Your Questions
Your Questions
Q: Dr. Eppley, I am interested in having a tummy tuck but do have a bit of a twist with my medical history. I have rheumatoid arthritis and have been on Xeljanz 10mg twice a day to control my symptoms. It has controlled them fairly well and I am not keen on potentially going off of it to have surgery. Can I have a tummy tuck while on this medication?
 A: Xeljanz, known generically as Tofacitinib, is a recently approved drug (2012) for the treatment of rheumatoid arthritis. It works as an inhibitor of the enzyme janus kinase 3 (JAK3) which interferes ultimately with DNA transcription in the cell nucleus. It helps in arthritis because it inhibits production of inflammatory mediators in joint tissue. As an inhibitor of the inflammatory process, the drug is known to increase the risk of opportunistic infections such as tuberculosis, cancers and lymphomas.
A: Xeljanz, known generically as Tofacitinib, is a recently approved drug (2012) for the treatment of rheumatoid arthritis. It works as an inhibitor of the enzyme janus kinase 3 (JAK3) which interferes ultimately with DNA transcription in the cell nucleus. It helps in arthritis because it inhibits production of inflammatory mediators in joint tissue. As an inhibitor of the inflammatory process, the drug is known to increase the risk of opportunistic infections such as tuberculosis, cancers and lymphomas.
But as it relates to surgery, the key questions are does it present an increased risk of infection or in any way impede wound healing?This would be particularly relevant in a large healing wound like that of a tummy tuck. There is no specific information in the medical literature that addresses the specific effect on wound healing of the Xeljanz medication. This is likely because it is relatively new although almost all anti-rheumatoid drugs, with the exception of corticosteroids, have a similar void of specific information on their effects on postoperative wound healing.
What I can find is from the newsletter Drug Safety Quarterly Fall 2013 issue which has an article entitled ‘Wound Healing and Anti-Rheumatic Drugs’ authored by Drs. Goodman et al from NYU. From it I quote…
‘Healthy wound healing proceeds through an inflammatory phase, followed by wound remodeling and finally re-epithelialization of the skin edges. These are the normal sequential stages of wound healing. Patients with rheumatoid arthritis (RA) are often on multiple medications to control their symptoms. These medications may include analgesic, anti-inflammatory, biologic or synthetic disease-modifying antirheumatic drugs. (DMARDs) With the exception of methotrexate, there are very few controlled studies that have evaluated the effects of these medications on wound healing and infection risk after surgery.’
‘…with the exception of methotrexate, there is a lack of data regarding optimal practice for perioperative management of antirheumatic treatment in RA patients undergoing surgery. Existing data, however, indicates that methotrexate may be continued throughout the perioperative period for otherwise healthy individuals. For the other anti-rheumatic drugs, while continuing medication may hamper wound healing and predispose to infections, discontinuation may lead to disease flare, which increases the need for corticosteroids or other medications that may also increase the risk for inadequate wound healing and infection to regain disease control. Moreover, there is no consensus among the various rheumatic disease societies regarding optimal practice. Although there are clear effects of anti-rheumatic therapy on wound healing and clear infection risk, the role of RA inflammatory activity on wound healing, infection, and rehabilitation should also be considered. For surgeries such as the implantation of a prosthetic joint, where surgical site infection carries significant morbidity, current practice favors a conservative approach.’
This summary comes from an institution that is performing joint replacements in orthopedic surgery. So these types of patients have significant functional and pain issues related to joint dysfunction. So accepting whatever increased wound healing or infection risk may be worth the trade-off for the benefits. Tummy tuck surgery is much more elective and those unquantified risks must be considered even more carefully.
This is a good discussion you should have with your rheumatologist. He/she probably will not be as understanding about tummy tuck surgery as the need for a joint replacement. But in the end you should follow their advice. The only thing we know for sure is that you are at some increased risk of potential wound healing problems or infection if choosing tummy tuck surgery while on Xeljanz but the magnitude of that risk is unknown.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw surgery just over a year ago and it left me with some irregularities. This led me to get chin and paranasal implants a month ago. While they have provided some improvement and there is still some swelling, they still have not completely solved the appearance of nasolabial folds and pre-jowls.
 I now suspect that this may be a soft-tissue problem. However, because I am only 25 years old such soft tissue deficiencies seem unusual. Anyway, I’ve googled facial fat grafting and this image really pinpoints the areas I would like to build up and bring forward (the direction of the arrows). My biggest questions are as follows:
I now suspect that this may be a soft-tissue problem. However, because I am only 25 years old such soft tissue deficiencies seem unusual. Anyway, I’ve googled facial fat grafting and this image really pinpoints the areas I would like to build up and bring forward (the direction of the arrows). My biggest questions are as follows:
1) Could my soft tissue issues have been caused by my previous underbite (thereby affecting soft tissue development) or the jaw surgery itself?
