Your Questions
Your Questions
Q: Dr. Eppley, Interested in forehead augmentation with PMMA bone cement for slight dents/ flat forehead.
A:In forehead augmentations today there are two materials to use, hydroxyapatite bone cement and custom forehead implants. The use of PMMA bone cement is, by comparison. is an historic and inferior material to use for this or any form of skull augmentation. As a result I do not use it anymore. That being said the more pertinent question is whether an HA bone cement or custom forehead implant offers superior aesthetic results . To make that determination I would need to see some pictures of your forehead that shows your concerns.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am planning a total facial reconstruction to transform my oblong face into a square-shaped aesthetic using custom implants. Since this is a massive financial investment for me, I am concerned about the risk of infection.
Is it possible, with current or upcoming technology, to treat a severe infection by cleaning and disinfecting the existing custom implants (like PEEK or Titanium) and re-inserting them, rather than having to completely discard them and pay for a brand-new set? Are there any specific materials or protocols you use that allow for salvaging the original implants even in the case of a significant infection?
I appreciate your expert guidance on this as I plan my long-term transformation.
I would also like to ask about the future of implant technology. As a medical student planning this for 2040, I am curious if there are any ongoing research or upcoming materials—such as antibiotic-eluting PEEK, silver-nano coated surfaces, or bio-active scaffolds—that are specifically designed to be ‘infection-proof’ or treatable without removal?
Since a full facial reconstruction is a significant long-term investment, I want to know if the field is moving towards materials that allow for deep disinfection and salvage in the event of a severe infection. Any insights into current clinical trials or future trends in material science for custom implants would be incredibly helpful.
Apologies for the specific year mentioned earlier; that was meant to highlight my long-term commitment. However, I want to clarify that if the current technology already offers implants that are infection-resistant or treatable without removal, I am ready to move forward with the procedure as soon as possible. My priority is the safety and longevity of the reconstruction, and I am eager to learn about the best materials available today that meet these criteria.
A:In assessment of the risk of infection in facial implants that risk changes considerably depending upon where on the face they are placed. In my extensive facial implant experience over 35 years I have yet to see an implant infection of the forehead, orbital or cheek areas in which the implants were placed transcutaneously. Almost all implant related infections come from the intraoral placement in the lower midface and lower jaw. That risk is in the 1% to 2% range.
I do not see into the foreseeable future any developments implant technology, by material or design, that will eliminate the known risks of implant related infections that exist today.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have long been concerned with the shape of my head, specifically feeling that it is too narrow in certain areas. My goal is to achieve a more rounded, symmetrical appearance. Before scheduling an appointment, I would appreciate knowing: Do you perform customized skull implants (using PEEK or PMMA) or bone contouring for aesthetic purposes? What is your typical process for a CT-scan-based evaluation to determine bone thickness? Are there non-surgical options (such as high-density fillers) you recommend for this specific concern?
A:When it comes to aesthetic skull augmentation I can provide you with the following answers to your questions:
1) There are no existing injectable fillers that can provide any defective or persistent skull augmentation defects. Only implants can do so.
2) Any type of skull implant is made custom based on the patient’s 3-D CT scan.
3) When it comes to custom skull implant materials the best option remains solid silicone in terms of both tissue tolerance, desired shape and ease of insertion. While they can be made out of PEEK that requires a full bicoronal scalp incision with wide detachment of the scalp from the skull to place it. Most patients are not willing to have that long scalp scar on their head for the sake of having that material. But for those who are so motivated it can certainly be done. PMMA material is not used for custom implants. That is an historic putty like material used in open applications which relies intraoperative shaping for its limited effects.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have been researching facial implant procedures and came across your work. I am interested in learning more about facial implant surgery and facial contouring in general.
My main question is about your consultation process. During a private consultation, do you also evaluate the face and recommend which implants or procedures might improve facial harmony and overall appearance?
