Your Questions
Your Questions
Q: Dr. Eppley, Interested in the surgery to fix my flat head. I been dealing with it my whole life. I’m a 27 year old male. And I wanna get this fixed
A: The first place to start is to get some side view pictures of your head to make assessment and then did imaging to see what type of back of head augmentative change you seek.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, yesI am a 25 years old and all my life I had a webbed neck and could not find a solution for it. Two years ago, I did physical therapy for a month, it helped a little bit and my neck got slimmer from the sides, but when I stopped, my neck got back to its usual shape. Sometimes my neck is slimmer, some days it is wider. My neck is not so stiff usually. Here are the pictures, I wonder if there are any solutions for fixing it from both sides, and from the profile, the access skin under my chin. I do feel any pain around my neck, and my concern is that I just want to have a normal and slim neck, like everybody. If there is any more information I can provide, please let me know. Best regards.
A: In webbed neck surgery the improvement it provides is reduction in the visible webbing from the front and back views. I can not say that much aesthetic improvement is seen in the side view where the webs do not cause any major aesthetic visibility. There is going to be benefit in the stiffness or movement of the neck.
Many webbed necks have a shorter chin projection which I think is an effect of the webbed neck. This will not improve by webbed neck surgery alone. It requires some form of concurrent chin augmentation and/or submental liposuction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a barely noticeable dent”on my brow which was caused by microneedling done years ago. (It seems it killed the flesh.) You seem like the brow expert so I was wondering if you had a permanent solution you could perform–an implant? (That’s super thin, only thick enough to smooth out the dent on my brow)
A: Need to see a picture of the brow concern. Since the problem originated from a soft tissue injury it would seem like a soft tissue solution may be more appropriate. (e.g., filler, fat injections) Not that an implant could not be used just an initial insight based on a description of the problem origin.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a car accident about 30 years ago and had tracheostomy done. I have scar from that and want to see if you can provide options to remove it.
A: That trach scar can be improved by total scar excision and closure. But there will always be s acar. The goal of scar revision, which should be called scar replacement, is to have an improvement in its appearance. There is no way to completely get rid of it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello doctor, I am 2 months after a mandibular advancement + genioplasty and I do not like the result at all because it has lengthened my face. So I want to shorten the bottom of my face, reduce the chin in length and move it back a little + reduce the lower edges of the mandible without touching the angles. However, I am extremely afraid that the soft tissues, muscles, could relax. And therefore end up with a “wizard’s” chin that goes down. And so, I do not know which technique is best for me between shaving or osteotomy. These are slight modifications I think no more than 8mm of reduction in height and maybe 3 of recession. According to you what would be the best technique for me and why? Thank you in advance!
A: Those are big bony changes that are best achieved by redoing the osteotomy not by shaving for the very concern that you have. (tissue sagging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, i would like to know how long it takes to get customized chin implant. I would like to enhance my chin to make it look more square and well-defined with just a little more projection. I don’t want anything too dramatic—just a subtle improvement that gives my face better balance. My local doctor uses implants they are more round shaped. I had jaw implants 9 years ago but it make my face so bulky.
A: You have correctly surmised that when you need a very specific facial implant augmentation change you need a custom implant design. Standard facial implants are made for now historiic facial changes which are different today.
Once a have the 3D CT scan it is a 2 to 3 month process to get designed, manufactured, sterilizied and shipped for surgery. This is largely due to the large number of implant cases that in the process at any one time.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Please see attached images of my eye area and CT scans from after orthagnathic surgery. I’m trying to address the under eye volume loss and sunken look. I think it also makes my cheek look flat as well by extension. Not sure if I should pursue under eye filler or just do a Infraorbital rim implant for a more permanent solution
A: Eye filler is useless for a skeletal deficiency. Custom infraorbital implants is what is best since through their rim saddling design they provide the best undereye hollowing correction effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Does masseter muscle dehiscence resolve itself if the jaw implants are removed or does the masseter still need to be surgically reattached? Thanks.