2) Given my age, can fat grafting be done for these regions? If so, how much volume of fat is usually required?
3) Instead of fat grafting, are permanent fillers an option? Alternatively, are there any different implants that can be placed in these regions?
4) I have implants near these areas. Can fat grafting be done safely without infecting my implants?
Anyway, I also had some fat grafting done to my brow ridge and central forehead to make it look masculine. My surgeon did a decent job, but I’m noticing that insufficient fat was placed in the central forehead (the area between the two eyebrows and just above the nose), which means that my outer/lateral brow ridges are more augmented than the inner portion, causing it to look like I’m constantly frowning. I’m looking to add more fat to the central forehead, but I understand that a revision should only be done a few months later. Regarding this, I have a couple of questions:
5) It has only been 4 weeks since the fat grafting, can I use temporary fillers to augment the deficient areas in the meantime?
6) If so, will fillers affect how my fat graft survives at this stage?
A: I am going to assume that your jaw surgery was orthognathic surgery, possibly a mandibular advancement osteotomy. But that issue aside, let me address your specific facial fat grafting questions.
- The cause of your nasolabial folds and prejowls is impossible for me to comment on since I don’t know what you looked before your jaw surgery or your most recent facial implant surgery.
- While injectable fat grafting can be done for these areas, how retentive it will be is somewhat dependent on your body habitus. Thin young people usually have a poor rate of fat graft survival and retention. The fat graft volumes needed for the nasolabial folds are 3 to 5ccs per side. The prejowls usually require a similar amount of injectate.
- There are few permanent fillers available in the U.S. and, even if there were more, I would not use them. All of the so-called permanent fillers run the risk of lump and nodules. While more often these do not occur, but if they do they are problematic to treat. Other styles of facial implants may indeed be more effective than what you have such as a true maxillary implant. (combined medial and lateral maxillary coverage which is much ore comprehensive than a simple paranasal style which I find archaic and inadequate for many midfacial hypoplasia needs)
- Fat grafting is done above the level of the bone where the implants reside so they are not in danger of being accidentally injected.
- I would probably wait another month before placing synthetic fillers into the fat grafted areas. The fat grafts are still healing and there is an increased risk of causing an infection by introducing another material into these areas.
- At 8 weeks after fat grafting, injectable fillers will not have any adverse effects on the outcome of the fat grafting.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 26 year-old male from Europe. I have a major concern about the proportionate shape of my temples, specially above ears. The muscle in the region is very thick and also the bone is protruded to large extent which makes heads looks very big. So I have decided to contact you as I can see you are the only one having expertise in this area of plastic surgery.
I have some questions regarding this:
1) How much muscle can be reduced..does this involves any risk?
2) How much muscle can be reduced?
3) How about narrowing the width of the forehead near the hairline?
4) Will this make considerable changes in my appearance?
5) What will be the recovery time?
6) What will be the cost of the surgery?
7) Iit possible to come for consultation and surgery once as coming to US twice will not be feasible?
A: In answer to your questions about temporal reduction surgery:
1 and 2) Usually the entire posterior belly of the temporalis muscle above the ears is removed. This constitutes a thickness of at least 5 to 7mm per side, sometimes even more depending upon the thickness of the muscle. I have seen temporalis muscle as thick as 10mms in some patients. Removal of this portion of the temporalis muscle causes no functional loss of jaw movement or any other disability.
3) Reducing the temporalis muscle near the eye and just below the forehead is a different matter than that at the sides of the head. This muscle can not be surgically reduced. It must be treated with Botox injections if any reduction in thickness is to be achieved.
4) Changing the convex shape of the head above the ears to more of a straight line (and hence narrowing the head width) is seen by those so afflicted as providing major improvement in their concerns.
5) Temporal reduction surgery has a very quick recovery time with little discomfort and minimal swelling. The change in temporal appearance is immediate.
6) I will have my assistant Camille pass along the cost of the surgery to you on Monday.
7) There is no need to come initially for a consultation. All before surgery discussions etc can be done by e-mail or Skype video. You would only need to come for the surgery and could return home within 48 hours after the procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about a custom jawline implant.
1) Does having a custom jawline implant that increases chin dimensions of 15 mm or so place undue stress on the bone? Presumably not, otherwise this wouldn’t be discussed as an option.
2) You had mentioned off the shelf mandibular angle implants are two wide in many cases. Would that hold true in my case?
3) Since my previous implant created a pocket, will this be favorable to swelling in that area?
4) What type of lead time do you need when designing this implant prior to surgery? I don’t think I’m as concerned about quantifying millimeters as other patients may as I am with having some broad criteria of the implant not looking overly large and unnatural.