I am asking because I am not entirely sure which implants would be appropriate for my face (for example jawline, chin, infraorbital rim, etc.), and I would be interested in a professional assessment of what could potentially improve my facial balance.
Do you also offer planning or visual simulations to show possible outcomes or different implant designs?
Thank you very much for your time.
A:In the world of facial reshaping surgery, a lot of which is done with implants although there are a few a autologous procedures, it would be very important to know what the patients aesthetic goals are. This is determined preoperatively by imaging of the patient’s pictures to determine their aesthetic targets. There is a common misunderstanding of imaging and the belief that it is done to show outcomes… which is not its purpose as no one can predict with any accuracy what any surgical outcome will be. Conversely it is done to determine what the patient’s goals are from a visual standpoint. Then the operation is designed with these visual targets in mind and hopefully come as close as possible to those imaged goals with the surgical plan.
Such imaging does not guarantee that the preoperative Visual goals will be achieved. But what I do know is you could never hit a target you never had.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have right side cheek bone fracture that is like a dent that makes under my eye appear flat. the injury occurred almost 2 years ago and I am wondering if it can still be repaired or put back together so that it looks normal again I also notice my right starting to become bluey and I’m not sure if it’s do to the injury.
A:Untreated ZMC fractures are not rare and present with contour depression that you describe. There are two approaches to restoring contour after such untreated midface frsctures, recut the bone and reposition it (that fracture is now fully healed) or doing an overlay implant to match the better projection on the opposite side. I have done it many times both ways and it’s fair to say that big custom overlay implants approach is far easier to undergo and gets more accurate results. The only reason to re-cut the bone at this point is if somebody says I simply don’t want an implant. But in so choosing one has to recognize that the magnitude of the surgery, the recovery, and this that it.com is not going to be similar to that of an implant.
That being said one piece of information that is critical In making these decisions is to get a 3-D CT face scan so we can fully appreciate the skeletal differences between the two cheeks sides. That is a scan that can be arranged and ordered in your local geographic area and then sent to me for review.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley,About the bump that is seen and the length of the clavicle, well I was thinking about doing both. (Clavicle reduction and shaving that bump) I am not sure if both are done from the exact incision spot or 2 different incisions would be made for each.
 A:The bump on the end of the distal clavicle requires a small separate incision over it for reduction. The incision for clavicle shortening osteotomies is ‘miles away’ so to speak from the distal clavicle bump.
A:The bump on the end of the distal clavicle requires a small separate incision over it for reduction. The incision for clavicle shortening osteotomies is ‘miles away’ so to speak from the distal clavicle bump.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Revision of sliding chin genioplasty. What can be done to fix an asymmetrical osteotomy?
A: A 3D CT scan is needed to understand the exact nature of the bony asymmetry. But as a general statement the options are either recut the bone reposition it orally or come externally through a submental incision and reshape the bone by shaving. Which one is best depends on the dimensions of the asymmetry.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I had one quick question before booking a consultation. I’m planning to undergo a cheekbone reduction procedure in a couple of months, and I wanted to ask how long I would need to wait after that before proceeding with jaw implants.
Would you be able to provide some general guidance on the recommended time between these two procedures? That would help me plan my consultation accordingly.
I’m planning to undergo the procedures in about 4–5 months. I want to first complete the cheekbone reduction procedure, and then do the jaw implants and rhinoplasty together afterward. So it would be helpful to understand the timeline I should expect.
A: Three (3) months after the cheekbone reduction should be sufficient healing time for further facial surgery.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, how long after a hair transplant is it safe to do a forehead implant?
A: Three months after a hair transplant a custom forehead implant can be surgically placed.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I just have a quick question about penoscrotal webbing surgery. Is general anesthesia mandatory for this procedure, or could it be done under local anesthesia? as I’m very anxious about general with some personal health issues, so I would prefer to avoid it if possible.