A: Masseter muscle dehiscence/retraction will not resolve itself by implant removal altbough its aprpearance may become less.
There is no consistently effective method for masseter muscle dehiscence repair.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Dear Dr. Eppley I recently came across information about your chin asymmetry correction surgery using the bone shaving technique. I have a few questions regarding post-surgery care and maintaining the results: Maintaining Chin Results: Is there anything I should do to maintain the state of my chin in the long term after this type of procedure? Are there any recommendations to avoid potential issues such as sagging skin or asymmetry? Botox Use: Would it be necessary to use Botox in the chin muscles after the surgery to prevent muscle activity issues or asymmetry? Excess Tissue Removal: If further adjustments are needed in the future to correct the chin’s shape, would simply removing excess tissue be sufficient, or would more invasive procedures, such as osteotomy, be required? I would appreciate any recommendations you may have. Thank you in advance for your response. https://exploreplasticsurgery.com/bony-chin-asymmetry-correction/
A: Bony chin asymmetry correction may involve bone removal only or a combination of bone removal and soft tissue removal. Each case has to be evaluated on an individual basis. Either way the procedure is intended to provide a permanent correction. Botox injections are not needed for chin asymmetry correction or maintenance after surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there, I have two forehead horns/bumps on my upper forhead that I am interested in having burred down. I still want a feminine and more rounded forehead but I just dont like the two asymetrical bumps on the sides (I did have two head injuries as a child that may have caused these). I wanted to know if a) this can be done with two smaller perpendicular incisions rather than along the front of the hair line (I have seen this in some of your photos) and b) is it possible to get this done under local anesthesia with drugs/gas to make me drowsy? I am very hesitant to go under general and have had other surgeries under local + drugs that have worked well. C) do you ever see cases where scar tissue fills in after the bone burring to be just as bad as before or close to? D) do you need x-ray or CT imaging beforehand? Thanks!
A: Forehead horns are congenital frontal eminence developments that have no coorelation to prior forehea trauma. They can be reduced by bone burring and whether they can be fully reduced is a function oif the bone thickness. This is the value of the CT scan to make that preoperative determination. Access to do the procedure can be done using a limited frontal hairline incision. To keep the incision(s) limited it can not be any further back or perpendicular to the hairline as this prohibits the linear access/visibility to do the procedure. I have not yet seen bony forehead horn regrowth nore would expect that to occur.
Local anesthesia is not an option for me to perform it. Patients that need that technique will need to seek out other surgeons who may be willing to do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Does scapula reduction reduce the length of the shoulders ? Does scapula reduction have any effect on shoulder width?
A: It does not. It is done to reduce the prominence of the scapular spine. It has no effect on shoulder width.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi. I have a facial artery on the left side near the corner of my mouth that is visibly protruding and noticeably pulsating. I have seen a vascular doctor on a few appointments and after close examination, ultrasound, and CT Scan, he has concluded that it is indeed a Facial Artery with Prominent Pulsations. It has become socially uncomfortable and is effecting my occupation/employment. Upon research we learned that this specific facial artery condition is something Dr. Eppley has experience with. Thank you
A: This is a classic presentation off a prominent loop of the facial artery its bifurcation point into the lip and nasolabial fold area. Why it occurs is unknown but I have seen and treated a handful of these cases. Successful ligation/loop removal can be done through a small incision directly over it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi. Sure to a chronic pain issue, I’ve already lost both my testicles to orchiectomy. Having received the largest saline prosthetics available, I’m still not happy with the size, and would like to “upgrade” to a larger size. Do you offer implant revision surgery to place larger prosthetics? Thanks so much for your time and help
A: If you have the largest saline testicle implant that is only 5.0cms in size. My ultrasoft solid testicle implants can be made any size from 5.5cm to 9.0cms.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
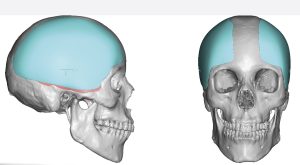
Q: Dr. Eppley, Good afternoon. I would be interested in a skull augmentation and reshaping with the use of scalp expanders. Could you tell me how long I need to keep the expanders on so that the skin can be wide enough for the operation? And what are your prices for this operation, including the cost of the implant? Thank you in advance.