5) You had mentioned getting Voluma prior to surgery would not affect things. There’s a surgeon locally adding this to his practice and providing this for free if I want to slightly accentuate the jaw angles. I don’t know if this issue still holds true with this custom implant option. I would assume in the worst case scenario this product could be dissolved, however, I don’t want to risk affecting this process in the future or perhaps even the 3D scan somehow.
 A: In answer to your custom jawline implant questions:
A: In answer to your custom jawline implant questions:
- A larger implant, like the custom jawline implant, distributes its forces (stress) on the bone over a very wide surface area. Thus one does not see the traditional implant settling phenomenon that can occur from an isolated chin implant.
- Most patients, men or women, need a vertical lengthening component to their jaw angles not just width. Most current styles of jaw angle implants only add width and very little if any length to the jaw angles.
- Having an indwelling implant with an existing pocket will tend to create less swelling in that area with a new implant than during the initial implant placement surgery.
- From obtaining the 3D CT scan to having the sterile implant in hand ready for surgery is a three week process.
- Getting a synthetic injectable filler, like Voluma, will not interfere with the images obtained in a 3D CT scan. It will also not interfere with placing any jawline implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I came across your web site while googling for plastic surgeons. Six months ago I got hit in the forehead with a beer bottle (blunt trauma). The plastic surgeon only looked at the injury two days later and applied micropore tape rather than stitches. Around a month ago, I started going to to a few local plastic surgeons to see what could be done about the car. All the surgeons having different ideas on what to do. I really don’t want to have to travel overseas for treatment, but I do want the very best results (as I’m stuck with my face the rest of my life).
It seems like the local surgeons have the following two schools of thought:
1) To wait until a year has passed, and re-evaluate. I do not like this option, as it seems to be getting worse as time goes on, not better
2) To cut out the scar and re-stitch it. Within this there are 3 opinions:
a) Cut out the scar, and remain with a horizontal line which conforms to my face’s natural lines.
b) Cut out the scar in it’s current orientation (around 45 degrees), because it can not be adjusted to a horizontal orientation without doing a z-plasty
c) Make a horizontal cut through the middle of the scar, leaving a small vertical mark on the top and the bottom (which the plastic surgeon claims will disappear)
Within the opinions above:
1) No surgeon was exactly sure what is causing the scar to bulge. Some claim it is excess scar tissue from not being stitched initially after the injury. Others claims it is a cyst that has formed. Another claims it is some kind of “fluid” under the scar. Keep in mind that the bulge currently feels more like a hardish jelly that a hard bump.
2) I have asked each one regarding geometric broken line scar revision. Some just refer to the Z-plasty or W-plasty when I mention that word. They claim that W-plasty is not necessary as the scar is small and with a straight cut, it will eventually result in a smooth white line. Some even suggest that making any jagged patterns will make it more noticeable.
3) I have also asked regarding dermabrasion and/or laser. All of them have said that as long as the surgery is ok, and healing goes normally, they do not see any reason for dermabrasion or laser. Only if the scar looks like it is becoming hypertrophic will they apply some extra treatment.
4) I have also asked all of them about botox before surgery. They all claim it is unnecessary.
5) Regarding final outcome, some surgeons claim the scar will be a fine white line, others claim it will almost disappear, and others say “we can assume it will be better than it is now, but no guarantees”. From one end of the spectrum to the other?!
So my question is:
1) Is there any way to get it horizontal without Z-plasty?
2) Would a straight cut be better than GBLR?
3) Is demabrasion/laser really necessary?
4) What is your personal recommendation at this point? Am I taking a risk doing it locally, and if not, which school of thought should I trust?
Sorry for the long winded message. Just spent hundreds of dollars and hours
trying to find someone who is confident and know what they are doing,
but it seems hard to find someone who can suggest the best and most
optimum treatment locally.
Thanks in advance for your help/advice.
A: I will take your very detailed description and various opinions and summarize your forehead scar revision issues/recommendations succinctly.
This is a hypertrophic scar and would be expected given the original unrepaired wound. There is no mystery as to why it is there.
Totally removing the scar (excision) is the most expeditious and effective method to getting to an eventual better scar. Everything else is just wasting time and effort.
The excision should be based on a stair step pattern closure to at least get 50% of the scar horizontal.
Botox injections should be done at the time of scar revision. (not before so the wrinkles lines are well demarcated) This will provide several months of tension free healing in the critical few months after the procedure
Microdermabrasion or light laser resurfacing may or may not be needed afterwards based on how it heals.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a custom jawline implant option and have some questions about it. You have mentioned that this particular implant will be able to address all of the following aesthetic issues of my jawline:
- Address the approximate 10 or 12 mm horizontal chin deficiency
- Address the approximate 5 to 7 mm vertical chin deficiency
- Address vertical and width dimensions of the mandibular angle (curious how this is accomplished if I visualize this as a chin implant with very long wings as this looks quite different than an off the shelf mandibular angle implant)
- Account for any existing jaw asymmetries
- Creation of a continuous jawline from to the chin back to the mandibular angle
I can see that this certainly seems favorable considering the decreased operating room time and relative cost between alternatives involving multiple procedures and implants as you explained.
