Your Questions
Your Questions
Q: Dr. Eppley For webbed neck correction apart from the aesthetic aspect, I wonder if I would be more flexible in terms of mobility? Also, is such an operation performed under general anesthesia or twilight sleep?How long does it take to fully recover and when would I be allowed to do sports again? What are the risks of the operation?
A:First and foremost the purpose of the imaging is to show that normalization of the neck shape can never be achieved completely…improvement is seen but the webs are never completely eliminated. If one sees the imaging as not enough change then the surgery is not for them. Imaging is, in essence, a patient qualifier for the surgery. Secondly it is not a surgery for functional range of motion improvement. No such improvement will occur nor is there any surgery that can have that effect. Thirdly, this is an operation done in the prone position under general anesthesia. Fourth one may return unrestricted sports activities 4 to 6 weeks after the surgery. Lastly the risks of the surgery are aesthetic…how much improvement is seen and how well does the scar heal on the back of the neck.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,So I have a drawing here of pretty much what I want for my custom testicle implants. I also included a picture of what I look like on a normal day as well as me stretching my sack with a saline infusion to show that I think I can handle a larger size implant. My goal is to have permanent low hangers that hide my real testicles, but I still want everything to look realistic. just a tad larger than most guys. I have been doing saline infusions for a few years now and I think I decently stretched my skin to make extra room in there.
A:Thanks for the information. The question is certainly not whether your scrotum can handle just about any size implant but what the implant’s size and shape should be. The conundrum is having implants that hang long enough but in so doing also hide your natural testicles. This is where the stretchy scrotum works against what you are trying to achieve based on your drawing. If the implants had that size and hung that low your natural testicles would certainly be exposed. The ‘problem’ with a lot of scrotal laxity is that it would take an enormous sized implants to fill it out without exposing your natural testicles but then they wouldn’t hang like you have drawn. So I don’t think you can achieve exactly what you want based on this drawing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a very important question for you. I have a flat forehead, but slightly sloped, and my brow ridges are underdeveloped, can you augment my brow ridges, and with implants, make my forehead more sloped? Is this possible? On the first photo, the person has a sloping forehead and well-developed brow ridges, while on the second photo, it’s the opposite.
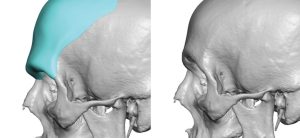 A:You are referring to the use of a custom forehead-brow bone implant surgery for that aesthetic effect, a procedure that I do regularly.
A:You are referring to the use of a custom forehead-brow bone implant surgery for that aesthetic effect, a procedure that I do regularly.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question regarding your testicular enhancement methods with solid implants to see whether it makes sense to schedule a virtual appointment.
My testicles are not small but rather regular (almost 5cm in length) and I would have normally opted for the wraaparound technique to have them enhanced. From one of your recent articles I understand that the wraparound technique not used anymore so the side by side displacement method is the safe alternative nowadays.
And here’s my question: if the custom implant needs to be at least 75% bigger than the natural testicle and if the largest implants so far have been 8.5cm long is this a good technique to enhance ‘standard-size’ testicles where the implants would need to be longer than 8.5cm?
I know that the scrotum can be stretched easily and mine is relatively wide already but what is the limiting factor for these custom implants: is there any technical or medical reason why they can’t be 9cm or 10cm in length?
A: It is not that I would never do a wrap around testicle implant again, and it is a great concept, just that one has to accept the 50% risk that one of them will eventually become dislodged.
At a near 5 cm size you are correct in that volumetric displacement would likely have to be in the 7 to 7.5cm range. Technically it is implant volume not length that matters most when it comes to a displacement effect. (e.g., a 5cm testicle implant = 45cc, a 6.5cm implant = 70cc and an 8.0cm implant = 130cc) As you can see using the length measurement alone is deceiving about the effects of implant displacement on the natural testicles. Then it comes down to whether implants of that size will fit which can be deceiving as there are two of them. But at 7.0cm (80ccs) and 7.5cm (105ccs) probably they would as long as one as some scrotal skin laxity.
I thin now you can also see why implants of 9 or 10cms in size would never be needed nor would they ever fit.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Here are the attached before, after, and hip implant outline pictures. To reiterate, I feel the hip implants designed help address the goals mentioned but might fall short of making this desired silhouette change. To outline the goals in order of importance to least important:
1) To look as natural as possible if not seamlessly natural with the rest of the body.
2) To feminize the hip and side-butt area.
