3 mm in depth. On a 3-D CT scan the area of orbital rim reduction could likely be visualized by its altered appearance.
That being said, there are two approaches to treating your lateral orbital rim deficiency. Go the ideal route of making a custom lateral orbital rim implant or use an older, but sometimes very effective historic approach of hand making an implant designj during surgery. A 2mm sheet or block of ePTFE is hand fashioned in surgery to the rim defect and secured like a custom implant design with a small micro screw.
Normally, I wouldn’t recommend the more historic custom implant design approach, but the simplicity of the orbital rim anatomy can make that a very viable option. Quite frankly, the decision between the two is primarily an economic one… meaning true custom implants cost more but they do provide the patient with preoperative knowledge of the defect and the exact implant design to treat it.
One caveat about custom implant designs that I would mention based on a comment/question you made in your inquiry is that you cannot design an implant and then paint the patient’s soft tissue back over it to see what it looks like. That technology in any accurate way does not yet exist. Custom implant designs remain an approximation or a guess as to what is going to best address the patient’s problem. In your case, that is a lot easier than most because the defect is small and likely can be well visiualized in a 3D scan. What you really wanting to do is to fill a bone defect rather than creating a true augmentation on a normal bone. Returning a bone to a normal shape is a lot more predictable than changing the shape of a normal bone to a supernormal one in terms of outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I have a protruding forehead (frontal bossing). I would like to know if you treat this in adults
A: Thank you for sending your pictures. The key question on forehead reductions is how thick is the bone and how much of iot can be safely removed. It is also evident in the pictures that you have had prior craniofacial surgery. What is needed is a 2D or 3D CT scan in which the the thickness of the frontal bone can be measured.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I have pectus excvactum and was looking to get a consultation regarding an implant. I have also attached a picture.
A: Thank you for your inquiry and sending your picture. This is a classic case of a moderate pectus excavatum involving the lower end of the sternum. This is treated by a custom implant design, which could be based on external measurements, a three D CT scan, or using implant designs from previous patients with a similar problem. Such a sternal implant is implanted through a small 2 cm incision at the bottom end of the sternal valley.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to make enquiries about skull reduction or occipital reconstruction cause I’m interested in it.
A: Thank you for your inquiry and sending your picture. In skull reduction surgery the most common request is for the back of the head reduction. The success of back of the head skull reduction is based on the thickness of the bone and how much reduction the patient can be expected to achieve. The only way to know this accurately is to get a 3-D CT scan and measure the thickness of the bone. Then we will know how much reduction can be achieved by removal of the outer cortical layer of the skull bone, which is safe to remove.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 30 year old trans woman at 5’9” and 142 pounds. I am going to get my ribs done (broken in rather than removed), but I’m also interested in learning more about the iliac crest implant surgery that you perform. I’ve attached a photo for you to review. Do you think I’d be a good candidate for the procedure?
A: Thank you for sending your pictures. Your narrow pelvic bone and straight frontal profile from the abdomen to the hips is exactly what the pelvic plasty procedure is designed to treat. I widening the iliac crest with a titanium implant, and, adding a silicone implant attached to it to build out the sub iliac Hollow. This is the only way to create some curves in the mid to lower torso area. While rib modifications may have some modest effect it is the pelvic widening whose impact will be more significant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a patient who had chin surgery and had a problem with her lip not closing properly. She is interested in going to the USA for further treatment.
She would like more information to help her make a decision, for example:
- Can this condition be cured?
- How confident in your ability to treat this condition?
- Estimated cost?
- When is the earliest time of appointment for surgery?
This email has attached patient information without identifiable personal information for your consideration.
A: Thank you for your inquiry and sending all of the patients information which is very comprehensive and complete. Given the patient’s prior reductive chin surgery it is not surprising that lower lip incompetence has occurred. This is a very common history for it. Between scarring mand the loss of bony support. The treatment for lower lip incompetence is challenging. In terms of obtaining consistent, successful results. This is particularly so when the size of the chin bone has been reduced.
In answer to your specific questions;
1) The chance of complete cure of lower lip and competence is not high. It is best to view the outcome as improvement. A complete restoration of the lower lip position as to what it was prior to any chin surgery is unlikely. Early surgical results are always favorable. But long-term results at 3 to 4 months out is the real outcome of the surgery and it rarely is as good as it looks in the first few weeks after the procedure.
2) As a result my confidence in a highly successful outcome is low.
I make these comments based on an extensive experience with this problem and the surgery to treat it. I would not want any patient as to the outcome. Some patients do have very good results while others do not. It remains a bit of a paradox to preoperatively determine whom those more favorable patients might be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to know if it is possible to reduce the height of the head by reducing the size of the forehead bone, as well as reducing the size of the sides. I would also like to know if it is possible to change the general shape of the head and restore those areas that need it.
A: Thank you for your inquiry and sending your pictures. In answer to your questions:
1) The most important area of skull reduction would be its height or what you have called the height of the frontal bone. The question is not whether it can be reduced but will the thickness of the bone allow for a visible height reduction. Only a 3D CT skull scan can answer that question accurately. We would need to measure on that scan the thickness of the bone and see how much can be safely removed. There is the issue of whether a scalp incision and resulting scar across the top of your head would be a worthy trade-off if improvement could be adequate. But that question is secondary to will the bone thickness allow for it.