A: You have thoroughly hit on all of the aesthetic benefits that a custom jawline implant would provide. And it is also the only way you could achieve all of these dimensional jawline changes with a single implant. Such an implant is not really an ‘extension’ of a chin or jaw angle implant. Rather it is an implant that accentuates the entire jawline rather than just being a forward extension of a jaw angle implant or a backward extension of a chin implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had cheek implants and facial liposuction two weeks ago. Since my procedure I can’t feel my upper lip and it still doesn’t move like its supposed to with no improvement since the first day after surgery. Is it highly likely something was transected or the fat closer to my lip was removed along with the nerves? The doctor did it through the same incision used for my cheek implants implants rather than one further back and it concerns me both sensory and motor function are absent from the same spot and there has been no recovery in more than two weeks.
A: It is not rare that numbness and facial muscle movement are temporarily impaired after cheek implants, particularly when it is combined with facial liposuction. It would be highly unlikely that any nerves were transected. But it could easily take up to three months or longer after the procedure for both normal facial feeling and lip movement to return. Two weeks is way to early for these small facial nerves to ‘wake up’ and begin functioning. Your sense of what is normal and how nerve recovers is understandably limited to this present experience. But it takes much longer to return to normal that most patients think after any form of midface surgery including cheek implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a chin implant revision. I had a silicone chin implant a few years ago which was terrible and looked awkward. So 1 year ago I replaced it with a Medpor chin implant which is no doubt much much better than that original nightmare. But this Medpor chin implant does not look rigid as opposed to silicone. It looks more like a “U” shape instead of “V” shape. The edges are not sharp as opposed to the famous MB picture either. So what is your suggestion, is it possible to add some medpor cuts to the edges to make it look more sharp do you think? Or is it a common issue with all Medpor chin implants? Thanks a lot for your great experience and knowledge.
A: The success of any chin implant to create a specific chin shape is not material based. It depends on the shape of the implant and the thickness of the overlying soft tissues and underlying bone shape. You did not state what style of Medpor chin implant you have which would be helpful to know. But Medpor implants in general are thicker and ‘bulkier’ than most silicone implants because the material from which it is made is machined into shape rather than poured into a mold like silicone.
The ideal chin shape image you are showing is more of a square shape unlike yours which is more circular and long. Whether your existing chin implant can be shaped into that form would depend on knowing what shape and thickness your existing implant is. It certainly could be improved but tot what degree can not predicted without further information. Medpor implants are generally bulky and some improvement in its form can usually be obtained by giving it a more angular shape.
I would point out that shaping an indwelling chin implant has its limitations based on the existing incision length and access to it. It is often better to place/replace an implant that has been shaped before it is put in with the dimensions that one wants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had cheek and paranasal implants placed in another state 4 days ago before flying back (1 hour flight). I think I have developed a slight cold, and have a slight runny nose while coughing up some phlegm too. My biggest worry right now is that there is some ‘squishiness’ when I press on my left cheek. Are there signs of a cheek implant infection, and what can be done for it?
Anyway, I’m still taking my antibiotics as prescribed, and there are no other symptoms (no redness, excessive swelling or fever). I’m hoping that I don’t have to get these implants removed, which is why I’m seeking your counsel with regards to what I can do.
Thanks for any help rendered!
A: I would not consider this squishness to be a sign of cheek implant infection. Most likely it is due to the positioning of the implant and/or a little fluid around it since it is so early after surgery. Many cheek implants are placed partially off the bone and/or are not screwed into position. This will allow the implant to ‘float’ around for awhile until scar tissue settles and secures it down. Further healing will also allow any fluid around the implant to be resorbed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in jaw angle implant revision surgery. I just got jaw angle implants with facial liposuction. I’ve always wanted a more defined jawline. So I got the procedure done. My doctor did the type of jaw angle implant that widens. But I wanted the one that lengthens and wides a bit. So already he didn’t do the one I wanted and he went too wide. It’s 4 days after surgery. Is it bad to remove implants and replace with others? Is their risk involved? I’m very unhappy about how he did this.
A: Th first thing to realize is that it is just four days after your jaw angle implant surgery. This is a time period of maximal swelling so it would be impossible to have any idea as to what the final result would be. It generally takes four to six weeks to see the final result. So the final result may or may not be what you want.
