Your Questions
Your Questions
Q: Dr. Eppley, I am interested in a wider mouth smile. This is an example in which when the woman smiles, wouldn’t it make sense that her smile would be wider if her mouth was widened ? Because the mouth opening is now wider, which means more teeth would show when she smiles no?
A: Maybe it would but one is smiling against a scar line so it is probably not a 1:1 ratio…meaning the amount of mouth widening at rest may not be the same amount numerically when one is smiling.
Quite frankly it is simply a dynamic assessment of a static operation that I have never assessed before….so I really can’t say for sure what the dynamic effect of mouth widening is.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if there is any possible way to get clavicle shortening done on a 13 year old girl.
A: Patients have to be at least 18 years for shoulder narrowing surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, If one were to do something like full midface implant, would it have a similar effect on the nose as a lefort where the nose becomes wider and upturned?
A:Not necessarily. It would depend on the various thicknesses in the nasal base area. It almost assuredly would not increase nasal tip rotation. But any form of midface soft tissue degloving, even without placing an implant, can widen the nostrils by a few millimeters. But that potential issue is overcome by either intraoral nasal base suturing or external nostril narrowing by sill wedges.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have been looking into paranasal and premaxillary implants trying to determine if they are something I would benefit from in combination with the IOM implants we are doing. With this context
1.) Would I benefit from the augmentation of either premaxillary or paranasal regions – I can send additional photos for analysis if needed
2.) What is the impact on the nose, and the risk of it raising/changing position and could nasal tip projection changes be avoided?
3.) If removed in the future, what sort of sagging would be present (such as would it cause the upper lip to retrude more than pre-placement, cause an elongated philtrum, etc.)
A:In answer to your midface augmentation questions:
1) In looking at your pictures you definitely would not benefit from premaxillary augmentation (central nasal base) as you already have adequate projection and a fairly open nasolabial angle. It is paranasal (side of the nose) augmentation that may be considered.
2) Paranasal augmentation causes no changes in tip projection, it may cause 1 to 2mm of nostril widening.
3) Removal of paranasal implants will not result in any tissue sagging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, So what I was hoping for was a way to widen my smile, I’ve always been told I have a pretty small mouth so perhaps that procedure combined with a v-line jaw procedure would be good?
A:i don’t know of a reliable method to make a dynamic change like widening one’s smile. While mouth widening surgery does exist that achieves its effect in the static non-moving state. That does not mean that it always translates to the dynamic smiling state.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can you correct a botched forehead augmentation that I’ve gotten a few years ago? It looks worse than before I had the procedure and I highly regret it. The middle right side is more protruded than the other side and my overall forehead looks strange in the middle area. I want a smooth symmetrical forehead without dips and concavities which I’ve dealt with since birth. The Dr. augmented my forehead by shaving the bone through 3 scalp incisions. I also got hairline lowering done by this Dr. A few years ago as well and hate that my hairline is crooked and you can still see a visible scar. I should’ve went to a more experienced Dr. and should’ve done more research. I’m hoping you can help me gain my confidence back.
Thanks! Hope to hear from you soon.
A:There is only one method now to make the forehead smooth and even and it would have to be augmentative in nature. The bone is not thick enough in the middle, particularly the lower part over the frontal sinus, to do any more reduction. This could be smoothed using either bone cement through the hairline scar that you already have. While that scar can be cut out and reclosed it will probably not be much better since your natural skin pigmentation is not going to hide a fine white scar line very well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would really like to ask you about surgical techniques for increasing eye distance. As I have read in your answers to similar questions in the past, increasing distance between eyes horizontally is quite challenging, and I understand that the most effective procedure is the orbital box osteotomy. This is however too extreme for me and I believe the change I’m looking for definitely does not justify the procedure. However, I have read a few more recent posts of yours where you describe less comprehensive procedures, such as periorbtial implants and a modified subcranial 180 degree orbital osteotomy. In less medical terms, what do these procedures entail and which, if any, would achieve a 6-8mm increase in interpupillary distance (which is what I would be looking for)? How difficult and predictable are the surgeries? How big are the risks?