A: While I respect your concerns about general anesthesia, and this is not a rare request, I do not perform any form of scrotal surgery under local anesthesia.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Can you ask Dr Eppley about brow bone implant (would he recommend custom or regular) Where would it be inserted from? Is it possible to combine with under + upper eye lift?
A: In answer to his brow bone implant questions:
1) There are no standard brow bone implants. They all have to be custom made.
2) The typical insertion point is a single small incision (2 cms) behind the frontal hairline.
3) Upper and lower blepharoplasties can be performed at the same time as a brow bone implant.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, If I just wanted to bring my hairline down where it peaks upwards. Does Dr. Eppley think a hair transplant or forehead reduction would be better?
A: While hair transplantation is one technique for creating a lower frontal hairline the frequent problem that I see from that technique is the lack of adequate hair density compared to the natural hairline behind it. Combined with the prolonged duration of time it takes to see the result from sufficient hair growth/length it is often an inferior approach to that of the frontal hairline advancement where the hair density is similar and the result is immediate.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have an unaligned chin and I would like to correct it. I’ve seen a general dentist who said my previous orthodontic work looks great so it’s a cosmetic concern. As a child, my chin seemed to be aligned for the most part but after I had braces, my chin moved significantly to the left. I’d like to discuss options for correcting this concern.
A: Thank you for sending your pictures and x-ray. Your chin asymmetry is very clear and your panorex x-ray shows a considerable shift to the left side….which also has a underdeveloped jaw on that same side which is undoubtably why the chin is shifted (see attached panorex analysis). In the correction of any bony chin asymmetry the question always is….do you shorten the longer right side to match the shorter left or lengthen the left shorter side to match the longer right? That choice is one of aesthetic preference.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I recently got a consultation regarding a deviated septum. I had a CT scans done and a confirmation letter from the doctor confirming the deviation. I am looking at going with you regarding this considering your specialties that I could add on to the surgery. I am wanting to get multiple surgeries done at the same time. Procedures: Zygoma reduction Rhinoplasty (including alarplasty + septoplasty) Custom infraorbital implant + canthoplasty Brow bone reduction My questions are: Is all of this possible to get done under one operation? I look forward to hearing from you.
A: It is very common to perform multiple facial structural surgeries at the same time. Brow bone and cheekbone reductions with facial implants and rhinoplasty can all be done during the same operation. The main concept to grasp about multi facial procedures, particularly of a structural nature, is that there will be some profound postoperative swelling and bruising that would be far greater in magnitude and time to go down than if any of these operations were done independently. The impact is on recovery not one of intraoperative technical execution.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I had a kidney transplant and now have severe temporal hollowing. How can I fix it?
A:I will need to see a picture of your temples to evaluate the extent of your temporal hollowing which would determine how it would be best treated. Given that the origin of it is undoubtably extensive fat loss implant augmentation would be the reliable method to improve it. The two pertinent questions in that regard are: 1) what is the exact type of temporal implant that would best treat it and 2) does your medical condition make such surgery reasonable to do without a high risk of infection. Being a transplant patient you undoubtably are on some form of chronic immunosuppression. What that medication is would determine your appropriateness for elective surgery. That and clearance from your transplant doctors.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I came across your studies recently and saw that you did a full midface mask implant using peek and it just so happened that the patient also didn’t want any or minimum lateral expansion in the malar I find myself in the same position recessed maxilla recessed infraorbitals and bad cheekbones which makes my nose appear way bigger than it is as it’s on a flat maxilla I was hoping to ask you how much or a general estimate of such a procedures cost as I Heard it can get quite expensive. Thank you
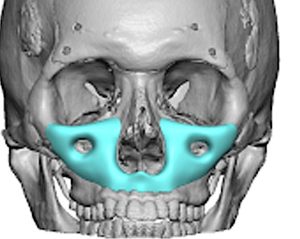 A: I have made many custom midface mask implants, mainly from solid silicone and a few from PEEK. In the US PEEK is twice the cost to manufacture as silicone and its size must be a bit more limited due to difficulty in placing it due to its very rigid construct.