But let’s assume for the sake of this discussion that your current jaw angle implants are inadequate. It is very straightforward with no increased risk over the original surgery to replace your jaw angle implants with a new design. Because you have an existing implant pocket, the amount of swelling and recovery would be significantly less than the initial implant surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been interested in liposuction for years because I feel my love handles / flanks make me look terrible. I knows I need to lose about 20 lbs but am not motivated because I believe the flanks will never go away. Admittedly even in basic training 20 years ago when I was very lean, but still had flanks. With that said, it has been a dream of mine to remove the ‘love handles’ even if it meant still having a little belly. My hope is that this change would motivate me to lose enough where I am happier with myself. I am 5’ 9″ and 195 lbs and still have decent muscle mass for age 39. With all that being said, how much could I realistically expect to have removed? Thank you for your assistance and honest feedback.
A: The flanks are one area of the body where the most aggressive liposuction can be done in a man or a woman because there is virtually no risk of any skin irregularities. Flank and back skin is fairly thick so it contracts down very well, particularly in men. I could not give an estimate as to how much fat can be removed unless I could see some pictures of the problem areas. Computer imaging can be done to give you a good idea as to what the result would like. Flank or lovehandle liposuction takes about one hour to perform under general anesthesia.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had cheek implants done and I look terrible. I’ve never been this hideously ugly, and other people seem to instantly love their results, so I’m really scared and really depressed. I hope to eventually move my face normally and that sensation will return. I don’t know why he augmented one side such that the two sides will be off balance butI could see from day one before the swelling set in that the two sides were not even.
A: With time and healing your face will move again normally but that will be a process of up to three weeks or more. Feeling will also return normally but that will take a little longer.
I have done this type of facial implant work (cheek implants) for a long time and I can tell you that not everyone instantly loves their results. Swelling and bruising causes a lot of facial distortions and it can be unnerving to see your face this way. But what you see now is not necessarily what it will be four to six weeks from now. But that is understandably hard for many patients to see. There are many patients who feel just like you do at this point so what you are experiencing is not unusual at all.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had cheek implants and facial liposuction done just a week ago. While my face is distorted from the swelling I already know that the cheek implants are not right. They are asymmetric and in the wrong place. After speaking with my surgeon, he stated he would only remove the old 2.5mm implants and would be unwilling to place new implants at the time of removal. What I don’t like is that there is still no projection to my midface in profile, which is my primary reason for undergoing the procedure. I’m curious if a 4mm silastic implant would provide a better result. I wanted to look like Jessica Biel or Megan Fox. Please let me know your opinion. If your professional opinion is to keep the 2.5mm, then I would still like to try a filler for the area directly below my eye to give my midface more projection and also to discuss refining my chin/jaw.
A: I am glad to hear that you have gotten to speak to your original surgeon as he is the one who knows what type of cheek implants were placed (I know its Medpor but don’t know the style)
While your cheek implants can certainly be replaced (cheek implant revision), an important issue would be to known what is the starting point. While the swelling in your face has come down, there is still about 50% swelling to resolve. So my concern is that the shape of your face is not completely ‘known’ nor is the final effects of what the current cheek implants will look like. That makes to hard to know what cheek implant style to change into when you are working with a ‘moving target’ as the swelling goes down and the final shape of the current implants become evident. What you don’t want to do is to change the implants and then find out what you have changed into is no better for a different reason.
It is also unclear as to what you mean by more ‘midface projection’. The term midface is an ambiguous one and means different things to different people so more clarification on this issue is needed. Cheek implants in general do not create midface projection, they create cheek projection.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am very interested in the rib cage narrowing surgery to achieve a thinner waistline. I am a very slender individual with a wide ribcage, so unfortunately diet and exercise alone have not been able to give me my desired silhouette. I have experimented in corsetry and own a few but the discomfort, inconvenience, and lack of real results have left me desiring something more extreme. I’m not sure which ribs I need removed but by my count it would be the 10th 9th and 8th ribs. As you can see from my pictures I do have a quite bulky rib cage so I believe narrowing anywhere above the floating ribs on its straight line would give me the desired results.
 A: Ribcage narrowing, also called waistline narrowing, would be fair to be called a bit of an extreme approach. While there is a small scar on each side to access the ribs for removal, it can be a very effective procedure. It can certainly be uncomfortably initially as taking bony ribs is not without some discomfort from removing the attached intercostal muscles. Usually no more than two ribs are taken in any one location as the ribs do serve a purpose, they provide protection to what lies underneath. In addition you usually do not remove above rib #9 to stay below the level of the pleura/apices of the lungs.