A: Most scalp tissue expanders in two stage skull augmentation procedures are in place from 6 to 8 weeks.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I’m interested in calf implants to straighten my legs . How does the procedure work and any side effects?
A: Calf implants make the calf muscles look bigger but I am not aware that would necessarily make the legs look straighter. I would need to see some leg pictures and do some imaging to see if that makes the legs look straighter. I can see that it might but imaging will prove if that is an actual aesthetic effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon.
Q: Dr. Eppley, Hello I am interested in getting tricep implant surgery. My main concern and goal is, I need them to be sub-muscular. I see Dr. Barry Eppley does the triceps VIA sub-fascia, would it be possible to get them sub-muscular. Please let me know as soon as possible, thank you.
A: Submuscular (on the bone) tricep implants can be done through a medial arm incisional approach. Be aware that the size of submuscular implant is much less in size due to the tighter more limited pocket.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve always had a high hairline/large forehead (shown in my attached photo) and have been exploring surgery to lower my hairline. Is this something that you could help with – or perhaps something with hair transplant surgery coupled with hairline lowering? I do use topical minoxidil (I have a little bit of hairless that this has helped with). Happy to schedule a consultation if you think it would be appropriate. Thank you!
A: Thank you for your inquiry. Frontal hairline advancement in men is a challenging procedure that must be considered very carefully. The male frontal hairline poses many different considerations than that of women. Issues such as hair density, pattern of the frontal hairline, patient expectations of where they like their hairline to be and how much natural scalp laxity they have or play a role in whether is a good candidate for the surgery. This is not to mention that the risks of having a frontal hairline scar are different than that of women whose frontal hairline is likely much more stable.
To make a better determination of whether this is an option for you I would need pictures of your frontal hairline from different angles as well as what you envision or where you would like your frontal hairline to be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I would like to schedule a virtual consultation with Dr Eppley to ask about custom implants to fix my deep undereye hollows and lack of midface volume. I would like to hear his solution for my case.
A:Thank you for sending your pictures. You have general periorbital rim weakness/flattening which is most manifest in the infraorbital rims which is why they look so hollow. Infraorbital rim augmentation would be the best approach. (see attached imaging) The only question is whether that is best done with a custom infraorbital implant or a sheet Alloderm graft….both which can be effective. Given your young age I lean towards the latter but that is a topic up for further discussion.
But if the goal is also to have some midface volume as well then the custom midface implant is the way to go.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello ,a question regarding muscle implants can they be implanted in any visible muscle ? l await Your response Regards
A:In theory that would be correct. The only question would be implant pocket location…whether that would be on top of the fascia, subfascial, intramuscular or submuscular. That would depend on the specific muscle location
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am trying to improve flat sagging buttocks as an older female? I’m hoping to get a more full shape with some outward volume as well. Fitting for my size and shape but significantly more than the flat bottom I’ve always had.
A:Thank you for sending your buttock pictures. Your buttocks has a two-fold tissue issue…lack of volume and lower buttock sag or ptosis. While the volume of implant will certainly be helpful in filling out the upper and mid-buttock areas, and will help pick up loose skin in those areas, it is not going to lift up the lower third of the buttocks or get rid of the lower buttock tissue sag. (see attached diagram) That can only be corrected with a lower buttock excision/tuck/lift. The question in that regard is whether the lower buttock sag excision correction should be done at the same time as the buttock implants. From an efficiency/convenience standpoint yes. But from a recovery/scarring standpoint maybe no?? An issue that merits further discussion.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a few questions about webbed neck surgery:
So if I understand, the posterior approach will slightly straighten the neck?