A: I have made many custom midface mask implants, mainly from solid silicone and a few from PEEK. In the US PEEK is twice the cost to manufacture as silicone and its size must be a bit more limited due to difficulty in placing it due to its very rigid construct.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am interested in gluteal implants with fat transfer.
A:Thank you for your inquiry and sending your pictures. I can definitely see the benefits of buttock implants as you do not have a large amount of fat for harvest. When you mention both that is known as composite buttock augmentation where whatever fat the patient has is injected over and around the subcutaneous area in the buttocks while the implants are placed inside the muscle well below where the fat is injected.
The question is not whether that can be done but how much benefit will the fat harvest and transfer be to the overall buttock augmentation effect. In your case I would say that’s an 85:15 ratio meaning 85% of the buttock augmentation effect is going to come from the implants while only a very small beneficial effect will come from the fat transfer.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am unfortunately experience massive post-surgery regret after undergoing vV line surgery in South Korea. While the surgery was performed well, I do not like the aesthetic result. I am now considering implants to restore the jawline. I fortunately have my pre-op CT scans available, and will be looking to have my jaw implants 3D modeled off those pre-op CT scans. However, my concern is overcorrection. I understand that surgical placement can deviate +- 1mm, so would like to avoid looking “wider” than my pre op state.Would this achieve the balance of restoring my previous jaw shape without risking overcorrection? Or is it too conservative? Would following the natural curve/geometry of my pre-op jawline, but at a reduced scale of say about 80%, achieve noticeable/satisfactory results? I also underwent a genioplasty where my chin was set back 3mm. I am not sure if it is due to the jawline shaving, but my chin somehow looks more protruded/bigger despite the setback? Would restoring my jawline without changing the chin make the chin more proportioned? Or would it be advised to restore the chin as well? I have attached CT screenshots.
A: I have seen many the line surgery regret patients from surgery in South Korea who all have a similar story. The surgery is almost always technically performed well but it just turns out to be the wrong operation for the patient’s objectives. And the reason that happens is three fold: 1) the patients objectives through preoperative imaging were never established, 2) the operation is done largely in a cookie-cutter fashion meaning everybody gets the same operation done the same way regardless of their native facial structure or what their aesthetic objectives and 3) by definition Eastern style V line surgery creates a radical change with vertical amputation of much of the jawbone. As a result some patients are going to feel over reduced just as you have.
The only definitive reversal procedure is a custom jawline implant to replace some or all of the missing bone. I would agree that the principal objective is to avoid over correction. There is a reason you had the initial operation and most patients are only looking for partial restoration as there is a reason one had the original surgery. This is indicated by your own theoretical numbers as you think about the dimensions of the jawline and implant replacement.
Lastly I am certain your chin still looks too big because the jawline behind it is not proportionate. The chin setback procedure only treated part of the over reduced problem.
Dr. Barry Eppley
Plastic Surgeon
Can My Small PMMA Bone Cement Occipital Augmentation Be Replaced With A Larger Custom Skull Implant?
Q: Dr. Eppley, I had PMMA bone cement augmentation to the back of my head done in South Korea several years ago. Its effect was very limited and I now wish to replace it with a custom skull implant. I was told at the timeI was told at the time that my result was limited because my scalp was too tight to accommodate much of the bone cement. One question I have is whether the PMMA bone cement will need to be removed and replaced or whether a skull implant can be designed to fit over it. If I get a custom skull implant will I be able to participate in sports and other physical activities? Lastly how durable are custom skull implants long-term?