A: Ribcage narrowing, also called waistline narrowing, would be fair to be called a bit of an extreme approach. While there is a small scar on each side to access the ribs for removal, it can be a very effective procedure. It can certainly be uncomfortably initially as taking bony ribs is not without some discomfort from removing the attached intercostal muscles. Usually no more than two ribs are taken in any one location as the ribs do serve a purpose, they provide protection to what lies underneath. In addition you usually do not remove above rib #9 to stay below the level of the pleura/apices of the lungs.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have cheek asymmetry and wonder what type of cheek asymmetry surgery would fix it. My left hand side cheek is more bulged out than my right one. I also have a dimple on my right cheek and there is not one on my right cheek. In my pictures you can see what I mean by the differences in my cheeks.
A: I can see that your left cheek does indeed bulge out more than the right and there appears to also be some other soft tissue asymmetries as well. The question is whether this bulge is due to a bony prominence or the overlying soft tissue. (or even a combination of both) I suspect it is due to bone because it is over the cheek bone prominence. A bone reduction (shaving ) may be all that is needed improvement. A cheek dimple could be made at the same time of desired.
To verify that it is indeed bone, a 3D CT scan would answer that question unequivocally. Bulging of the cheek prominence often occurs because of the union of the zygomatic and maxillary bones which form the anterior cheek prominence. Often it can be bowed out due to how the facial bones developed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 25 years old male inetrested in lip scar treatment. When I was 12 years old I had an accident which resulted in the need stiches in my upper lip. Thereafter my moustache hairs will not grow in this area. Is there any chance for regrowth of hair in that scar part. Please let me know as that would be very kind of you.
A: Upper lip lacerations in men very commonly result in beard hair loss. This is because the scar tissue that repairs the lip tissue does not have hair follicles in it. The wider the scar is the bigger the lack of beard hair will be and the more visibly apparent the lip scar will be. Beard hair will not regrow into a lip scar. Hair follicles must be in the tissues to do so. Your options are either scar excision to bring the hair bearing lip skin closer together or hair transplants into the lip scar itself. Most of the time lip scar revision would be the appropriate initial course of treatment particularly if the lip scar has any width to it and is more vertical on orientation on the lip.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty to narrow my chin. I told the doctor that them when I smile, my face looks big at the side of the chin so he mentioned that he’s gonna cut or reshape the bone there and remove some muscles. I’ve attached the photo of the before and after surgery. Because after I did this, every time I smile or not even smiling, I see my line around my chin area looking like someone took a bite out of it and the bone there’s gone. Also I feel like my chin is more narrow not like before. I really don’t mind if it’s making my chin comes forward, but not like before. It is possible to reshape the chin bone in any way. Or just simply just cut the middle and then put the bone in front?
A: Based on your pictures and the x-rays, what you had done was a sliding genioplasty that brought your chin forward and up a bit as well as had a central wedge taken from it to narrow it. This is clearly evident in the x-rays and by the plate fixation used. What this has done, and is not uncommon, is to narrow the chin but there is a step off at the back part of the osteotomy cuts. I see where no other bone has been removed…and certainly no muscle or soft tissue has been removed. This has left you with a chin that is now too narrow for the rest of your jawline…hence your interpretation that it looks like a bite has been taken out of the jawline behind the chin. (hollow part)
You have two options to consider for your sliding genioplasty revision. Probably rather than moving the bone back, which can be done, you could simply fill in the bone defects left along the jawline. (provided you are satisfied with the way the front part of the chin looks)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a short lower jaw and feel that it needs improved from front to back. This includes the chin and jaw angles. I am uncertain as to the best way to do it. As a man, I do not lie walking around with a jawline that is not very masculine. My biggest concern about any type of jaw implants is that they might become loose or dislodged if I get hit or participate in any sports. What is your recommendation?
A: There are three different approaches to your type of jawline enhancement and include the following:
1) Standard chin and jaw angle implants (3 pieces)
2) Sliding genioplasty for chin and jaw angle implants (2 pieces)
3) Custom wraparound jaw implant (1 piece)
There are advantages and disadvantages to each jawline enhancement method. Your biggest concern about implant dislodgement would be completely avoided by a single one-piece jawline implant that has a custom fit by computer designing. This is because it is a single implant that with its wrap around effect has more surface area for implant fit and this becomes very difficult to ever move from its custom fit location.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for a surgeon who can help me to decide how to improve my scar. I know it is hard to evaluate a scar from just pictures. I have a small scar 0.5 cm on my chin resulted from squeezing and scratching the spot and I got it infected. It was 10 years ago.The scar was just a very little raised and became white. I had radio frequency treatment done 5 months ago. And after a month the scar became a little more raised. I attached the picture of the scar so you can have a look. It is a slightly hypertrophic scar.
I got a lot of different options from the doctors. Nothing has been done yet, I am very careful as the scar is on the face. A few doctors recommended to me that laser CO2 fractional would be the option for me and some of them said that excision of the scar will give me a more significant improvement and I should have a scar as fine line. Two doctors recommended steroid injection to flatten my scar but it will not reduce the white color.Another doctor said that it could make another complications like pigmentation surrounding skin. I do not want to try laser CO2 as I had radio frequency treatment done on my face and my scar became a little more raised and white.