 A: Alternatives to a 360 degree orbital box osteotomy is considered in patients who have aesthetic hypotelorism (aka decreased interpupillary distance) in which the need for the increase in interpupillary distance is less thana combined 10mms or 5mms or less on each side) The inferior orbital box osteotomy exists for that purpose which is done through a combined lower eyelid and intraoral approach. The ‘problem’ with this approach is its unpredictability. Will it achieve a 6 to 8mm increase in IPD or will it end up as 4 to 5mms? Impossible to know for sure beforehand.
A: Alternatives to a 360 degree orbital box osteotomy is considered in patients who have aesthetic hypotelorism (aka decreased interpupillary distance) in which the need for the increase in interpupillary distance is less thana combined 10mms or 5mms or less on each side) The inferior orbital box osteotomy exists for that purpose which is done through a combined lower eyelid and intraoral approach. The ‘problem’ with this approach is its unpredictability. Will it achieve a 6 to 8mm increase in IPD or will it end up as 4 to 5mms? Impossible to know for sure beforehand.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, ! love your work. i’ve had a liplift before and i dont love my lips, specifcially the cupids bow area. it feels very “unsupported”. i also wish my bottom lip was bigger downwards, which lip filler doesnt really do.
i was wondering if you have any techniques that could inprove my lips? i was thinking perhaps a lip implant to round out the top? i attached pics of what i have and what i want. thank you!
A: What you seeking is a cupid’s bow reduction or a smooth non-indented area between the two peaks of the cupid’s bow. In essence a smooth vermiliion-cutaneous border across the lip. This can not be achieved by fillers or an implant. There are two techniques to try and achieve that effect. One approach is to excise the skin between the cupid’s bow and advance the vermilion into the excised area. (central vermilion advancement) The other approach is to excise the peaks of the cupid’s bow . The choice between the two depends on how sharpo the cupid’sd bow peaks are, the depth of the skin indentation between the two cupid’s bow peaks and the size of the upper lip. For your upper lip I would recommend tye central excision and vermilion advancement based on your upper lip shape. (see attached) Because of the notch in the smile line of your upper lip a small Internal V-Y will help with the central vermilion advancement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My dream is to have a more V shape body like this, have done some retouch / app on last picture.
A: Based on your pictures you are inquiring about reduction of the wing of the pelvic bone. (aka iliac crest) Iliac crest reduction surgery can be done but is usually performed over the most prominent lateral extension of the bone. Your pictures, however, show the entire prominent iliac crest from anterior superior iliac spine in front to the posterior superior iliac spine in the back due to your lean body frame. Reducing the entire iliac crest s not advised due to the length of the scar and the amount of muscular attachments that would need to be released to do so. middle portion of the crest is usually reduced for these reasons.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 69 year old female who had a chin implant 15 years ago. It was a Large silicone wing implant which has shifted over the years. Never fit properly over my jaw. I have an asymmetrical facial structure. I lost my angular chin. It became rounded.I have a narrow face. I wanted a little more projection from side profile. Was never happy with the results. Presently I am preparing to have a facelift and I am doing research, but I would like the implant to be removed.
I have been on many consults but most doctors do not want to remove the implant and say that it just creates more problems and they won’t touch it. Other doctors will remove it and want to put a smaller one in and then other doctors want to remove the capsule and let it go back to its original state along with doing a facelift. All say I never needed it in the first place.
I am looking for a doctor who can really tell me what’s going on and what I can expect and if I should even remove the implant. I’ve never been happy with it so now that I’m doing a facelift is the time to address it.
