Your Questions
Your Questions
Q: Dr. Eppley,Wondering if the lump on my forehead is a pseudolipoma from trauma and if Kybella would work to help flatten it, or, if another procedure would be more appropriate.
A:I am not sure what a pseudo-lipoma is. But it is more likely, because it has occurred from trauma, of being an osteoma. But whatever the pathology is it is highly unlikely Kybella injections would be effective for its reduction. It is going to require surgical removal.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, would it be possible to deproject the radix slightly, to give the illusion of a brow ridge (assuming my radix is already really outgrown) (it looks kind of like those blue avatar people from the side profile). I attached a morph of my nose (the first is unedited, with just me pulling back the soft tissue to show the bone more clearly, and the second is how i would want it to look). Do think a result like this is achievable without making my nose slope straight down from my forehead (The main issue isn’t that it’s too big, even though it is too big, the issue isn’t that is molds into my forehead and makes it look super flat). Any advice or help would be greatly appreciated, thank you.
A:While I see no attachment that shows your morphed nasal changes I can tell you that reduction of the high nasal radix is one of the hardest things to do in all of rhinoplasty surgery because it is a bone structure located in the no man zone between the nose and the forehead where there is limited surgical access. I have done numerous high radix reductions through a dual osteotome technique from an intranasal and a percutaneous approach. Whether your ideal morphed changes are achievable would require an actual assessment of that image.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am interested in improving the appearance of the area above my lips and softening my lip lines. I am also interested in lip surgery or augmentation for my upper lip which is basically non existent now at the age of 51. Improved volume and symmetry in both the upper and lower lip is desired. I have been looking for a surgeon that has a specialization in this area. I was excited to see so many examples in the photo gallery. Looking forward to seeing what the possibilities are. I had two prior consultations wbut in the end did not feel they were the right doctors for me.
A: Thank you for your inquiry and sending your pictured. You have four aesthetic lip issues: 1) a very long upper lip with a lot of skin between the nose and the upper lip vermilion, 2) small vermilion height (pencil lip), 3) vertical lip lines (wrinkles) and 4) a larger but still small lower lip vermilion/size with central vertical lip lines
Because of the amount of nasal base/sill show I don’t recommend a subnasal lip lift. The upper lip vermilion advancement is better because it changes the entire vermilion from one side to the other and will also diretcly remove those lip lines in the zone of excision. Because of the central lower lip lines and to keep the lip size proportionate a 2mm lower lip advancement would be helpful as well. (see attached diagram)
While I believe pip advancements would be the only effective surgical lip augmentation method it does create fine line lip scars so one needs to be cognizant of that tradeoff.
Vertical lip lines are a very difficult problem to improve long term due to their dynamic cause (lip movements) and occur almost exclusively in Caucasian females due to their thinner skin. The only treatment is laser resurfacing but I don’t recommend that at the same time as the lip advancements as it may make negatively affect the vermilion-cutaneous scar lines.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Five years ago I got my first set of implants 500cc smooth round dual plane moderate plus implants. After drop and fluff I lost alot of the volume and was left disappointed. One year later I revised my breasts. I got 800cc smooth round high profile implants and they were phenomenal!
Last year I gave birth to my final child and I breast fed for 12 week. My boobs were full and robust when the milk came in but after breast feeding they have now softened and finally dropped.
I wish to get either these two silicone breast implants
1050cc motiva
1135cc mentor (maybe 1240cc)
Keep the dual plane placement for a more natural look
I have been told by three plastic surgeons that they don’t go any bigger in implant and they suggest I get a lift. I believe a lift wouldn’t help my goal as that is taking skin away from the area when all I want is to fill the area
A: Thank you for sending your pictures. The question is not whether you can increase your breast implant size to greater than 1000ccs but whether it will have the effect you ideally desire. It will increase your breast size for certain but it will not have much of a lifting effect. Technically your prior consultations were correct in that a lift is the only way to change the now imbalance of upper pole tissue vs lower pole tissue. Bur given the magnitude of that ‘problem’ the tradeoff of the scars would be aesthetically ill-advised.
When increasing breast implant size greater than 800ccs with an already good result there are several basic principles to be aware:
1) The larger breast implant size should not violate the existing capsule that already exists particularly the inferior and lateral capsule borders to make the implant fit. When that is done implant malposition/drop may result creating a problem that is very difficult to correct due to the weight of the implants. While I am confident that you can go from 800cc to 1000cc with a low risk of that concern how much beyond that can not be predicted in advance. But as a general rule most patients can not safely go beyond a 30% size increase.