3) To augment the hip (and body) silhouette to get as close to or emulate that supplied after changes picture.
4) To fill in the congenital dip that is currently present on the side-butt hip area to look more if not seamless with the rest of that area in terms of volume.
I also wanted to know what, to the best of their knowledge, would be the trade-off between the scars produced for the current planned implant vs anything larger.
A:Your hip augmentation goals and objectives are not in question. What is in question and is the fundamental dilemma that you face is the following:
To review the fundamental issue with hip implants and their high and predictable postoperative problems that they cause, it comes down to this general premise:
Accept a smaller implant size/coverage with a reduced risk of problems…or go for a bigger coverage area and accept the assured equalae that comes with it.
The key question of course is what is the adverse sequelae that will happen with larger surface area hip implants…the bottom third will bend and the inferior edge of the implant will show,. That will occur with a 100% predictability based on the coverage area you have outlined. The question thus is not whether it will happen but how significant will that effect be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello i want to ask i have 25yo and i see on my skull asymetry. one side is more flat than other side soo if its possible to make more symetrie skull thx!:)
A: All skull asymmetries can be improved using a 3D CT scan to accurately identify the flat asymmetric area from which a custom skull implant is designed to treat it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I was wondering if I could get a consultation from you re a recent sliding genioplasty I just had. I did a google search after the surgery and saw your comments about lip droop. I measured my facial dimensions and it appears my chin was shortened by about 10 mm after surgery and my upper lip about 2 mm. I drool most of the time and can’t say certain consonants like B, F and P. It’s only been three weeks, but your comments have me concerned that this won’t be self-correcting. I was curious if there was any chance of correcting the lower lip with a second surgery.
Thanks for your time
A: I normally don’t comment on patient’s concerns/problems when they are in the early recovery period and are under the active care of the surgeon who performed it. But what I would say in your cases you need ask your surgeon about this early outcome as a lower lip that significantly droops down after chin surgery has a high chance to be a persistent problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Are the titanium hip implants hard when someone touches you? Can I see some before & after pictures please?
A: They are metal so they are hard to the touch, just like your natural iliac crest bone. We are just starting implantation of these implants here in the U.S. so we don’t have any results yet to show. To see results go to the Korean site where they were developed and have been implanting them for several years.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would hydroxypatite implants be an option for skull implants?
A: Unless it is a very small area that is located on the bony skull (not the sides) in which a long scalp scar can be used to access it….no. While hydroxyapatite is biologically appealing it is a poor aesthetic augmentation material whether it is the face or the skull. It simply doesn’t have the proper handling and shape characteristics to effectively use.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, hello I have ptosis of the chin. A surgeon put sutures for an elevation of the vestibule, no anchorage, and it did not work.I know that now you make facial implants but how to fix this please? what technique? help me
A: Ptosis of the chin can be very difficult to significantly improve. Vestibular shortening is an adjunctive procedure in the treatment of chin ptosis not a primary one so it alone would not be expected to work. A small implant that allows for tissue ingriowth, anchorage and vestibular shortening is a more comprehensive approach.
An important question is what is the cause of your chin ptosis?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Could he also do a midface lift from inside the mouth incision to combat any sagging from removal.
A: A midface lift requires a superior point of pull, thus an inferior intraoral approach will not work. But I would doubt that would ever be necessary from nasal base implant removals.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
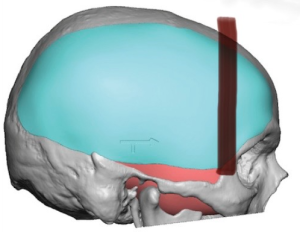
Q: Dr. Eppley, is there a way to make rib removal results more extreme? like removing more ribs?
A: The reason I present the imaging in the way it is shown is because you make a decision for surgery based on the LEAST amount of change that is known to occur NOT on the most amount of change you hope will happen. The former is known to occur while the latter may never happen. It is all about controlling expectations as that is how you don’t end up disappointed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Does The Orientation of the Dermal-Fat Graft Affect How Well It Works In Buccal Lipectomy Reversals?
Q: Dr. Eppley, In your case study titled “Plastic Surgery Case Study – Buccal Lipectomy Reversal with Dermal-Fat Grafts” you write “With the suture placement through the graft the dermis surface of the graft into the pocket on the opposite side of the incisional closure.” I have 2 questions about the Dermal Fat Grafts (DFG) orientation inside the buccal space, as it is described in the above excerpt:
1. Does the Dermis side of the DFG face the cheek/away from the mouth, or does the Dermis side face the tongue/towards the mouth?