A: In a long standing chin implant that is too large removing and not replacing it will result in significant chin ptosis…so that is the worse option. The overlying soft tissues will not go back to what they were. Removing and replacing it with a more appropriately sized/shaped chin implant would be the prudent choice. What that should be depends on what the current implant looks like and how it is positioned on the bone. To avoid guessing a 3D CT scan should be done where everything about your current chin implant will be clear.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have 1500cc silicone breast implants but I would like to switch to 2500cc in overfilled saline solution. Here in Italy they don’t do it because they say that an 800cc prosthesis overfilled to 2500cc would certainly break, then tend to deflate, the valve would have problems. What do you think?
A: Those are legitimate overfilled saline breast implant concerns although I have not seen them. I think an equal if not bigger issue is that with an existing implant capsule from your indwelling silicone implants the capsule is not going to allow for an additional 1000ccs of volume. It may permit 300cc to 500cc ore volume but most certainly not 1000ccs.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a 3mm bump on my saggital crest. I am 20, only just realized. Should I be worried. Many people have skull deformities. Will this have any affects on me it later life? Is this surgery essential or cosmetic. Lots of misinformation. Because looking at skulls this looks normal.
A: It is a cosmetic issue only.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Heya! I wanted to ask something about the shoulder reduction surgery. Are the metal bars that are used to keep the clavicles together following the clavicle shortening permanent, or can they eventually be surgically removed once the bones have healed and no longer need its support (hypothetically speaking). How long would that take to remove them if so?
A: Most clavicle reduction patients do not remove their hardware but those who do does so because they have excessive hardware show. For those who chose to do so it is done one year after the shoulder narrowing surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How does the inferior orbital box osteotomy increase IPD? Is any bone shaven/moved or is it only soft tissue? How would you describe the risks?
A: It works by increasing lateral infraorbital space which shifts the position of the globe.(eye) Risks include lower eyelid scarring, infraorbital nerve numbness and undercorrection.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, just curious if you had testicular enhancement procedures. I am 34 years old and on TRT for the past 3 years and got little nuts now lol.
A: Most testicular enhancement procedures use a side by side by side techniques using custom testicle implants in the 6.0 to 7.0cm size range. While the natural testicles can be removed, the side by side technique keeps them in place and the larger implants displace them from view.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How can I help my head to be smaller?
A: While certain areas of the head/skull can be reduced to change its shape and make it appear a bit slimmer/smaller. How that applies to you I can not say based on your inquiry, this requires a specific description of your head shape concerns along with pictures that so illustrate.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
How Can I Improve The Prominence Infraorbital Rim Appearance After PEEK Infraorbital-Malar Implants?
Q: Dr. Eppley, In January I had double jaw surgery for sleep apnea along with a saddled PEEK implant to the infraorbital zygomatic region. I was wondering if it is possible to resolve my issues with the implant without removing them. While the shape of the implant seems natural enough, in certain lighting the implant shows through the skin and there is a very deep hollow between the undereye and the orbital rim. Does it look possible to smooth out with fat grafts or will I need it removed or replaced?
A: Whlle I haven”t seen your PEEK infraorbital-zygomatic implants design what I can see is that the infraorbital component is prominent which is a design and material issue. But assuming every other aspect of the implant’s effect you like it would make the most send to try and camouflage the issue rather than directly treat it. (total implant replacement) The options for infraorbital camouflage include injectable fat grafting or ePTFE sheet implant overlay.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got newer implants with a breast lift that left me with bad keloid scarring about 2 years ago. I’ve tried topicals but I’m not seeing much of a difference. The scars are worse due to the fact I was allergic to the stitches and it caused sores which took longer to heal. I’m including a pic of the lower part of my breast. I don’t know if these can be removed but I wanted to ask because it has really affected the way I feel about my body in a bad way. Please let me know if you can help. I live in TN and I don’t want to travel for surgery unless you think you can drastically reduce these scars. Thank you
A: With wide hypertrophic scarring topical treatments will not be effective. The only effective treatment is to cut out all of the scars and reclose it to bring ubnscarred skin edges back together. (secondary breast lift) It would be helpful to know how the incisions were initially closed which should be in the original operative note. In addition this also raises the question of what does your original surgeon say about improving the scarring since what I am suggesting is not novel…it is the only path to improvement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How can the scars from may facelift be improved?