2) It is also important to be aware in any aesthetic implant surgery, including breast implants, that past history (lack of any significant problems like infection, capsular contracture, asymmetry etc) is not a guarantee of a future uncomplicated aesthetic outcome.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Could you please tell me what the exact issue is with my forehead structure? Based on the photos I sent, do you think I am a good candidate for forehead contouring surgery?
I would also like to know:
- What procedure would be recommended in my case?
- What kind of results can realistically be achieved?
- How long does the surgery usually take?
- Is the procedure considered high risk?
- What are the possible complications?
I would appreciate your professional opinion and guidance.
Thank you very much for your time.
A: Based on your pictures I assume you are referring to your rounder more convex forehead shape, particularly the upper forehead bossing and increased forehead width. (see attached pictures)
The success of a bony forehead reduction depends on whether the frontal bone is thick enough to allow for a safe and effective reduction. That is determined preoperatively by a 3D CT skull scan with color mapping of the bone thicknesses.
The biggest aesthetic issue in considering the procedure is one of access, the incision needed to do the procedure. Only a frontal hairline incision can provide adequate access (see attached picture)
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I had double jaw surgery around 6 months ago and had impaction because of downward growth. I am now trying to improve my eyes that have droopy eyelids and a fairly negative tilt. While most surgeons seem to say a canthopexy would fix this, could there be a more skeletal problem related to a negative tilt eye shape? I am afraid to be dissapointed by canthopexy results. Are canthal tilt related issues related to something that is skin and muscle or more skull related? I attached pictures of my current eye shape from both the front and the side. It does not appear to have been affected by my jaw surgery at all. Is making an eye shape change even possible? Would getting something such as infra orbital implants or a fat graft be enough to make a shape change, or would it need to be a more complex procedure?
A: By definition when you do double jaw surgery, if there is any significant advancement, you leave the orbital area behind. The maxillary osteotomy cut is well below the infraorbital rims and cheekbones. Thus some patients will develop an orbital or orbital-malar deficiency afterwards particularely those patients that has some mild deficiency beforehand (which I suspect was you).
While I don’t know what yoru orbital area looked like beforehand you have a negative orbital vector now. Givn that the shape of the lower eyelids follows the shape of the bone underneath it the lower lids swoop done out laterally with a low outer corner posiiton amd increased scleral show.
This is a facial condition that i see all the time and the correct strategy miust be based on structural infraorbital-malar augmentation and lower eyelid elevation. What will absolutely not work are lateral canthopexies alone or fat grafting. While a lateral canthiplasty is needed as part of the structural augmentation it will fail when trying to do so without structural augmentation done underneath to support the vertical eyelid lengthening. When a skeletal deficiency exists fat graftng is always a poor treatnent choice patticularly in the orbital area where teh volume persistenjce is close to zero and soft tissue addition (even iof it survived) can not support lower eyelid repositiioning.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley I’m interested in the testicle enhancement surgery and have a question. I’m. 52 years old and my testicles have atrophied significantly over the years and at some point in the next couple years I would like to have the type enhancement surgery you offer. My issue is I also have severe testicle retraction due to a botched hernia surgery years ago in addition to extremely overactive cremaster muscles. This causes my testicles to ride extremely high or inside me and are basically impossible to pull down very much. I was thinking about possibly having the microsurgical cremaster muscle release procedure but is it even necessary if I have testicle enhancement like you offer which displaces my natural testicles? I’d appreciate any information you can provide me regarding this issue.
A: Your situation is not one that I have yet encountered. In theory one would think that retracted testicles would be very favorable for the implant displacement method for the obvious reason that they are already ‘displaced’ superiorly and any risk of postoperartive testicle show would be greatly reduced or eliminated. On the other hand a hyperactive cremaster muscle may not necessarily relax after implant placement and may be a potential source of pain or chronic discomfort.
In short without actual clinical experience I can only speculate about the risk:benefiit ratio.
Dr. Barry Eppley
Q: Dr. Eppley, I’ve always had a very large forehead that kind of comes to a point on top. I was looking into forehead reduction or hair transplant on the top maybe half inch area of my forehead to make it more harmonious. Thanks!