Can you briefly describe what happens during the posterior and how long does the recovery process last?
Will it be possible to loosen the trapezius muscles with some physical therapy or kinesiotherapy?
Can the side profile be fully fixed with sliding genioplasty and a chin filler?
A:In answer to your webbed neck surgery questions;
1) The posterior approach does NOT straighten the neck. The posterior approach is used tp put the scars in a more favorable location than the side of the neck.
2) I would recommend that you visit www.exploreplasticsurgery.com and search under Webbed Neck surgery where you read and see that posterior approach to fully understand it.
3) The trapezius muscles can NOT be surgically loosened.
4) The chin position can be fully corrected in side profile and illustrated in the prior imaging. The amount of chin augmentation shown was just one potential type of change, more or less can also be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I underwent a frontal craniotomy due to a brain tumor, and it left a bone dent and a bulging bone part in my forehead.. What options would you recommend for surgery? And would it be possible to give an estimation of the cost? Thank you
A:Give that this was from a prior craniotomy where a large incision exists for access and there remains bone gaps in the depressed bone flap the use of hydroxyapatite bone cement to fill and smooth over the defect would be the most prudent material approach for forehead recontouring.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am an adult with what I believe to be scaphocephaly that was untreated as a baby and wish to have it looked upon by a specialist that can help me I would really want this fixed for me and my future.
 A:In adults I typically treat the long narrow scaphocephalic skull shape with custom head widening implants. (see attached example of the implant concept) This may also involve some bony reductions as well if aesthetically beneficial and incisional access will permit of the sagittal crest as well as the front and back of the head.
A:In adults I typically treat the long narrow scaphocephalic skull shape with custom head widening implants. (see attached example of the implant concept) This may also involve some bony reductions as well if aesthetically beneficial and incisional access will permit of the sagittal crest as well as the front and back of the head.
I would need to see a front and side view pictures of your head for an assessment and imaging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 28 years old and all my life I had a webbed neck and could not find a solution for it. Two years ago, I did physical therapy for a month, it helped a little bit and my neck got slimmer from the sides, but when I stopped, my neck got back to its usual shape. Sometimes my neck is slimmer, some days it is wider. My neck is not so stiff usually. Here are the pictures, I wonder if there are any solutions for fixing it from both sides, and from the profile, the access skin under my chin. I do feel any pain around my neck, and my concern is that I just want to have a normal and slim neck, like everybody. If there is any more information I can provide, please let me know. Best regards
A:You have what I call a mosaic type webbed neck which means it is a moderate webbed neck that is associated with tighter tissues than the full expression of a Turner’s webbed neck where the neck webs are wider with looser/more supple tissues. Improvement in the neck webs is possibloethrough a posterior approach. (see attached imaging) But I would never call it a complete correction or the making of a perfectly normal straight line neck profile. The widened trapezius muscles prevent that complete degree of correction.
Many webbed necks are associated with shorter chins which is a result of the webbed neck. Unless one undergoes a concurrent sliding genioplasty (see attached imaging) the excess tissue under the chin will remain as the submental area is too far away to be affected by the posterior neck tissue movement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello Have you ever seen case where jaw implants went through skin 8 months after surgery? Intraoral placement, genioplasty before (10 mm forward 3 mm down), chin implant before all of these. After 2 months skin thinning, later scarring, scar burst, red fluid 5 days now yellow fluid no symptoms, sometimes pain when eating hard food. Have my surgeon achieved unique result? I did not find anyone with such problem. Now they want to remove all 3 segments which is disaster. Probably it is because those in the Netherlands prohibited silicone implants. (mine is polyethylene and it was too big)
A:These are not implant-related complications I have ever seen. But it is implants and there is a delicate balance between tolerance and problems which can occur if the implant is too big and/or in the face of chronic infection. The first ominous sign was the skin thinning at 2 months after surgery at which time action would have been prudent as this was a sign that the balance had been tipped unfavorably.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I really would like to see what can be done to address my undereye areas bags, perhaps with an orbital rim implant? And then finally my main concern, the upper third of my face, I don’t hate the brow prominence in and of itself however I would like for some way to ease the transition between brow and forehead. These two problems combined give me a very tired and deficient look from many angles which I hate. Some angles is fine however and when there isn’t a direct lighting the transition is much smoother.