A: Thank you for sending your pictures. Your facelift scarring shows multiple issues which includes:
1) hypertrophic anterior scarring
2) trapped right earlobe skin
3) left pixie ear (pulled down scarring
4) bilateral anterior displaced preauricular scars
Like all secondary problems it is helpful to know exactly how the issues occurred so they could be avoided the next time. While you nor I will never know the exact details of your facelift (what was done under the hood so to speak), and I wouldlike to read the operative note from the surgery, I do know the following:
1) To be successful with the anterior (preauricular) scarring the facelift flaps must be re-raised ad the closure line moved back into a retotragal position which is more consistent with a female facelift. This will also hide some of the closure and give the rest of the anterior scarring a chance to heal better.
2) The elongated left earlobe is a form of pixie ear in which the scar pulls down on the earlobe, lengthens it and then shows visible scsarring below the earlobe. This again supports re-raising the facelift flaps.
3) For whatever reason there appears to be trapped earlobe skin/tissue in the closure line, hence the hole.
When you put all this together the only successful strategy is to redo the facelift…this time with deeper tissue support and different scar placement. (retrotragal) Management of facelift scars rarely is as simple as just cutting out the scars and closing. It almost always requires some or all re-elevation of the facelift flaps and a deeper method tio better distribute the forces onj the incisional closure. This becomes paramount because the ‘easy’ tissue laxity has been removed and now the tissues are scarred and less mobile.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello there, so I’m trying to see waistline reduction for a specific measurements, I’ve already removed the 12th, 11th, and the 10th rib previously. Had liposuction and I still have yet to achieve the proper results that I’m looking for. I was wondering what you might suggest.
A: Whether you can ever achieve the waist narrowing results you are striving for is up for debate. But what is clear is that the last anatomic barrier to what is possible is skin. The rolls of skin on your back indicate significant laxity for which a vertical backlift can have a definitive torso narrowing effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, can you please let me know the cost of brow bone implant? I’m trying to figure out whether it’s more cost effective to have done in the States or in Thailand. Thanks
A:In reply to your inquiry I can make the following comments:
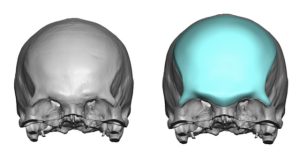
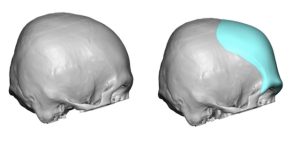 1) You can not just have a brow bone implant alone as your forehead is significantly recessed as that will make it look unusual. You need a combined forehead-brow bone implant to bring the entire upper third of your face foreward. (see attached imaging as well as implant design)
1) You can not just have a brow bone implant alone as your forehead is significantly recessed as that will make it look unusual. You need a combined forehead-brow bone implant to bring the entire upper third of your face foreward. (see attached imaging as well as implant design)
2) The augmentation would have to extend down into the nasal radix area to avoid the nasofrontal angle from becoming too deep.
3) The question is never whether it will cost less in Thailand…as that will always be true. The real question is what will be the result differences.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can’t figure out what’s going on, I think somehow my maxilla is too small or something.
A:You have two fundamentally different paths to go down:
1) Treat the underlying maxillomandibular deficiency with Bimax advancements (upper and lower jaw advancement surgery – see attached imaging)
2) Leave the maxilla and mandible (jaw bones) where they are and do a camouflage approach with either either chin augmentation alone (implant vs sliding genioplasty) or total jaw augmentation with a custom implant. (perhaps even with a rhinoplasty to help de-rotate the tip of the nose) (see attached imaging)
There is no right or wrong here. It is all about what final aesthetic result do you want and how effort do you want to put in to achieve it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’d be interested to know the approximate price of standard infraorbital rim implants and the price of custom ones as well. The lid retraction is genetic I’ve never had any surgery near my eyes. My goal would be to get rid of my sceleral show, improve my negative orbital vector and get rid of the darkness under my eyes.