2) The sides of the head are an easier decision to make as the temporal muscle will almost always allow for the convex side of the head to be made straight. But that is a question that can be confirmed by the 3D CT scan.
These two head shape issues are intertwined as if you reduce the sides of the head without making any changes to its height it will look even taller. So the determining issue is the viability of the height of the head reduction.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Can you also ask the doctor that since cheekbone reduction involves the use of pins/screws and plates to secure the cheekbone, can these get knocked loose if there was blunt force facial trauma?
A: Hardware loosening in cheekbone reduction osyteotomies is generally a risk that would most likely occur if substantial facial trauma was sustained in the early healing phase. Once the bones are healed, hardware would be very unlikely to become dislodged by trauma.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I came across your articles last night and was stunned at the depth of your knowledge and expertise. I look forward to being in contact! Procedures/areas of interest (individualized pricing/imaging for each as well as combined would be greatly appreciated but I understand if that is asking for too much): Lip reduction/augmentation – Desired result: more balanced lip size, more defined shape at neutral facial expression Brow bone augmentation/Lateral canthoplasty – Desired result: Hunter eye look you describe. More masculine and appealing upper third/eye area. Custom infraorbital-malar implant – Desired result: higher cheekbones, more definition and masculine look. Custom mandibular implant – Desired result: Emphasis on chin augmentation, adding squared shape and projection both downwards and from the side profile. Widen jaw angle. Not opposed to the idea of buccal area work or chin/jaw/neck lipo if you feel it would enhance/more efficiently achieve the desired results. Thank you so much!
A: Thank you for your inquiry and detailing your numerous facial enhancements. That is a long list of options and the prudent way to approach it is to first create a priority list of the most important to least important and then pass that along to me with some facial pictures (front, side and ¾ views) so I can do some imaging a potential changes in these areas. The priority list will also allow us to answer your cost questions, and based on assessment of your pictures, I would have a better idea as to exactly what the details of those procedures would be.
When, considering a potential facial reshaping makeover establishing the patient’s priorities is the first productive step.
Dr Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m wondering what skull reshaping options there are for plagiocephaly. I would be interested in augmenting the back right side of my head, slight augmentation on the top left side, as well as bridging what I would describe as a divot/dent at the top just above the forehead, as well as reducing the top right forehead and right side a bit due to being pushed forward. I would be interested in the best implant options for the augmentations, as well as the feasiblility of bone burring etc for the reduction.
A:Thank you for your inquiry. All of your skull shape concerns that you have described are common in plagiocephaly. As you have mentioned in your inquiry the two deficient areas can be successfully augmented by custom skull implants based on your 3-D CT scan. The more protrusive right forehead can also be reduced by bone burning. How much reduction needs to be done and can be successfully completed would be determined by measurements on your 3-D CT scan.
The question is not whether all of these skull areas can be treated with overall improvements. The two pertinent questions are how much effort do you want to put into it (cost) and how much scalp scar burden can you tolerate to do so. These two questions are the defining parameters for your consideration in the treatment of your plagiocephaly. The latter question requires a virtual consultation to clarify. The first question will be outlined by be addressed. A very helpful thing to do when one has a multi-area skull shape concerns is to establish a list of priorities from the most important to the least important. As I have just mentioned the question is never whether you can do all of them but what is the effort versus reward ratio.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Dr. Eppley, Do most cheekbone reductions result in a bony union? Are there some that result in a fibrous union?
A:With plate and screw fixation there is a high probability of bony union. Without it a fibrous union will usually result. Whether it really matters that a bony union results in a midface bone which is a non-moving structure and has no masticatory function can be debated.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my eyes are pretty far apart and my bizygomatic width is narrow-average. This throws off my face a ton. Is there any way to widen the cheekbones with implants? If yes, how much mm width could you possibly get?
A: Increasing bi-zygomatic with is done by zygomatic arch augmentation using custom made implants. The amount that the zygomatic arch can be augmented is essentially unlimited as defined by the size of an implant that can be placed and what almost any patient would need. I have augmented the zygomatic arch in some patients by as much as 1 cm per side which would likely be way beyond what is your aesthetic needs would be. Most patients likely would only need 3 to 5 mm per side to achieve their facial widening objectives.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Injectable filler found during chin implant surgery can be removed, and will not sit on top of the augmented chin and cause overprojection?
A:Filler that presents itself in surgery would be removed because it is visualized. Any non-visualized filler would remain and would need to eventually dissipate by the normal resorption process which is highly accelerated by the trauma of surgery in the overall inflammatory healing response.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a buccal fat removal with liposuction almost 5 months ago and I ended up like this. I need to know how this can be fixed.
A: Submalar hollowing caused by buccal at removal is treated by a fat injection approach in the majority of patients. This offers the least invasive approach with the understanding that the survival of fat injections is not completely predictable. The other alternative is the intraoral placement of a dermal – fat graft put back directly into the buccal space. This is the least common approach as it is more invasive than requires and excisional harvest site. That is a more viable option in your case them and many other patients by an intraoral cheek procedure that you would be doing anyway. I am not saying that this is the ideal procedure in your case, just that in doing cheekbone reduction osteotomies the buccal space could be conveniently visualized.
Dr. Barry Eppley
World-Renowned Plastic Surgeon