A: With a need for a more limited central hairline AND a bony prominence the frontal hairline offers the ability to do both while keep a robust frontal hairline density. If reduction of the bony prominence is not that important and a little less hairline density can be tolerated then hair transplantation would be a good option.
Dr. Barry Eppley
Q: Dr. Eppley, I am seeking a consultation regarding calf implants. My legs were always thin but following an Achilles rupture my left ower leg is significantly disproportionate and I cannot seem to rebuild the muscle despite years of training. My left is roughly 12.5” and my right is roughly 13.5”.Thanks!
A: Thank you for sending your pictures. Despite the asymmetry you have very thin lower legs and they are so thin that I initially thought you might have had congenital clubfoot. The first key question is whether the goal is to have the smaller calf match the larger calf or to enlarge both calfs. For now I will assume it is the latter. Your calfs are so small that I don’t think you can successfully have implants placed under the muscle fascia in the traditional location. Your calf muscles are very small and tight and not much of an implant could be placed under them. You would have to have subcutaneous implants which need to be different sizes due to your asymmetry. These needs require custom calf implant designs.
Dr. Barry Eppley
Q: Dr. Eppley, I have been getting lip filler for eight years and have tried numerous types of filler, numerous techniques and numerous injectors, and I always suffer from lip migration. To be honest, I was not blessed with lips and my goals are to have more “lip shape” than volume because I love the look of large full lips that are flatter than projected. I’ve been researching for the past two years about the lip advancement technique, and your work is stunning! I wanted to know if I would be a good candidate for upper and lower lip advancements being someone who is naturally tan and not naturally blessed with any kind of lip whatsoever. I have not done lip filler in 2 1/2 years, but I still feel as though I have some residual filler in my lips. I always used Restalyne Kysse or Juvederm. Thank you kindly for your help!
A: Compared to many lip advancement patients your lips are very full by comparison (even minus the residual filler) But even fuller lips can undergo vermilion advancements. Having intermediate skin pigmentation slightly increases the risk of more visible scarring. But the real risk factor in that regard is how much vermilion advancement is being done and does it need to cross the cupid’s bow area. It seems like your lips are most ‘deficient’ laterally more than centally (see attached picture) which would also be the safest approach to minimize scarring.
Dr. Barry Eppley
Q: Dr. Eppley, Where can I find more information on the total cost of a pelvic plasty?
A: The pelvic plasty procedure has three variations to it, 1) titanium crest plate alone, 2) titanium crest plate +silicone hip implant and 3) titanium crest plate + hip fat grafting. Which method is determined on an individual basis. But the most commonly used technique is #2.
Dr. Barry Eppley
Q: Dr. Eppley, I have had a facial fat transfer to the cheeks and am unhappy with the results. Is removing transferred fat graft something that cam be done?
A: Removing fat from the cheeks is very challenging to do. It is easy to inject the fat, far more difficult to reverse or remove it. Whether some improvements can be made and what procedures are needed to do it depends on knowing the following information:
1) When was the procedure performed?
2) How much fat was injected?
3) Evaluating before and after pictiures
4) What area of the cheeks is the most bothersome (draw on a picture to show it)
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I had Medpor infraorbital implants placed back in 2024 to correct my negative vector, and the outcome is poor. The scar tissue around the implant has created visible deformities under my eyes, is slightly pulling my lower lids down, and causes a constant feeling of tightness and discomfort. Several oculoplastic surgeons have assessed my situation and none recommend removal at this time, however the appearance and sensation are causing me a great deal of distress. What would you recommend? Thank you.
A: I think it is clear that these infraorbital implants you have in are better out than in, regardlrss of what any surgeons have said. They likely did not recimmend remnovals because they are either inexperienced with removing Medpor implants or didn’t know what to do once thet are out.
The latter concern is the key one. The question is not whether they can be removed…as they can…but what are going to do in their place. This is very relevant for two reasons:
1) There is a reason you and them initially placed (negative orbital vector), and
2) The soft tissue around the lower orbits and cheek is going to be worsened than before they were placed. (lower lid retraction)
Thus there has to be a concomitant plan for replacement. Whether this is custom infraorbital-malar implants , dermal-fat grafts etc remains to be determined.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, would I be able to talk to you about skull reshaping? In terms of vertical height. Its the vertical height for me that I really don’t like
A: I believe you are likely referring to the posterior sagittal bump which would be the highest part of the top of your head. (see attached pictures) That can be reduced based on the thickness of the bone which is preoperatively assessed by a 3D CT skull scan with color thickness mappning to ensure an adequate but safe reduction can be achieved.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I’m interested in an extended corner mouth lift for my downturned mouth. One year ago I had a corner lip lift procedure done in Dallas Tx. Unfortunately it did nothing to help my droopy dog problem.