A: It is important to be aware that standard infraorbital and custom Infraorbital implants do not have the exact dimensional effects. (customs saddle the rims while standard implants do not which will affect how they treat a specific problem particular in congenital scleral show)
While implants have a role to play in the treatment of scleral show and eye corner reshaping they must be combined with lateral canthoplasties and spacer grafts for the lower eyelids to be maximally effective. Natural scleral show is a reflection of underlying tissue deficiencies which includes bone and soft tissues. Unless all are addressed either a failed or inadequate result will occur. As a result you can see why the combination of implants (bone augmentation), spacer grafts (lower eyelid vertical tissue addition) and lateral canthoplasties (coner repositioning) is ideally needed.
Thus you have to look at implants as part of the solution but not the total solution.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, when I had the genioplasty in SK, there is a noticeable dent on the edge of my jaw that creates the look of a ‘jowl’. One side of my face is much more shaved down than the other, making it appear full, the same side with the genioplasty dent, and it makes me very insecure still.
I would also like a little bit of extra jaw angle on the side that is still a greater size, to create a more pointed edge, as well as more chin projection horizontally, and probably nothing vertically. Although, the length of my face may be an illusion due to how narrow it is with the lack of a proper jaw angle. I was also wondering if I could get paranasal implants for my nasolabial folds. I realize this is a lot of different procedures, but I know you are the best when it comes to implants, and after seeing how much difference the cheek implants have made in my face, you would be able to help me. Thank you so much
A: It is easy to see in your postop x-ray the very significant left jawline/chin deficiency which is present to which a custom jawline implant is the only effective method to improve it. That can certainly be combined with a right jaw angle implant to achieve your desired effects. Getting both sides of the jawline augmented and even/symmetric is the exact role that the custom implant design process is suited to do.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
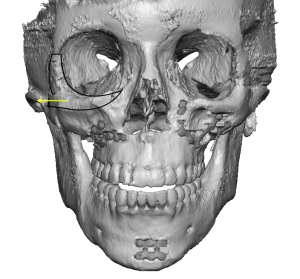
Q: Dr. Eppley, I would like to get an aesthetic metopic ridge reduction surgery. 39M.Can I have more details about the procedure, like cost, what to expect, etc? I think I was born with a minor form of trigocephaly (metopic craniosystosis).
A:I believe your supposition is correct in that your midline ridge is a microform of metopic synostosis…as that would be the only explanation for why it is there. Burring reduction would be an appropriate treatment for it provided the bone is thick enough to do so. Usually it is since in synostoses the suture line is thickened not thinner. But it is always a good idea to check a 2D scan to know for sure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I had a facelift over a year ago with a neck lift. I have been getting injections on my scars but they still haven’t helped. Is there anyway I can get some information on possibly getting treated?
A:These are significant hypertrophic scars for which injections are not going to be effective. The only effective approach is to cut out the scars, re-elevate the facelift skin flaps, and do an extended SMAS or deep plane lift/support. This is the way you keep all the tension off the closure line and then they will heal without the hypertrophy and pixie ear deformities that you have. There is no ‘little’ way to fix this problem. While the injections have not been harmful they are just buying time to get to what really needs to be done and at one year postop that can now been done at any time.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would like to have a slimmer non round shaped face? What is your recommendation and costs associated. would like a flatter chest, smaller muscle and shoulder blades that don’t stick out so much.
Head Width Reduction
Temple Reduction/Bone Reduction
Check bone Reduction
V-shaped Jaw Surgery
Chin Implant
Shoulder Blade Reduction
Chest Reduction
Trapezius Reduction
A: This is a long list of desired procedures for which I can summarize my opinions as follows:
1) Unless one is having clavicle shortening (shoulder narrowing) there is little sense to scapular and trapezius reductions. So I would eliminate the body procedures minus the chest reduction which is really chest liposuction/areolar gynecomastia reduction.