A:1 )The limitation with PMMA bone cement skull augmentation is not scalp stretch. It is the material itself. When you place a putty like material under the tight scalp the scalp pushes back as the material sets. This produces a limited augmentation effect as the bone cement is flattened. This is only a avoided if one has a full coronal scalp incision where the bone cement is placed in an open setting without the pressure of the scalp on it where its shape and volume can be better controlled. This is where implants have a huge advantage over bone cements but only because of their preform shade but also because they push out the scalp more effectively and resist any rebound scalp pressure. The difference in the volumes obtained between the two methods of skull augmentation are usually 3 to 1 with implants being able to create 3 to 4 times the volume that bone cement can.
2) Whether in considering secondary custom skull implant augmentation the PMMA bone cement is removed or the implant overlaid on the existing cement depends on several factors which can only be better assessed with the 3-D CT scan. I have done it numerous times both ways. But should the cement need to be removed it is done at the same time as the implant placement. The Implant is designed by digitally removing the cement seen on the scan.
3) In my extensive skull implant experience patients are able to go on with life and fully participate in any activities that they so desire.
4) Skull implants are just as durable as bone cement. Both materials are structurally stable and are unable to be broken down by the body.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I’ve attached two photos — one is my natural frontal resting photo, and the other is a conservative mock-up showing improved symmetry and structural balance. I’m trying to understand whether the changes shown in the edited version are surgically achievable and, if so, what procedures would be required. My primary concerns are: • Mild chin deviation from midline • Slight asymmetry in mandibular angle width/projection • Lower-third rotational imbalance • Desire for slightly stronger jaw definition • Subtle improvement in midface support (infraorbital area) without overfilling In the mock-up, the changes are structural rather than exaggerated — centered chin, more even jaw angles, slightly sharper mandibular border, and improved facial harmony while keeping my natural identity. My questions are: 1. Is this level of correction realistically achievable? 2. Would a sliding genioplasty be more appropriate than a chin implant for centering and projection? 3. Would custom jaw angle implants be necessary for symmetry, or could this be addressed with genioplasty alone? 4. Do you see any true midface deficiency that would warrant infraorbital or cheek augmentation? 5. Based on the photos, do you suspect skeletal asymmetry versus soft tissue asymmetry? I am open to obtaining a CBCT scan and cephalometric analysis if necessary to properly assess structural alignment. Thank you for your time — I’m looking for structural harmony and balance, not over-augmentation.
A:Thank you for your inquiry and sending your pictures let me start out by saying that is not a realistic outcome for you with any type of surgery. Those changes look like a completely different person. That being said let’s break down what the differences between your face in the ideal image one which I think you know it is a generalized midface and brow bone lack of forward projection. This is evidenced most clearly buy your significant negative orbital vector. The major change that the ideal error results shows versus you is much more forward projection and fullness for the brow bones down to the base of the nose. Augmentation particularly in the mid face would be beneficial even though it is not going to be a outcome like your ideal image result.
Your chin and jawline concerns are a different matter. You’re trying to make refinements to its shape but without augmenting it in any significant way. That is relevant in the chin we’re what you are seeking is some vertical lengthening which represents a true bony deficiency. Whether that is done best by a custom chin implant or a vertical lengthening bony genioplasty requires a more in depth discussion. But as for the jawline behind it that is best left alone as any efforts to make changes in that area is just as likely to create an adverse outcome as it is to make it better.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have 2 dents on the Left and Right side of my head from cranial surgery when I was a younger I would like to see if it is possible to reduce or remove the dents
A:Thank you for your inquiry. Because you’ve had prior cranial surgery I am going to assume you had a craniotomy and these dents likely represent where the burrholes were made. The question is not whether are these indentations can be filled in for a smooth contour but what is the best method to do it I’ll be at hydroxyapatite cement or some other form of a modified implant. The most prudent approach would be to get a 3-D CT skull scan so we can see accurately the exact dimensions of these defects and then the best treatment to eliminate them can then be determined. I am also going to assume because you had a prior craniotomy that you would likely have an adequate existing scalp scar in which to approach the cranial contouring.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Hello. I have a right forehead and upper brow symmetry that I want corrected. I will attach a few photos showing my asymmetry of my right forehead and upper problem. Thank you.