A: What you previously had was not a corner lip lift. It was a lateral vermilion advancement, which can create some increased lateral lip fullness, but is not intended to provide any corner lip lift. The cutout pattern used had no chance to create that effect. To achieve that type of mouth corner change the cut out pattern must resemble that shown in the attached imaging.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I do have an area of spongy tissue centered below lower lip vermilion c/w involuted hemangioma tissue. Tissue with some irregularities and Mild transverse crease between involuted tissue and vermilion. I hate it.. It’s residual from hemangioma from when i was infant. Told by numerous plastic surgeons in Beverly Hills that surgery is dicey because it may not look good enough.
A: I don’t know what that area below the lower lip looks like when you are not pursing your lips (as seen in the current picture) but it is already an irregular tissue area….which is typical for an involuted hemangioma. Thus the issue is whether an open excision would make the area look better (less projected and smoother), heal with the same irregularities in the long run but not as full or projected or look worse (more irregular). If you were only looking at these three potential outcomes on an even statistical basis only one of them makes it really better. This is what the term of ‘dicey’ really means.
But beyond a theoretical even statistical basis for each potential outcome I suspect that making it look worse is unlikely. The real debate is how much better in appearance can surgery make it…..a little or a major improvement in appearance. Unfortunately that is a question that no one can really answer. The only way to know for sure is to actually do the surgery.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have deep-set eyes, and I wanna ask if there is a surgery to make my eyes actually forward? My eyes’ surroundings are not deep but the eyeballs as what I see, and it’s been like this since I was young. It affects the appearance of my eyes a lot. And I’ve read about Orbital Implants/Surgery, and Orbital Volume Augmentation, where something is put behind the eyes making the eyes appear actually forward. I don’t know if it’s actually possible, but for cosmetic reasons. I also read that it can be possible for cosmetic reasons but a very small number of surgeons offer it for cosmetic purposes. And it’s making me so confused. Please let me know if it’s possible or not
A: There is no safe and/or effective procedure for bringing the eyes forward. Certainly not for the aesthetic patient who has had no prior orbital injuries or surgery.
Dr. Barry Eppley
Plastic Surgeon
Q:Dr. Eppley, I want to get a full head reduction , back of head reduction and forehead reduction as well as top of head reduction, can Dr Eppley look at these and be able to help with this?
A: Thank you for your inquiry and sending your pictures. In skull reduction surgery, particularly those that involve multi-surface areas, the two key preoperative considerations are: adequate bone thickness to permit an effective and safe reduction, and 2) enough incisional length to successfully perform the procedure.
That information is acquired by: 1) a 3D Skull CT scan with color mapping of bone thicknesses, and 2) patient acceptance of a bicoronal scalp incision which is necesary to have adequate exposure of the front, top and back of the skull bone surface areas.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I recently had full FFS. I was not aware that brow bossing reductio would remove my bone around my eyes removing the sultry look I once had leaving me looking skeletal. I see that you do implants around the eyes and I’m hoping maybe you can help me. I would also love to see outcomes of people with similar issues and if these implants would last for life. I left some new images where there’s clearly missing bone and some old pictures where you can see how nice my eyes used to look.
A: Brow bone reduction by bone flap setback is the most common procedure performed in FFS surgery. Restoration of the lost brow bone projection can only be done by a custom brow bone implant. As the popularity of FFS continues the need to partially or full reverse brow bone reductions is also be done more frequently. Ideally the implant design is done using the preoperative FFS surgery 3D CT scan if it is available.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I used to have braces and my teeth have a good alignment, however my lower jaw/chin go further back than I would like it to. When I stick my lower jaw past my upper and my bottom teeth are more forward than the top row, I like that appearance better. Is this something a sliding genioplasty could achieve? (Photos attached include me biting down normally and me forcing my lower jaw forwards for the desired look)
A: What you are doing by jutting your jaw forward and biting down is creating a total jaw augmentation effect. (chin and jaw angles) This is more than just a chin augmentation effect alone. A sliding genioplasty can certainly create the chin augmentation but not that of the masseter muscle enlargement.