2. Does the orientation effect the viability of the graft?
A: In answer to your dermal-fat graft questions:
1) The dermis side faces the incision or the tongue side.
2) In the deep buccal fat pad space the orientation of the graft does not affect its external visibility.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a problem with flat back head and have few question about skull reshaping surgery.
How long does recovery take after surgery?
Can I travel by plain after surgery?
Do the implants need to be replaced or do they last for life?
A:In answer to your flat back of head questions:
1) Custom skull implants are made to treat it (see attached) and such implants are permanent and never need to be replaced due to structural failure.
2) Recovery is largely defined as swelling and sometimes bruising of which the most significant of these effects are largely resolved in 10 to 14 days after the surgery.
3) Patients can return home 2 to 3 days after the surgery including by air travel.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
 Q: Dr. Eppley, This is the kind of head widening implant design I think I’ll need .. I made a line where I think the implant should start or somewhere around there .. my main thing is the thickness I just want to have a normal head shape I would say I want the maximum thickness to give me a normal round head shape.. but I dont know how that works .. I’m just afraid I’ll look the same but I also dont want my head to look weird and big 😩 I just want to look normal without me having to do tricks to my hair/head.
Q: Dr. Eppley, This is the kind of head widening implant design I think I’ll need .. I made a line where I think the implant should start or somewhere around there .. my main thing is the thickness I just want to have a normal head shape I would say I want the maximum thickness to give me a normal round head shape.. but I dont know how that works .. I’m just afraid I’ll look the same but I also dont want my head to look weird and big 😩 I just want to look normal without me having to do tricks to my hair/head.
A: What you are illustrating is the implant’s footprint. (i.e., what should it cover) Once that is established it is about implant thickness (how much/wide) and where should the maximum projection be located. (usually that is more central above the ear) In such head widening implants the risk is always being too bit as opposed to not seeing a difference. (which has never happened) As a general rule 5 to 7 mm max thickness is the normal range for most patients.
That being said the most important step before any implant design is to determine what type of change the patient is seeking. The concept of a normal head shape is open to individual interpretation.To do so imaging needs to be done on the paient’s picture to determine what is too little and too much from which the implant design is determined. (aka I need a front view picture that shows the sides of your head)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I ask about options in orbital box osteotomies that don’t expose the brain? I dug up two examples I found online:
1. Here’s a variation of the box osteotomy that tries to avoid the brain by cutting into the sinus instead:
2) Here’s an implants-focused approach with minimal/no osteotomies?
It seems like this approach accomplishes many things at once that I’d like: increase in distance between the pupils and between the canthals, as well as widening the temples to fit the change.
Of course, I’d like to take a feminizing approach to the implants, which merits more nuance than adding more bony volume.
Would you be open to discussing either option? If so, I’d love to hear your thoughts!
A: When it comes to the Trsnscranial and Transinus Orbital Box Osteotomies the operative phrase is ‘trying to avoid’ entering the cranial cavity’ does not eliminate the risk that it may happen and all the sequalae from it…still an ll-advised procedure in my opinion that does not justify the effort and risks for the aesthetic gain desired.
This is what happens when the patient aesthetic goals are a ‘tweener’, meaning the goal is too small for the big operation but just beyond what the smaller operation can do.
The implant approach to hypoteloric issues takes a 180 degree change in treatment direction. Here the question is not one of safety or magnitude of the surgery but one of will it be effective to achieve the goal. There is no doubt that periorbital implants can be designed and placed to change the shape/position of the orbital box…that is done not infrequently for horizontal rim augmentations. The critical question is whether doing so for a change in orbital box width (with a different implant design) will make the eyes appear to have an increased interpupillary distance. In theory it has the same effect as the orbital box osteotomy without cutting the bone as osteotomies do not really move the eyeball laterally unless they are a true 360 degree transcranial box osteotomy.
I would be cautious about interpreting the computer simulations you have attached as those are theoretical implant designs and the before and after result shown is simulated (with the eyes closed)….so we don’t really know what would happen on an actual patient. I think it would clearly make the orbital width wider, I just don’t know how that would affect the appearance of the interpupillary distance.