A:Thank you for your inquiry and sending all of your pictures. In assessing your right forehead asymmetry the upper orbital box is lower than that of the right resulting in a lower eyebrow position as well as a lower lateral brow bone position. The question is whether a unilateral eyebrow left alone would provide significant improvement for you or whether addressing the fullness in the right upper eyelid due to the lower brow bone position would also be necessary. For now I am going to assume the combination both as needed for the purposes of a requested quote.
The one cautionary note that I would mention is that in treating more modest facial asymmetries the result almost has to be perfect for the patient to view it as worthwhile. It is always important to remember the patients are going to critique their postoperative results with the same degree of scrutiny that brought the problem to surgery.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley,Removal of 15 yr old steel metal plates from upper and lower jaws ( under went jaw correction procedure 13 yrs ago) Wanted to check if its possible . Thanks
A:I am sure it is possible to remove them. Do you have any postop x rays which shows the metal hardware? If not you will need to get so am x-ray of which even a standard panorex x ray will suffice.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I would like to discuss whether i can reduce my metopic ridge to achieve a smooth and normal forehead appearance.
A:The success of any form of skull reduction, including a metopic ridge, is whether the bone is thick enough to allow for an adequate and safe bony reduction. That is determined precisely by a 3D CT skull scan with color mapping of its thicknesses.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am considering holistic genioplasty. Due to my relatively strong facial features and overall body structure, my primary aesthetic goal is to achieve a chin that provides a pronounced vertical projection. I am personally drawn to a longer facial appearance and believe that increased vertical chin height would enhance overall facial harmony. Although I have not yet discussed specific measurements in detail with a surgeon, based on personal evaluation, photo editing, and proportional measurements, I find a vertical chin advancement of approximately 10 mm aesthetically appealing. At this level, I observe improved balance between the maxilla and the chin, as well as better harmony in relation to my lips. I understand that horizontal projection is more complex to evaluate subjectively, and at this stage I am less certain about my preference in that dimension. My main questions are the following: From your professional perspective, is a vertical advancement of around 10 mm generally considered excessive or outside the typical aesthetic range? Beyond the aesthetic aspect, is there a risk that such vertical elongation could pull the lower lip downward and potentially lead to lip incompetence or difficulties with passive lip closure? I fully understand that definitive decisions require clinical examination, cephalometric analysis, and surgical planning. My intention is not to predetermine measurements, but rather to better understand what is realistically and safely achievable. For reference, I am also sending three images: One image is taken from a CT scan. During the scan, my head was positioned somewhat awkwardly on the scanning table, which makes it appear slightly projected forward. The second image shows my natural side profile. The third image shows my face with a more neutral head position and an estimated vertical chin projection of approximately 10 mm.
A:I am not certain what makes a vertical lengthening bony genioplasty holistic but I will assume what you really mean is autologous. I believe the three questions you are asking are the following:
1) Is a 10 mm vertical lengthening bony genioplasty a normal procedure that most surgeons perform? I of course can only answer based on what I do and such amounts of vertical bony chin lengthening are very normal in my practice. But then I have a different patient population than most surgeons.
2) Despite the amount of vertical bony lengthening performed, often well in excess of 10 mm, I have never seen the lower lip pull down.
3) By the imaging of your ideal aesthetic goal you should realize that is a much greater amount of vertical bony lengthening than 10 mm and probably is at least 15 to 18 mm.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I’m concerned with an overall deflated look to my face, especially around the under eye area Im struggling to identify if the solution in bone related or soft tissue related. I am young and never had surgery but I’ve done 2 fractional c02 lasers in the past. My goal is to achieve the full look in the picture I included with me when I was younger but I had much better overall volume and under eye support, my eyes also appeared sharper too. Wondering if you have any ideas? Thank you again.