I would go for excision but a few doctors said that my scar could look worse because of the location. One doctor explained to me why he would not do excision as the scar is on the chin and there is no loose skin so if he cuts it out it will have to be closed under tension which could make my scar worse.
Another surgeon told me something different please read below:
‘The existing scar is not big enough that there should be much tension on the surgical scar. With a good surgeon, and a good post-operative healing process, should leave you with a fine white line. I would place it in a curve or oblique line that parallels the curve of your chin pad – this is called a resting skin tension line (RSTL). The deeper layer of sutures should be dissolving, but the last layer at skin level should be non-dissolving for the best chances at a good result.’
Another surgeon told me this:
‘One of the surgeons you have seen is right to say that it does depend a little on how much loose skin there is but in general, there is ample laxity in facial skin to perform an excision of this kind without distortion. So long as the new scar is placed carefully in relation to the natural lines of relaxed skin tension the new scar should be favorable, but it will still be a scar.’
What do you think about it?
What would you recommend after excision, i need to know your opinion to get the best care after excision.
One of the surgeons wrote me this:
‘I ask my patients to cover their wound/scar with Micropore for the first 3-4 weeks as this provides some mechanical protection to the wound, and traps some sweat and waxes from the underlying skin, which is good for the scar.’
Silicone sheeting is applied after 3-4 weeks, as the scar undergoes a change in how it is behaving. For the first 3-4 weeks, a scar is depositing collagen bundles in a random manner to build up strength. After that 3-4 week,s it enters the remodelling phase, where the scar starts to pull down the random collagen bundles and arrange them in the best possible direction for the scar. At this stage, the body also send in new blood vessels to help that process. This is when scar management such as scar massage and silicone sheeting will help. Starting to do these things earlier than 3 weeks can weaken the scar and cause it to widen.
What do you think about it?
A: The short answer is…if you want to have any chance of a visible improvement in your scar, you have to excise it. There is not an issue of inadequate skin laxity ti close it. Scar revision has ittl chance to make it worse, it is only a question of how much improvement can be gained.
When it comes to scar therapy, I do not believe there is any magic. Given the very small size of the scar, I would recommend topical steroid gel applied at night only.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I did lots of research before my jaw angle implant surgery. But I guess not enough to find the difference between lateral jaw implants to vertical implant. I have a high jaw, and I didn’t want it much wider. Just further down with slight wider. I told my surgeon this and he said that there’s only one implant for the jaw. The lateral one. I now can see the width that I will have but of course there’s swelling. The width is too much and it’s not down where I was wanting my jaw to be. So that’s why I would like to do the vertical lengthening jaw implant. I’m trying to see if my doctor can remove it this week. My doctor did not place screws with my implant, he just placed the silicone implant in the pocket of my jaw. I don’t think my doctor was an expert on jawline enhancement and I think that was my first mistake. I’m actually freaking out thinking I just ruined my face. Is it possible to fix my jaw implant problems? Not only did he do the wrong implant, he also went too large. Please comfort me with info and what I can do.
A: Unfortunately your research on jaw angle implants was indeed inadequate. Of the three decisions you have to make about jaw angle implants, the very first one is whether the implants should be of the lateral width style or the vertical lengthening style. The second decision is what sizes or thicknesses should theses styles be. Lastly, there is the issue of material choice. (silicone vs Medpor)
By far the most common jaw angle implant is the vertical lengthening style with some width. (but usually less than that of the vertical length increase) Pure width (lateral width) jaw angle implants are used in 10% or less of all jaw angle implants in my experience.
You did not ruin your face, the implants can always be converted to the vertical lengthening style at any time. With your facial shape, you likely need a 7mm vertical lengthening and 3mm width style jaw angle implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a lot of orbital bossing of the skull which may be pinching the supraorbital nerves causing daily migraine pain. I guess this surgery would be called forehead reconturing/orbital bony contouring/brow bone reduction of that region. I was hoping to get a surgery that could take care of the functional as well as the aesthetic. I have a 3D Ct scan of that region and was wondering what a rough estimate might be for that surgery. Would insurance cover this procedure? I know that the same incision is made across the hairline for both the migraine surgery and the recontouring of the orbital bony area of the forehead. Listed below are descriptions of the surgery I have in mind. Thanks!
1. Forehead reconstruction or cranioplasty where the glabella bone is taken apart, thinned and re-shaped, and reassembled with small titanium wires or titanium microplates and screws.
2. Or the compression technique in appropriate cases where the wall of bone is first thinned and weakened, and then compressed into place. It then heals in the new position.