A:You are referring to a combination orbital rim issue with the superior orbital rims (brow bones) too far forward and the infraorbital rims too far back. Thus a combination of brow bone reduction and infraorbital rim augmentation would be the corrective approach. Your face pictures are taken from a far distance so there quality is not great but at least in the side view I have imaged the concept of the potential orbital rim changes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to shorten the nose vertically? Most rhinoplasty results I have seen is because the tip is droopy or long. But in my case the bridge bone looks long and my nostril is lower than my tip. I haven’t seen it done but is it possible to cut/reduce the septal cartilage and reposition the nostril. I hated the way it look long from the front , it looks too far from my eyes.
A:While tip rotation involves making the tip shorter and more uplifted which is a common rhinoplasty change you are referring to a whole nose vertical shortening which is not possible.
.Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Could a surgical hairline advancement be safely preformed via an incision at the hairline in the future if I had a behind the hairline coronal incision already made? If it’s possible without a risk of necrosis or tissue ischemia please let me know how long one would have to wait to have this done. Thank you.
A: No…that would be a very risky procedure for the very reason you have mentioned.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to you because of my facial asymmetry, especially of the eyes, that I am looking to correct. My right eye is positioned lower than the left one and canthal tilt is more negative. Furthermore, my right eye is more hooded and its superolateral orbital ridge sits lower. While my right cheek area lacks volume, on the right side my jaw is more prominent. I was thinking of cheek (right side) and jaw (left side) implants. Concerning my right eye, I was thinking of canthopexy or canthoplasty and brow lift, maybe even orbital floor implant and reduction of the superolateral orbital ridge. What procedures do you think would be most effective in achieving a more symmetric appearance? And what steps would I have to take next to plan surgery with you.
A:Everything you have described is classic for a right vertical orbital dystopia (VOD) including the procedures you have mentioned to address it. An assessment of which VOD and other procedures may be beneficial requires a picture assessment (front view) and a 3D CT face scan which I assume you have not yet had. (you should be able to get that in your country)
Once I have that information I could provide an informed opinion about what the optimal corrective procedures may be. Usually the front view pictures tell us what we need to do and the 3D CT scan provides confirmation of those bony needs as well as serves as the platform on which to build any implants if needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had Medpor jaw implants in 2012. In comparing the two sides of my face there is a marked ‘bump’ where the implant is. The goal would be to produce smoother jaw line, to the extent possible (compare with the other side of the face). My fingers show the beginning and end of the implant.
I expect a small reduction in thickness should be enough, but along most of the implant length.There are still screws inside. My doctor said that they can now be removed (during the surgery) The implant on this side feels less regular to my finger. Especially the bottom-outside edge feels sharper and more ‘to the outside’ (this edge is causing the prominence), while the implant on the other side appears more closely following the natural bone.
Very much looking forward to a reply.
A:If I interpret these pictures properly what you are seeking is a width reduction of the implant with a length located between your two fingers along the jawline to which I can say:
1) That cannot be done from the submental incision. It is one thing to put the implant in that way but you are never going to revise that areas of the implant from that approach.
2) This would have to be done from an intraoral approach a direct incision on the bottom edge of the implant to do so..
3) At the location of the most anterior part of the implant lies the exit of the mental nerve from the bone. (marked on your picture as a red vertical line) You would be wise to stay away from that part of the implant to avoid any risk of permanent numbness of the lower lip.
Dr. Barry Eppley
World-Renowned Plastic Surgeon