I can, however, borrow from my own clinical experience with perirorbital implants done for a slightly different purpose…to make the orbital width wider for a narrow forehead/temple/lateral orbital width. In looking at a few patients with matched before and afters there may be an increased interpupillary distance.(see attached)
It is an interesting concept because of its lower risk and for less severe hypotelorism cases. (wouldn’t work for more significance case) I can envision a periorbital implant design that has some potential for that effect. This largely adds width and little increased horizontal projection. Its design is very similar to the transcoronal 270 degree orbital box osteotomy.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Im interested in hip/buttock implants and would like more informations.
A: The first clarification is that I only do implants for buttock and hip augmentation and not fat transfer. (aka BBL surgery)
That being said the first step is to determine what your buttock and hip augmentation goals are and whether they fir into what implants can safely achieve. To make that determination I would need to see current buttock and hip pictures along with some idea of what type of change you are seeking.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Sir, In general of larger sliding genioplasty,how much percent of setback is possible?
The problem is I had underdeveloped jaws ,old surgeon didn’t inform me about that and did did a maximum vertical and horizontal advancement, so my mouth is near to nose (it’s in upper position) and my chin is too down , my bone is completely healed, although I had larger advancement ,I need complete setback but it’s not possible.how much setback is possible
How much setback is possible, and how much mm can be reduced in revision genioplasty
A: There is no restriction of how much a sliding genioplasty can be reversed, provided one knows the exact dimensions horizontally and vertically the chin bone was moved. Your surgeon should be able to proivide those millimeter numbers. But if not it can de determined by a lateral cephalometric x-ray.
Be aware that the soft tissue chin pad has been stretched and it will not go completely to its original shape. Thus I would be cautious about a 100% reversal as you may create soft tissue problems that you did not have before.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I was wondering if there was anything that could be done about my forehead. One side is good and the other side bulges out very far. I sent an image to better explain what I mean, the arrow is to the side I am talking about. Please let me know if there is any surgery’s or procedure that could make it symmetrical and the same as the smaller side.
Thanks
A: I believe you are pointing to the anterior temporal region (not the side of the bony forehead) which is made up of muscle and not bone. There is not a good surgery for muscle reduction in that temporal area. Botox injections is used to treat masticatory muscle areas that are not amenable to surgical reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, With the new custom skull implant, will there be a void between the implant and my skull? or will the implant be in full contact with my skull for the entire surface area? The implant is placed directly onto the bone (skull). Understood, however, if the volume is greater than the thickness of the implant, will there be a void between implant and skull? meaning the implant will have a curvature and the skull is flat, there will be void between implant and skull. does that make sense?
A: Silicone skull implants have some flexion so the pressure of the scalp will press it flat against the skull if it does not have a perfect fit.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I would like to schedule a consult, before I do I just have one question. I’m looking to have infra orbital malar implants done. Would this interfere if I decide to have double jaw surgery down the road ?
A: Infraorbital-malar implants are placed well above the level of a LeFort I osteotomy and done through a lower eyelid incision. Thus they can be done before and after double jaw surgery without any issues.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope you might be able to offer an increase in calf size for me.I’ve been working out for 10 plus years and they just don’t grow 😊 😊Therefore, a polite inquiry as to whether it would be possible to get them bigger via calf implants
A: The gastrocnemius muscles can be extremely hard to hypertrophy (grow) due to their tight muscle fibers. Calf implants (2 per each calf, one for each muscle head) would be the only method to make an appreciable size change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve developed pixie ear deformity from a mini lift 3 years ago. I’m 26 years old and don’t have much skin laxity. I’ve done a lot of research into how to fix this, I’m aware some of the options include a revision facelift but also a more direct approach by reducing the ear lobe and the leaving a vertical scar at side of face . Can dr help me?
A: Unfortunately facelifts in young patients often result in adverse scarring and elongated ear lobes. While a revision facelift would be one approach for a pixie ear deformity that is not going to work for you as you have correctly surmised. The pixie ears are too long (severe) and you are too young to have any significant skin laxity. The only effective approach would be to treat it directly with earlobe shortening through an inferior helical rim technique. While effectively shortening the earlobe this will leave a fine line scar in placed of where the lower end of the earlobe now is.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, , I have a very protruding rib cage while at the same time being pretty thin. Can this be reduced by rib removal/shaving safely? Does the rib cartilage regrow? Will there be life long limitations on exercising etc?