Dr. Barry Eppley
Q: Dr. Eppley, I’m writing to inquire about medical or aesthetic options to improve the width and overall fullness of my lips. I naturally have relatively small lips and would like to understand what safe, effective treatments are available to achieve a wider and more balanced appearance. Could you please let me know: What procedures you offer for lip widening or enhancement (e.g., fillers, surgical options, or other techniques)? Whether these treatments primarily increase volume, width, or both How natural the results typically look Any risks, downtime, or long-term considerations
A: Thank you for your inquiry and sending your picture. The fundamental aesthetic lip issue is the mouth size or a lack of adequate horizontal lip width. Without more lip width you can’t have any vertical lip size increase without looking disproportionate.
To create more lip width, aka mouth widening, the vermilion around the mouth corners has to be advanced by removing skin and relocating the vermilion corner in to it. This creates fine line scars around the vermilion edges in so doing. There is a delicate balance between how much the mouh is widened and the resultant scars.
While scars are always a tradeoff for many aesthetic procedures, in any form of vermilion advancement that is always a significant consideration.
Dr. Barry Eppley
Q: Dr. Eppley, I had hip implants placed and you can visibly see they’re not long enough or wide enough and aren’t the right shape or size for my hip area. I would like new hip implants to be thicker, longer and wider. Covering the entirety of my hip area and wrapping around the back as much as possible.
A: Thank you for your inquiry and sending your pictures. I would have to now some more information about your hip implants (dimensions, when placed, surgical incision location) but I can certainly see your concerns/objectives. These are hip implants that are isolated to the subiliac hollow area of which the outlines of the implants can be seen.
While the aesthetic outcome of the hip augmentation may be less than ideal, it is important to recognize that they were placed and have healed uneventfully without medical complications (infection, chronic seromas). When you consider replacing such implants for a larger and improved result those surgical risks are going to be reincurred and you may or may not be so fortunate the next time. While this is relevant to all implants it is particularly poignant in hip implants which have the highest complication rates of all aesthetic body implants due to their more superficial tissue pocket location.
Thus in considering hip implant replacements with a focus on trying to minimize these risks it is important to not get ‘greedy’…meaning keep the replacement implants reasonable in surface area coverage and thickness. Don’t try to make them do too much. Some more is better, a lot more could be disastrous.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I submitted paperwork online for a virtual consult with Dr. Eppley regarding custom jawline implants and I just wanted to follow-up about scheduling an appointment. My understanding is that I’ll likely need a ~3D CBCT scan of some sort for him to take a closer look at my jaw and assess how plausible my goal/plan is, so if that is indeed necessary before a consult.
A: While a 3D CT scan is needed for the designing of a custom implant it is not necessary for the initial virtual consultation. The scan is the platform on which a custom implant is designed but it does not tell us how to design it. That guidance comes from imaging of the patient’s pictures.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I just retired and I’m built like a brick house.Now I would like to be much more feminine looking figure wise. I’ve seen people who received rib contouring and I wasn’t impressed with the results. I have only seen one Dr. Eppley’s patients who had the procedure and they looked great, 100 times better than rib contouring.
I researched both rib contouring and rib removal and I think removal is the best option for me.
A: Thank you for sending your pictures. Rib removal surgery works best and should only be performed on lean patients where the only obstruction is structural (bony). In patients that have some significant skin laxity and a thicker subcutaneous fat layer procedures that address those issues should be done first. In your case an extended tummy tuck with lateral oblique plication with flank and back liposuction will get much better results than rib removal alone.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have a narrow face and would like to add facial width. Is this possible through implants? It’s just overall narrow and would like for it to be a bit wider. Also if there is are there risks? Like will it ruin facial harmony since the facial features stay the same but the bone seems widened?
A: The only way to increase facial width is with implants. The best way to assess those potential widening effects and as to determine how much widening you prefer is imaging predictions based on your own pictures. To do so I would need a non-smiling front view facial picture.