A:Fundamentally what you are referring to are deflated cheeks at least judged by the picture that you are showing when you are smiling. Smiling inevitably inflates the cheeks by pushing the soft tissues upward. While this is obviously a soft tissue issue (loss of volume), given that the bone does not change over time at your young age, treatment options could be either soft tissue (fat injections) or bone -based. (cheek/midface implants, technically cheek implants only sit partially on the bone and their lower half is actually out onto the soft tissues of the cheek) There is even a role for injectable fillers as a test for cheek augmentation effects.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have a bump on my sternum. It’s small, between my breasts, right where the 2 sides of my rib cage connect. The bump is hard like bone, does not move, has no feeling. It feels like bone, not like tissue. Can it be shaved down?
A:This is a prominent sternal edge, which although it can be shaved down and would not regrow, this requires a incision over it to do so. Whether a scar in such a visible area is a good aesthetic tradeoff can be debated. I would question that in a female.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I would like to ask if you perform cranial reduction surgery in adults, specifically procedures aimed at reducing the overall size of the skull. I understand that cranial reshaping procedures may have limitations, and I would appreciate any information you can provide about what is realistically possible in adult patients.
If possible, please let me know what type of evaluation would be necessary and whether international patients can schedule an online consultation.
Thank you very much for your time and attention.
A:Thank you for your inquiry and sending your pictures. The most accurate way to determine whether any skull area can be successfully and safely reduced is to get a 3-D CT skull scan work color mapping of the of the thicknesses of the emnire skull can be done. That will then determine how much and where such bone reductions can be done.
That being said based on my experience of thousands of aesthetic skull reshaping procedures I would question right from the beginning whether your skull is thick enough to allow sufficient bone reductions to make a visible difference. As you can see from your baby pictures this is the natural shape of your skull and, being a female, the skull bones are naturally thinner than that of a male. But for the sake of truly knowing what is and is not possible at the least their merits forgetting a 3-D skull scan so you can know one way or the other with certainty.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley,’ve been looking at your temporal muscle reduction cases and blogs for a while, and I just have a few questions.
Whenever I have my bike helmet on, there’s pressure on both sides of my head. I tried different helmet sizes, but didn’t notice any difference. The pressure goes away when I open my mouth. From what I’ve read, it’s “seeing head width improvement when opening your mouth is due to the thinning of your temporal muscles on the side of your head. They lengthen and narrow when opening one’s mouth widely.”
The pressure occurs around the area you marked in your March 11, 2022 blog.
1. Do you think temporal muscle reduction is a good permanent solution for me? No temporary solutions like Botox.
2. Will removing the muscle create a dip or curve in the supraorbital foramen area?
3. As for pricing, do you have a rough estimate for this whole procedure? Including operating room, anesthesia, etc., costs?
4. Is this something that can be done in your clinic or a hospital? Is an overnight stay needed?
I’ve attached pictures of my face.
A:Thank you for your inquiry and sending your pictures. Everything that you are describing as well as your pictures does substantiate that removal of the posterior temporal muscle mass would provide improvement both symptomatically as well as aesthetically. In answer to your questions:
1) As per my initial description, yes.
2) The supra orbital area is the brow bone and not the temporal area so no change will occur there.
3) Will be provided to you in a subsequent email.
4) this type of surgery is done and my private outpatient surgery center…. which is neither my office or a hospital.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Is there an estimate for when the torso narrowing surgery (more than just ribs 10-12) will be available? I’m pretty interested in the idea.
A:I am not exactly sure what you mean by ‘when will this surgery be available’. Currently I perform 10 rib surgery which consists of shortening osteotomies of ribs 8 and 9 with ubtotal removal of ribs 10 to 12 all in the same surgery in properly selected patients. Based on what I know currently I do not envision benefits to be achieved by rib modifications above rib 8.
Dr. Barry Eppley
Plastic Surgeon