2) The lowest hanging fruit on the face, so to speak, is the chin augmentation. This is at least 10 to 12mms of advancement for which a sliding genioplasty is the appropriate procedure. (see attached) This forward movement will also make the jaw more narrow in appearance so this is your V line procedure not the whole jawline. (see attached imaging)
3) You have a wide face which starts at the skull and goes down through the cheeks but, as part of that development, your eyes are also widely spaced. (type 1 hypertelorism) As a result you don’t want to try and narrow your face aggressively as that will just make the eyes look even wider apart. I think the skull/temporal reduction is beneficial but I would leave the cheeks alone. (see attached imaging)
In conclusion, a sliding genioplasty with type 4 temporal reductions and possibly chest liposuction is what I would recommend.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in getting some custom cheek implants. I wondered if you could send through some before and after pictures of males with implants that add Malar projection with the sizes? I believe I’m looking at 5mm of projection.
A:Due to patient confidentiality I don’t pass out patient pictures. (I suspect you would not want your pictures passed around randomly either) But that issue aside other people’s results and implant dimensions have little actual correlation to someone else based on anatomy and aesthetic preferences. What matters is what is the patient’s specific cheek augmentation preference/target is? That can only be determined by computer imaging of the patient’s pictures to determine their range of change tolerance. I don’t how you have picked the 5mm thickness number. Buit unless one has gone through the imaging exercise to develop a feel for the change the patient is seeking there is no way to know the relevance of any specific implant dimension.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Would a genioplasty/sliding genioplasty have different look affect or roughly the same?
A:If you are referring to how it looks horizontally or in the side view an implant and sliding genioplasty will look the same as long as they are in the under 10mm movement range. It is in the front view where they may look potentially different as a chin implant can make the chin wider or more square if desired while a sliding genioplasty can not.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing this email to share my concerns about a craniofacial asymmetry that has been bothering me. I was born as a preterm baby and I was hospitalised for over two months due to low birth weight and complications from hydrocephaly. Since my childhood, I have been extremely conscious about my prominent ears. I also had dental malocclusion, which bothered me as I believed that it contributed to my lopsided smile but otherwise, there were no complications in speech or eating. In 2011, I underwent orthodontic treatment and in 2013, I had otoplasty to correct my prominent ears. While the otoplasty dramatically improved my appearance, I noticed that my left ear was slanted at an angle “\” while my right ear seemed perfect. I underwent two revision otoplasty till 2014 to unsuccessfully resolve this issue. I then decided to let the matter rest.
My first orthodontic treatment concluded in 2014, by my lopsided smile remained and I am still undergoing orthodontic treatment to this date to correct a mild occlusal cant. I have had consultations with oral and maxillofacial surgeons in 2016 and they ruled out jaw asymmetry.
I have spent the past decade trying to understand the factors contributing to my facial asymmetry. The issue that bugs me the most to date is my lopsided left ear.
I used to go to a hairdresser regularly, who pointed out that my head is asymmetrical – my left side is convex, and the back was apparently “flatter”. Frankly speaking, I have never noticed the latter. I started reading up on cranial asymmetry and I eventually realized that the issues I have are most likely linked to plagiocephaly.
It seems like a hopeless cause, and I am not sure if anything can be done to correct my facial asymmetry. I hope something can be done to bring some harmony between the left and right ear and correct my lopsided smile.
A: In answer to your ear and facial asymmetry questions:
1) You have correctly surmised that changing the position of the ears vertically is not possible as your two previous attempts to do so have failed. Thus leaving them alone is the appropriate choice.
2) Conversely the skull and facial asymmetries are very improvable as your 3D CT scan shows the bony asymmetries of the right back of the head and the left cheek and jawline for which custom implant designs treat those very effectively.
3) The lopsided smile (one mouth corner higher than the other) is challenging since there is no good way to lower the higher left mouth corner side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon