Your Questions
Your Questions
Q: Dr. Eppley, I have done some research on an occipital augmentation cranioplasty for a flat back of the head. I am still about 18 months away from having the money to receive such an operation but in the meantime I have two questions.
1.) What are the long term effects of such a operation?
2) How long is the scalp incision to do the surgery?
3) If I sent in a picture, is there any way to get a good estimate of the size of the needed incision? And is there a way to see what possible results would look like on myself?
Thank you for your time!
A: In answer to your questions:
1) Based on my extensive occipital augmentation experience, I have yet to seen any long-term untoward consequences such as implant problems (infection), skull or scalp issues. There can be some aesthetic issues such as smoothness and edge transition blending into the bone.
2) The size of the incision is going to be based on what implant method is used, preformed implant (6 to 7 cms) or PMMA bone cement. (9 to 10cm) That is predictable up front.
3) Side view pictures can be used to show potential result predictions using computer imaging techniques.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was reading an article by a male to female transgender woman who mentioned having a procedure in Mexico where the doctor broke her lower ribs and wrapped them tightly so that they would fuse together in a more narrow position. I am a slim young woman who would like a more narrow rib cage to give me a longer more narrow waist, but would like to keep my ribs if at all possible. I assume this would be called “rib manipulation” since it is the controlled breaking of the lower ribs. Have you heard of this being done for cosmetic purposes and can you give me information on the pros and cons of this procedure?
 A: What you are referring to would be known as rib reshaping by osteotomies as opposed to the more traditional rib removal procedure to make a more narrow rib cage. The rib as it extends from the spine and around the side of the body is composed of bone (from the spine out to about halfway around the side of the body) and then becomes softer cartilage as it extends to join the sternum. (ribs 10 through 12, also known as the ‘free floaters’ do not extend to the sternum…which turns out to be a very important point in this discussion) If the rib is osteotomized (cut) at the bone-cartilage junction, the cartilaginous end would be more bendable and theoretically could be molded inward as it heals for a more narrow waistline with after surgery binding. This would only apply to the free floating ribs which do not have an attached end. It would not work for any higher ribs because they have a complete arc around the body with a fixed point to the sternum.
A: What you are referring to would be known as rib reshaping by osteotomies as opposed to the more traditional rib removal procedure to make a more narrow rib cage. The rib as it extends from the spine and around the side of the body is composed of bone (from the spine out to about halfway around the side of the body) and then becomes softer cartilage as it extends to join the sternum. (ribs 10 through 12, also known as the ‘free floaters’ do not extend to the sternum…which turns out to be a very important point in this discussion) If the rib is osteotomized (cut) at the bone-cartilage junction, the cartilaginous end would be more bendable and theoretically could be molded inward as it heals for a more narrow waistline with after surgery binding. This would only apply to the free floating ribs which do not have an attached end. It would not work for any higher ribs because they have a complete arc around the body with a fixed point to the sternum.
The advantages to rib reshaping is that it would be less invasive since the ribs are not being removed, would have an easier recovery, may be able to be be done with a smaller incision on each side and would preserve the ribs. The disadvantages is that it is not really clear if it would really work and could be a source of chronic pain if the separated rib area do not heal. (osteochondritis)
Dr. Barry Eppley
Indianapolis, Indiana
Q:Dr. Eppley, I came across your website and your blog. From what I gather, you have extensive experience dealing with complex chin augmentation cases. I have had three chin implants placed in the past (the first was mersilene mesh, replaced with silicone, and then replaced with Medpor), all giving less than ideal augmentation. The silicone one was replaced by Medpor because my chin felt really sensitive and uncomfortable. My doctor said it was due to bone erosion and that Medpor would be better. However, the area still feels sensitive. Currently, I have the RZ Large Medpor Square Chin implant in and it’s smaller than the previous XL silicone chin implant I had, so the chin contour is very strange now as a result of putting in a smaller implant. I saw one p[lastic surgeon who told me that due to all the erosion as a result of the implants, I may not have much bone to augment. I believe that without the implants, my horizontal chin deficiency is around 13mms. My chin could also use a bit of height. Given all this, I have seen one of your cases where you combined sliding genioplasty with an implant. Do you believe this is viable in my situation?
A: Certainly chin augmentation history is complex but you now learned several important issues. First, no preformed off the shelf implant alone can create the chin augmentation effect that you desire. Secondly, the chin sensitivity has nothing to do with the often misused term, ‘bone erosion’ or the implant material. This is more of a soft tissue stretch issue as the implants have gotten larger over your first and original much smaller chin implant.
At this point, you have only two viable options for chin shape improvement. Either get a custom chin implant made from a 3D CT scan that can meet the dimensional needs that you want and now know better or use a sliding genioplasty combined with a chin implant to create a dual autogenous/alloplastic change. How viable the latter approach would be be based on knowing what the bone looks like now. The best way to get that information, which is critical at this juncture so that you have the best chance of having a fourth and final chin augmentation procedure, is a 3D CT scan. This will show the amount and shape of the chin bone as well as the implant that sits on top of it, all of which can be measured to the millimeter to know how likely a sliding genioplasty will ‘work’ and what size implant would need to be used in conjunction to get the chin dimensions that you need.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a minor amount of loose skin under my chin and between my Adam’s Apple that I want flattened. The neck skin has very little, if any, fat. I’m 51 years old and my skin heals from cuts and abrasions very well. The procedure with the lowest trauma and shortest recovery time along with the lowest cost is preferred. Please let me know what procedure you recommend, along with the its recovery time to where I can be out without the procedure being noticeable. Thank you.
A: Thank you for sending the pictures and describing your objectives. The small midline neck wattle poses a bit of a quandary in terms of an ideal procedure. It is not big enough to justify any more major surgery (formal neck lift) but it is significant enough that is it not going too respond to smaller minimally invasive procedures. (e.g., external skin tightening, liposuction etc) Thus in these situations one is ‘forced’ to choose a procedure that is not perfect. (can not create the ideal result or has some trade-offs) This translates into either a submentoplasty with liposuction (otherwise known as a submental tuck up or a direct small neck lift. (most effective since the skin excess is vertical but the scar may not be acceptable in a younger patient)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have questions about jaw angle reduction and temporal implants. Here’s a list of my questions I want to ask:
1. My jaw is still growing and i have braces, will this affect anything? What possible complications can there be? I’m willing to take all the risks and complications. ( i am getting the braces removed soon)
2. If my jaw angle is vertically reduced to make its location higher, will this make it higher from the front view too? Can this be an possible result? By higher i mean close to the ear.
3. Is there any implant to make my head larger or my forehead larger? Since my face is long, i want to make it more proportionate. I have been reading about the temporalis muscle, any implant/augmentation surgery for that
4.what is the difference between having the jaw shaved with a ear incision, and inside mouth incision? Recovery time? Results? Damage? Risks?
5. Here comes the important part… How long is the recovery time? For the ear incision & inside mouth incision? Is there any massage or laser treaments i can take to dramatically reduce the swelling so i can look ‘normal’ after a week of recovery?( i’m willing to pay a lot for any treatments that’ll help ) please include the implant part as well!
6. is it possible to do implant and jaw reduction surgery together? If so how much time will it take and what risks are there?
A: In answer to your questions:
1) Having braces and undergoing orthodontic treatment has no impact on any type of jaw angle surgery.
2) The traditional method of jaw angle reduction surgery does exactly what you are describing. It removes the jaw angle so that the most posterior part of the jaw angle is at the same level as the earlobe. It is important to understand that is so doing the jaw angle will no longer have a square form but a more rounded or sloped angulation.
3) Forehead and mid-temporal augmentation can be done to achieve a larger more pronounced forehead and increase the bitemporal distance for a wider head as judged by its width above the ears.
4) The jaw angle can be reduced by two different surgical approaches. (incisions) The intraoral method is the historic and most common method still used but it does pose challenges for angling the bone cut in an ideal and symmetric manner. The external approach uses an incision behind the ear or just below the ear and provides a much better angle for the bone cut and a quicker recovery (by staying out of the mouth) but runs the risk of causing temporary or permanent facial nerve injury. (that risk is low but is not zero)
5) There is nothing a patient can do to expedite the recovery process which is largely about who long it takes the swelling to go away before one looks human (7 to 10 days) and for its complete resolution. (4 to 6 weeks)
6) It would be common to combine any number of aesthetic craniofacial procedures such as jaw angle reduction and temporal augmentation. The risks of such surgeries, besides infection, are largely aesthetic…symmetry, over/under correction of the desired goals.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read somewhere about temporal implants for head augmentation which I assume is of the muscle. If you add an implant there, wouldn’t it widen my head? And if so, how is it done with what type of implant and location?
A: It depends on what part of the temporal region in which the implant is placed and what type of implant is used. A preformed anterior temporal implant is now available that augments the temporal hollow. (the region between between the anterior temporal hairline and the eyebrows/side of the eye) which often occurs from aging, genetics, drug therapy or neurosurgical approaches. A larger preformed or custom mid-temporal implant is also now available that when placed below the muscle on the side of the head above the ears will increase the bitemporal dimension or width of the head. This as you can see, it is important to know what temporal region of augmentation one desires to select the right temporal implant style and location of augmentation.
Using implants for temporal augmentation is one of the newest areas of craniofacial implant development that has extended the use of implants in the face upward to that of the skull.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like information about brow bone augmentation with calcium hydroxyapatite and customized implants from 3D CT scans. I had a rhinoplasty where the surgeon used transverse and medial osteotomies of the nasal pyramid, and nasal dorsum. I realized that the eyebrows lost support after surgery. The augmentation surgery in the region of the supra-orbital rim or brow ridges with customized implants are made of what material?
 A: Brow bone augmentation can be done by different materials which can also control the surgical approach to place them. (incisional access) The traditional and still most commonly performed technique for brow bone augmentation is through an open scalp incision using either PMMA or hydroxyapatite bone cements. When just the brow bone is being done, hydroxyapatite cement is the material of choice. But when the brow bone is being combined with total forehead augmentation, PMMA bone cement is used due to being a more lower cost material per amount of volume. Performed or custom implants can also obviously be placed through such a wide open exposure. Custom brow bone implants made from a 3D CT scan are always made of a silicone material, primarily due to ease of adaptation to the underlying brow bone and cost. Newer techniques of placing custom or preformed silicone brow bone implants are being developed to avoid the larger scalp incision. (endoscopic frontal and upper eyelid incision)
A: Brow bone augmentation can be done by different materials which can also control the surgical approach to place them. (incisional access) The traditional and still most commonly performed technique for brow bone augmentation is through an open scalp incision using either PMMA or hydroxyapatite bone cements. When just the brow bone is being done, hydroxyapatite cement is the material of choice. But when the brow bone is being combined with total forehead augmentation, PMMA bone cement is used due to being a more lower cost material per amount of volume. Performed or custom implants can also obviously be placed through such a wide open exposure. Custom brow bone implants made from a 3D CT scan are always made of a silicone material, primarily due to ease of adaptation to the underlying brow bone and cost. Newer techniques of placing custom or preformed silicone brow bone implants are being developed to avoid the larger scalp incision. (endoscopic frontal and upper eyelid incision)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Dr. Eppley, I am 20 years old but have had prominent “tear troughs” all of my life, my left tear trough being more prominent than my right. I am very interested in getting injectable fillers for that area. I was wondering if you would be able answer a few questions for me. Would you recommend fillers for my tear troughs? If so, what kind and how much filler would you most likely use? How much would it cost? Is this something that you perform often? Thank you for your time.
 A: Based on just the one side view picture you have shown, you do not have a true tear trough deformity. Rather you have pseudo or seemingly tear troughs when in fact it is caused by something else. What it appears you have is congenital herniated lower eyelid fat pads. This causes a fullness/bulging/bags of the lower eyelids which subsequently creates a tear trough appearance due to the bulge above an otherwise normal tissue area along the infraorbital rim. (lower eyelid socket) Injectable fillers would be contraindicated in this type of lower eyelid anatomy. Conversely you need removal and/or translocation of the lower eyelid fat pads. Some would be removed while a portion would be moved to drape over the infraorbital rim, thus eliminating both the lower eye bulge and the tear trough at the same time. This operation is known as transconjunctival lower blepharoplasty with fat transposition.
A: Based on just the one side view picture you have shown, you do not have a true tear trough deformity. Rather you have pseudo or seemingly tear troughs when in fact it is caused by something else. What it appears you have is congenital herniated lower eyelid fat pads. This causes a fullness/bulging/bags of the lower eyelids which subsequently creates a tear trough appearance due to the bulge above an otherwise normal tissue area along the infraorbital rim. (lower eyelid socket) Injectable fillers would be contraindicated in this type of lower eyelid anatomy. Conversely you need removal and/or translocation of the lower eyelid fat pads. Some would be removed while a portion would be moved to drape over the infraorbital rim, thus eliminating both the lower eye bulge and the tear trough at the same time. This operation is known as transconjunctival lower blepharoplasty with fat transposition.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in fat injections (Lipodissolve) for my lower abdomen. I am done having children and have gained an excessive amount of weight during my pregnancies. I have lost the weight, but the aftermath is stretch marks, loose skin and a “pudge.” My upper abdomen has no stretch marks and is ok. I am trying to find an affordable procedure, that I can handle with minimal downtime, as I have 2 small children.
A: What you need, without even seeing a picture of you and based purely on your rather classic description, is not going to be achieved by an injectable fat reduction technique. Lipodissolve is intended for very small fat collections (like the neck) in which the overlying skin is of good quality. It is completely ineffective for the post pregnancy belly that you are describing. What you need is some form of a tummy tuck which can more effectively deal with the excess/loose skin and fat. With this type of abdominal problem, you either hold out for a tummy tuck one day or do nothing…as nothing will offer any acceptable level of improvement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in occipital augmentation. I have a flattened head at the back which is also assymetrical. It has been a major problem for me for many years. Isolation and depression are the main effects. I have a local surgeon who is tells me a PEEK onlay is the best option. Would you consider this to be better than a filler material. He tells me I will have a transcranial scar and will have to have my hair cut short, preferably shaved. The argument for the onlay is it is difficult to achieve a smooth transition with filler material. I should add he has never done this operation before. Could you give me any advice. I am a little nervous about head shave and a huge incision.
A: After having performed over 100 occipital augmentations with every known material (except PEEK) and method, I can tell you for certain I would never use a hard preformed material like PEEK. (or preformed HTR or preformed acrylic for that matter) The material on insertion is too hard and this requires a maximal incision to get it into place. That may be fine but I don’t know of too many patients that want a full coronal incision for their occipital augmentation.
The two most commonly used and preferred cranioplasty materials in my practice are either intraoperatively fashioned PMMA bone cement or a preformed silicone implant. Either of these materials can be placed with much smaller incisions and work well. I have not seen an infection with either cranial augmentation material to date. This does not mean these methods are perfect (PMMA can have some edge transition issues because of its intraoperative fashioning) but these issues are aesthetic and not of any major medical significance.
FYI, I do not have my patients shave any hair for their skull augmentation regardless of the material or approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What is the difference between the composite facelift using the subSMAS spaces and your technique? Do you make those incisions inside the ear cartilage behind the tragus? Can you please explain the differences between the Deep Plane facelifts? I am basically looking for the most invasive change/longest lasting facial rejuvenation change.
A: Let me provide you with some further comments and my experience with composite acelifting since this is a topic about which you have inquired.
I do not claim to have originality or unique experiences with extended SMAS or sub-SMAS facelifting or composite facelift procedures. The principal motivation of a composite facelift is to bring a rejuvenative effort to more of the midface rather than just the neck and jowl areas. In other words, extending the lifting efforts to more of the central face area. A true composite facelift, in the purest sense of the term, works below the SMAS layer around the cheek, buccal fat pad and deep to the nasolabial fold area. The theory behind such a central dissection is that there is volume descent of the midfacial fat pads which has certainly been shown to be true by anatomic studies. This is not an area that any of the more traditional forms of facelifting strive to reach and treat. By dissecting the fat pad out and lifting and securing it vertically, midfacial descent of tissues is improved.
While this dissection can be done, and a few surgeons certainly tout it, more widespread experiences have been that the risk of injury to the buccal branches of the facial nerve, prolonged operative times, substantial and sustained edema and recovery and the sustainability of the midfacial results do not justify this type of effort in most patients. Other than a very few surgeons, the documented and proven long-term results simply do not justify that effort. The risk of buccal nerve injury, even if temporary, is very real and unsavory for any patient who sustains it.
If it is midface rejuvenation that one is striving for from a deep plane approach, there are more effective and less risky methods that can be combined with a good SMAS dissection. (e.g., subperiosteal midface lift through an eyelid approach)
Thus one should not confuse longevity of a facelift necessarily with the deepest plane approach. There is only so much one can do with the SMAS layer and the intent of a deep plane technique is not necessarily one that ensures a more sustained result because of its extensive SMAS manipulation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had the silicone micro-droplet injections initially done two years ago with no problems. Then I had a second silicone injection into my upper lip six months from which my lip has turned hard and tight. What can I do now to get my lip back to being soft again?
A: Silicone injections may have their role in facial soft tissue augmentation but the lips is the most precarious place to put such a material. When it works it is great but the risk of significant scar reaction/nodules in the lip poses a difficult problem. Whether it is possible to get your lip soft and supple again is hard to predict. Since it is virtually impossible to ever get the silicone material out of the lips, unless there are some distinct hard nodules, all that can be done are fat injections. The objective would be to break up some of the fibrotic scar tissue and layer in some healthy fat grafts that hopefully survive and act as a more supple interface amidst the silicone material which is encased in scar tissue.. This adds new healthy fat cells in and around the scar that would hopefully soften up the lips through the addition of new tissue.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am wondering if I am a candidate for an abdominal panniculectomy procedure. What I mean by being a good candidate is whether insurance will pay for the procedure. removal. I am not sure if I am a grade 2 or 3 pannus.
A: Only your insurance company can truly answer the question of whether an abdominal panniculectomy would be covered but the basic criteria are:
1) an abdominal pannus that covers the groin crease and hangs onto the thighs,
2) an abdominal pannus that is associated with recurrent groin crease skin infections that has a documented three month history of topical skin treatments (non-surgical therapy) that has failed,
3) a BMI of less than 30 or a body weight that in within 20% of their ideal body weight based on standard height and weight measurements.
If one does not fulfill all three criteria, my experience has been that approval for abdominal panniculectomy surgery will be denied. And in some cases, even if all three criteria are met, a denial will still be given. It is also important to check whether your insurance company has a policy exclusion for panniculectomy surgery, as many companies now do, so this may not be a surgical procedure that is even eligible for coverage.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I developed a depression/dent on the middle of my forehead that is circular after the birth of my second son. Whenever I bend over or pressure is applied to my abdominal area, the depression on my forehead fills up with fluid and a huge bump is visible. I have had a CT scan done and the results showed that it was not a dent on the skull surface, however it did not explain the cause. Why do I have it and will it ever go away?
A: The simple answer is I don’t know why you have it nor can I predict with any certainty if it will go away…but if I had to guess I would not think it is going to go away. Since the dent does to have a bone-basis for its presence, one can assume this is a soft tissue deficiency. That is predictable since if the dents as due to a bone issue, it would have been present essentially since birth. (short of some traumatic event) I have no doubt that the dent fill sour when you bend over but that is not because it fills with ‘fluid’ per se. That is probably due to blood vessel engorgement from the pressure which would be more obvious when the tissues are thinner.
What I would initially is to some temporary filler injections to make it more level and probably resistant to that bulging engorgement effect. If that us successful the you can eventually move on to a fat graft or fat injections for a more permanent result once you are assured that a soft tissue fill solves both problems.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an endoscopic mid face lift two months ago. Actually I had minimal problem but I decided to go through this surgery. Actually it did not help me that much. I did not have any complication but it just was not very helpful for me. As my swelling went down I do not see any noticeable changes at all. Now the problem is that my upper lip is very stiff and it is hard for me to move it. I am at 2 months post surgery and it has only improved by about 30%. The approach was through my mouth. Is this caused by the Endotine device or because the dissection was through my mouth and temple. Is it normal to have a stiff upper lip after midface lift? Your answer will be very highly appreciated.
A: Most effective midface (cheek) lifts do involve a combined temple/scalp and mouth approach. While this does create some temporary mouth soreness and upper lip stiffness, it has not been my experience that the upper lip stiffness is prolonged out to months after surgery. The Endotine device is positioned up on the zygomatic bone so that device is not the source of prolonged upper lip stiffness…or should not be. It is the path of dissection and how much tissue was released in doing so that is the cause. This is an issue for which only time and further healing can provide a resolution.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about temporal reduction surgery.
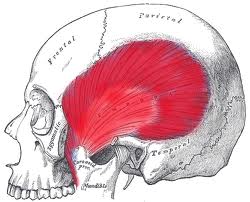
1 What is the thickness of the temporalis muscle?
2. I have been searching for the this kind of surgery on the Internet and I have not found many surgeons who deal with this, why? Is it because it’s the most difficult operations of all or is it because there is no big demand for this procedure?
3. Do you have any materials (video, pictures) of this kind of operation?
4. When the temporalis muscle is removed , would it influence any other muscle or anything related to that section of head?
5. In your message to me you wrote : ” A vertical incision is made and the entire posterior temporalis muscle is removed and the underlying bone burred as much as possible” What is burred?
6. Is there any chance that you can make a picture for me of how I would look like after the surgery ?
7. This operation can not cause any damage to my brain?
 A: In answer to your questions:
A: In answer to your questions:
1) The thickness of the temporalis muscle differs depending on its location. The average thickness of the temporalis muscle above the ear is usually around 7mms or so.
2) Temporal muscle reduction surgery is not commonly practiced due to lack of awareness and patient demand, it is not complex surgery.
3) I do not have any videos of this type of surgery but do have intraoperative pictures of it.
4) Removal of the posterior portion of the temporalis muscle has no functional effects on the workings of the muscle and its jaw opening/closing function.
5) Some temporal bone burring is done is some cases.
6) I can do some computer imaging if I have a frontal view picture of you.
7) This is an extra cranial procedure not an intracranial one so there is no risk of any brain injury.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about my breast augmentation procedure that I forgot to ask about during my consultation. My left breast is slightly bigger than my right breast and I was wanting to know if this would affect the overall look of my breasts after getting implants? It is only a slight difference in size, and is only noticeable from a side view. I am just afraid that it will affect the look of my breast post surgery.
 A: Breast asymmetry is very common amongst many women undergoing breast augmentation and is a very important aesthetic issue to identify before surgery. As a general statement, all implants do is to take the breasts you have and make them bigger. They are nothing more than a mound enlarging device. Thus whatever breast shapes one has when they are small will become bigger. This means that for some women a small breast asymmetry may become more noticeable afterwards. (i.e., the breast asymmetry becomes bigger) In other cases, enlarging the mounds may make the slight breast asymmetry go away completely. The difference in what may make breast asymmetry more or less noticeable after augmentation is whether the asymmetry is due to mound size differences or whether it is due to a difference in the horizontal position of the nipples. Slight mound size differences will usually go away even with equally sized implants on both sides. (the key is the term ‘slight’ mound size differences) Conversely, horizontal nipple level differences will usually get worse with implant enlargement as the mounds enlarge. For this reason if I see such differences I point that out to patients during their consultation and usually recommend a small nipple lift at the time of breast augmentation to even out the horizontal nipple levels to avoid the so-called ‘cock-eyed’ breast look when nipples are at different levels on the breast mounds.
A: Breast asymmetry is very common amongst many women undergoing breast augmentation and is a very important aesthetic issue to identify before surgery. As a general statement, all implants do is to take the breasts you have and make them bigger. They are nothing more than a mound enlarging device. Thus whatever breast shapes one has when they are small will become bigger. This means that for some women a small breast asymmetry may become more noticeable afterwards. (i.e., the breast asymmetry becomes bigger) In other cases, enlarging the mounds may make the slight breast asymmetry go away completely. The difference in what may make breast asymmetry more or less noticeable after augmentation is whether the asymmetry is due to mound size differences or whether it is due to a difference in the horizontal position of the nipples. Slight mound size differences will usually go away even with equally sized implants on both sides. (the key is the term ‘slight’ mound size differences) Conversely, horizontal nipple level differences will usually get worse with implant enlargement as the mounds enlarge. For this reason if I see such differences I point that out to patients during their consultation and usually recommend a small nipple lift at the time of breast augmentation to even out the horizontal nipple levels to avoid the so-called ‘cock-eyed’ breast look when nipples are at different levels on the breast mounds.
I don’t specifically remember any significant asymmetries in your breast mounds that would justify either a nipple lift on one side or the use of different implant volumes. But since you have noticed a slight asymmetry in your breasts and it is of concern to you, I would lastly mention an old breast augmentation adage…‘breasts are not twins but sisters’. This means that if they are slightly different before breast augmentation surgery, they will continue to be different after surgery. One should not expect perfect symmetry from surgery when the breasts are exactly perfectly similar before surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible to correct mild midface hypoplasia with fillers? Will it be a result that is approximate to what facial implants can do?
A: If you add enough volume of injectable fillers in the cheeks, orbital rim and paranasal regions, some midface hypoplasia correction (increased projection) could be achieved. But no filler is permanent and substantial filler volume would be needed. It is also important to remember that gel-like hyaluronic acid-based fillers (e.g., Juvederm Voluma) do not provide the same type of push on the soft tissues that implants do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 29 years old and I have 3 kids. They are all good size and I’m small build so therefore my skin has stretched out bad!!! Also as a result in having kids I have an umbilical hernia. Can that be taken care of as well at the same time as the tummy tuck?
 A: It would be very common in tummy tucks and abdominal panniculectomies for a woman to have a concurrent umbilical hernia. The hernia can be repaired at the same time as the tummy tuck procedure and is an ideal time to do given the very open exposure. In some cases there is a risk of loss of the umbilical stalk with the hernia repair dependent on the size of the umbilical hernia.
A: It would be very common in tummy tucks and abdominal panniculectomies for a woman to have a concurrent umbilical hernia. The hernia can be repaired at the same time as the tummy tuck procedure and is an ideal time to do given the very open exposure. In some cases there is a risk of loss of the umbilical stalk with the hernia repair dependent on the size of the umbilical hernia.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can oval shape buttock implants rotate? Is there an amount of time that goes by that rotation is no longer a concern because they are now in their permanent place? If so, how long until that happens? If they rotate can you push them back manually without another surgery?
 A: Oval, sometimes called natural, shape buttocks implants can certainly rotate if they are placed in the subfascial location rather than the intramuscular position. That risk is greatest during the first several months after surgery but the risk is lifelong since they are not textured implants but have a smooth surface. You may be able to push them around back into the place but they can just as easily rotate again. But if the buttock implants are placed in an intramuscular pocket, the chances of inadvertent rotation are significantly reduced because of the more constricted pocket space.
A: Oval, sometimes called natural, shape buttocks implants can certainly rotate if they are placed in the subfascial location rather than the intramuscular position. That risk is greatest during the first several months after surgery but the risk is lifelong since they are not textured implants but have a smooth surface. You may be able to push them around back into the place but they can just as easily rotate again. But if the buttock implants are placed in an intramuscular pocket, the chances of inadvertent rotation are significantly reduced because of the more constricted pocket space.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had upper jaw surgery and a sliding genioplasty done four years ago when I was 18 years old. I have never been happy with the results on my chin and would like it reversed, is this possible? The surgery left indention’s on the sides of my chin and a upturned appearance to the chin.
 A: A Sliding genioplasty can be reversed in the same fashion as it was done originally…the bone is cut and moved back to its original position. I suspect based on your description of the chin issues (notch deformities on the distal ends of the cuts and an upturned chin) that the angle of the genioplasty cuts was too steep. This moves the chin as much upward as it brings it forward and leaves a v-shaped notch on the lower edge of the jawline where the chin bone moved forward.
A: A Sliding genioplasty can be reversed in the same fashion as it was done originally…the bone is cut and moved back to its original position. I suspect based on your description of the chin issues (notch deformities on the distal ends of the cuts and an upturned chin) that the angle of the genioplasty cuts was too steep. This moves the chin as much upward as it brings it forward and leaves a v-shaped notch on the lower edge of the jawline where the chin bone moved forward.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was searching for the information regarding facial sagging after cheek bone reduction surgery. I suffer from facial sagging after cheek reduction surgery that I had four months ago. Even though my bone is tightly fixed, sagging is quite severe and it keeps getting worse. I think it might be because of the loss of skeletal support. He didn’t reposition the unit of my cheek bone but removed part of my front cheekbone by dissecting it as an ‘L-shape’. The worst part is that only the right side of my face is sagging and I don’t know what to do. I’ve been searching for some doctors who are renowned for face lifting. They said that they need to release the zygomatic ligaments and lift the SMAS up as well as the skin. I can see that you are the one who understand the right reason and solution of this problem. So I will be truly thankful if you spare some time to give me some advice. Thank you so much.
A: I am sorry to hear of your unfortunate unilateral outcome from your cheek bone reduction surgery. The obvious origin of the problem is the loss of ligamentous attachments of the overlying soft tissues to the cheek bone as well as the loss of skeletal support for them. It is interesting, assuming that the same bone reduction techniques were done on both sides, that only one side of your face has this tissue sagging problem. This shows how precarious the soft tissue attachments are to the bone and how slight differences in dissection techniques can make a big difference in their outcomes. As has been pointed out to you, the key to improvement is not just the skin shifting but the need for deeper soft tissue repositioning. The only tissues that possible to relocate are the SMAS layer. But moving the SMAS layer without giving it skeletal support will not provide a significant improvement. The first place to start is to have a good idea of what the underlying bone support looks like between the two sides. I would recommend that you get a 3D CT scan to visualize your cheek bone anatomy as it is now. Then with that information a more complete surgical plan can be devised as to how to manage the bone and the soft tissues.
Dr. Barry Eppley
Indianapolis, Indiana