A: The question is not whether the prominent subcostal ribs can be safely reduced but whether the scar tradeoff to do is a worthy tradeoff. Unlike lower rib removal where the scars are in a more favorable location subcostal rib removal places the incision in a very visible area right over the subcostal margin. So I would be cautious about that scar location as it is not in a natural relaxed skin tension line and the scar may not do well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi! I had clavicle reduction and waist narrowing with Dr Eppley on March 13, 2023. I am considering having the clavicle hardware removed. I’m interested in learning more about what it would cost, how far out it would have to be scheduled, recovery restrictions, that kind of thing. I am very pleased with the results of both the shoulder narrowing, and the waist narrowing. I healed up very well. However, one of the screws on my right clavicle feels like it has worked its way out by just a few millimeters. It’s not a huge deal, but the surrounding tissue can get a little irritated sometimes, which is why I’m asking about the hardware removal. Thanks!
A: Good to hear from you and I am glad to hear that both procedures were beneficial. Certainly after over one year of healing the clavicle hardware can be removed. The hardware removal is very different and offers a much easier recovery. It is a one hour procedure done as an outpatient. There are no significant restruction of arm movements after surgery other than I would avoid heavy lifting for the first 30 days after as a pure precautionary maneuver. The clavicle osteotomy site is undoubtably healed but whether it can sustain heavy load bearing across the healed osteotomy line which has been protected by the plate and screw fixation is one potential issue to be aware. This it may take some time for the clavicles to re-establish their strength once the fixation has been removed, thus I would simply be mindful of that in the short term.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in getting calf implanst to make my lower legs bigger. Do I need three implants per leg to do so?
A:I am not aware of a 3 implant approach to calf augmentation. There is only one muscle (gastrocnemius) with two heads in the lower legs that can be augmented with implants. (2 per calf muscle) Thus a 4 implant bilateral calf augmentation would be the standard approach which would produce a result similar to the attached imaging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in custom infraorbital-malar implants from Dr. Eppley post-double jaw surgery Ihave scheduled in 8 months. I’m contacting wondering how long I should wait after having the jaw surgery to come in for a consultation with him about the implants? I heard residual swelling can last many months, but wondering if that matters when dealing with planning implants. Curious when he thinks is the best amount of time to wait? Also, i’m just wondering how about how long is the waitlist for the first appointment? So i can kind of know when I should start trying to book! Thank you!
A: Given that the implant design process and getting scheduled for surgery is a minimum of 3 to 4 months it would be good to get started anytime. A 8 months postop there really is no significant residual swelling in the undereye area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Hello, I’ve recently (6 days ago) had several surgeries for my eyes, to make them look more alert. The surgeries were a lateral canthopexy, lower eyelid raising, lower blepharoplasty, brow lowering and fat grafting to the upper and lower eyelids. I now have the issue that I look too changed, mainly from what I suspect to be an overfilling of fat in my upper eyelids area (3ml on each side). My eyes have gone from having moderate upper eyelid exposure to being almost completely hooded.
I was wondering, is a revisional upper blepharoplasty possible to remove some of the excess fat? Or is it that I’m still too swollen and some of the fat will be absorbed anyway? Thank you
A:You judge the final outcome from this surgery at 3 months not 6 days. A lot will change between now and then as the tissues heal.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I had previously made an inquiry about my shoulders a month ago and I’ve come back to make a new inquiry that would really help me if I could get some sort of disclosure on it. I have a square jawline that I’m not happy with and I was wondering what could be done to make my jawline more narrower and even give my chin an outward look instead of being flat from the front and the bottom? (pictures attached below, and I also apologize for the terrible quality once again since they had to be taken on a not so great handheld camera since I don’t have my phone available at the moment). I was also wondering how close, in terms of timeframe could I have my desired shoulder and chin narrowing cosmetic surgeries done? Thanks!
A:What you are referring to is V line surgery (aka jaw reduction surgery) There are two types which I label as Western and Eastern (Asian) methods. The chin part of such V Line surgery would be the same with either style (sliding genioplasty) It is the jaw angle part that will differ radically between the two styles. I have imaged (see attached)m the Western style where the jaw angles are narrowed but largely keeping more of their overall shape. In the Eastern style they are radically amputated which, produces a profound narrowing effect, but removes the entire shape of the jaw angles and often results in some loose sagging skin.
Both shoulder narrowing and jaw reduction surgeries can be performed together or separated by 3 months apart.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to make my waist as small as possible. how many inches are patients typically able to get off?
A:On average patients report 1″ to 3″ waistline reduction but that will vary depending upon their height and body type. What I pay for attention to is the effect rather than a number. (although he two are obviously connected) In that regard I have attached some imaging to show what I believe the effects of rib removal on your waistline.
Dr. Barry Eppley
World-Renowned Plastic Surgeon