Dr. Barry Eppley
Plastic Surgeon
Q:Dr. Eppley, Hello! I found your practice online because I have been researching sliding genioplasty reversals. I am interested in having a sliding genioplasty reversal. I had a sliding genioplasty 7 years ago with a 4mm advancement forward. Unfortunately, it made my face look significantly longer and wider. I would like to learn more about sliding genioplasty reversals and go over which options would be best. I would ultimately like to have a shorter more narrow chin. Please let me know if I am a candidate and if a reversal or chin shaving surgery would be best for me. Thank you.
A: As you have metioned there are two methods for ‘chin reduction’ after a sliding genioplasty, submental chin shaving and secondary sliding genioplasty, both of which can create vertical height reduction and width narrowing. Each method has their advantages and disadvantages. Chin shaving avoids an intraoral osteotomy approach at the expense of a submental incision/scar. The osteotomy method avoids a submental scar but is prone to increased risks of bony irregularities and some redundant submental tissue laxity.
In essence there is no perfect way to do it without risks/tradeoffs. Augmenting the chin is ‘easy’ but reducing introduces new issues that were not as pertinent as the first surgery.
One major consideration is what degree of changes are needed. If there are only minor amounts (a few millimeters) vertical and width change then the submental shaving method would be more appropriate. However if the changes needed ar more significant then the osteotomy method may be preferred.
Dr. Barry Eppley
Plastic Surgeon
Q:Dr. Eppley, ı wanna learn about this iliac crest reduction.I got wide hips and ı wanna change that.
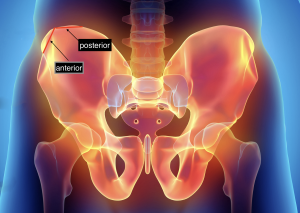 A: On the basis of your pictures it looks like you are referring to the whole of the iliac crest, both anterior and posterior portions. Iliac crest reductions are typically done on the widest anterior portion of the crest as the posterior portion is not usually visible and is harder to access (see attached image) I suspect in a thinner patient where the posterior portion may be more prominent/visible it could be reduced as well…but I have never yet done it.
A: On the basis of your pictures it looks like you are referring to the whole of the iliac crest, both anterior and posterior portions. Iliac crest reductions are typically done on the widest anterior portion of the crest as the posterior portion is not usually visible and is harder to access (see attached image) I suspect in a thinner patient where the posterior portion may be more prominent/visible it could be reduced as well…but I have never yet done it.
Dr. Barry Eppley
Q: Dr. Eppley, I have a facelift last year and my tragus was removed. I would like to reconstruct a new tragus.
A:This is a far bigger problem to correct than you think. This is a classic example of a facelift that was done were all of the tension has been put on the skin level at the ear resulting in loss of the tragus, a pixie ear and hypertrophic scars behind the ear. The only way to approach correction is to redo the facelift and re-elevate the skin flaps to create more skin around the ear which may be able to support a cartilage graft for the tragus, reduce the pixie earlobe while keeping the scar underneath it as well as narrowing the scars behind the ear. Whether you now have enough skin to be able to do that depends on how far out you are from the original facelift surgery as well as is there any residual skin laxity
Dr. Barry Eppley
Q: Dr. Eppley, Hello I have interest in possible solid tear trough implants. I see one pic showing before and after from profile view of tart trough implants can you please Share more pics of tear trough implants? It seems everyone just does fat transfer or filler but I don’t understand why. Does this implant get screwed in under the eyes? Please advise thank you
A:Tear trough implants are a very specific type of iinfraorbital implant and the only type of infraorbital mplant that is available as an off-the-shelf item. By its history it Is designed to treat, as the name indicates, tear troughs which are grooves are indentations limited to the inner half of the infraorbital rim. They should be distinguished from under eye hollows which affects the entire infraorbital rim and are treated by custom infraorbital rim implant designs. Thus the first question is what are you specifically trying to treat as that will determine whether standard teardrop implants are appropriate for you.
But regardless of the type infraorbital rim implant they are placed through lower eyelids incisions and are secured with small micro screws.
Dr. Barry Eppley
Q: Dr. Eppley, Hello, I am interested in infraorbital and submalar facial implants. I have done a CBCT which I can share.
A: A CBCT scan may or may not include adequate data on the infraorbital rim area so I would have to see some pictures of it to see if it does. Regardless the scan does not provide information on how to design the implants, it is merely the platform on which they are designed. Design information comes from analyzing your pictures and doing imaging to determine what your desired aesthetic midface augmentation goals are.
Dr. Barry Eppley