A: Certainly orbital rim recontouring by brow bone reduction and decompression of the supraorbital nerves can be done at the same time. Only brow bone reduction uses an open scalp incision. Isolated supraorbital nerve decompression for frontal migraines is usually done by an endoscopic limited incision technique. But the open approach does afford great access to the nerves for the best decompression possible.
Most brow bone reductions are best done by an osteoplastic flap technique where the outer table of the frontal sinus is removed, reshaped and then put back in its reshaped form by either resorbables sutures or very plates and screws.
Neither is aesthetic brow bone reshaping or supraorbital nerve decompression for migraines covered by insurance. Prominent brow bones are not a recognized craniofacial deformity by insurance companies. Nerve decompression for migraines is currently viewed as ‘experimental’ surgery without long-term clinical studies to be currently viewed as an approved medical procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in facial reshaping surgery. I can not figure out what my face needs to look better. I’d really appreciate you taking your time for this. I have been given different surgery options from doctors here in Australia. However my opinion is that the best doctors are located in America, especially for facial surgery. It has been recommended to me that I have cheek implants, buccal lipectomy and a chin implant. But I want to know your opinion since you are regarded as one of the best surgeons in the world for facial reshaping surgery.
A: In looking at your pictures, your facial reshaping/restructuring goal would be to shorten your longer face and provide some more central projection. You have a more flat paranasal/midface and thus you have to be careful with how you change things to not look worse. I would recommend the following:
1) Chin augmentation but by sliding genioplasty as your chin needs to come forward but should become vertically shorter not longer. (implants tend to make the chin longer or at least neutral in vertical length)
2) Malar/Submalar implant augmentation with emphasis on providing with anterior projection not so much width
3) Avoid a buccal lipectomy. That would be one of the worst things you can do to a face that already lacks projection and could easily end up looking gaunt.
4) Paranasal augmentation to build out the base of the nose and the maxilla. This complements what the dimensional changes of the cheeks and chin and avoids ‘leaving the area between the two behind’.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have read about your custom jawline implants (wrap-around style) on exploreplasticsurgery.com and was wondering if these implants can increase the width of the jaw angle as well as the vertical height or is it just the vertical height that these can change? I’m also trying to establish the drawbacks (apart from cost) of these wrap around implants over the separate jaw/chin implants.
A: Custom jawline implants can be made to any dimension that is aesthetically desired in either height, width or shape. The actual cost difference between a custom implant and standard implants is much less than one would think, with only about a 20% cost difference at best. While the cost of the custom implant is higher, it takes only 1/2 of the operative time to do…thus explaining why the cost difference is not that extreme. Having done hundreds of combination chin and jaw angle implants, I now find that single custom jawline implant produces a better aesthetic result with a very low risk of malposition/asymmetry compared to using three separate pieces. (1 chin and 2 jaw angles) In fact, it is virtually impossible to have a malposition of a custom implant because of the precision fit and design.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in getting a forehead reduction with the hairline lowering included. However the bossing of my forehead is the entire bone, top middle and down to the bottom over the brow bones. Can these areas be burred and reshape with the same approach you use on the brow ridge and eye orbits sockets as well?
A: The entire forehead can be reduced by burring. The only exception or caution would be over the brow bones where the underlying frontal sinus exists. The bone on the front of the frontal sinuses (brow bones) is usually very thin and may be only 3 to 4mms thick before the frontal sinus is encountered. A lateral skull film x-ray is needed before surgery to measure the thickness of the bone to see how much it can be reduced by burring. If more reduction is needed than just burring can allow, then an osteoplastic bone flap technique is needed to maximize the lower end of the forehead reduction. In a woman this is rarely needed however.
That is a long answer to say that a burring technique can sufficiently reduce the amount of bossing of the frontal bone and is often done on conjunction with a hairline lowing/advancement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in the Brazilian Butt Lift and would like to know how many procedures you have performed? I have attached two pictures and would like to know what kind of results you would expect with my body type. I am not wanting a big Kim Kardashian booty just some volume to add some shape. Looking at my attached pictures do you think this is achievable?
A: It is a good thing that your Brazilian Butt Lift (BBL) objectives are not like that of Kim Kardashian as you simply do not have enough fat to harvest to achieve that amount of buttock size increase. The success of BBL surgery depends on two important factors, how much fat does one have to give and how much fat will survive after being processed and injected. When you realize that less than 50% (at best) of what comes out as liposuction harvest ends up as buttock volume addition, the reality of what is achievable by the BBL procedure comes into focus.
What one means by ‘just some volume to add some shape’ is open to interpretation, the question is really whether the procedure is worthwhile. There is only one guarantee with the BBL operation and that is the body contouring that results from the liposuction harvest. When one does not have a lot of fat to harvest and process, a realistic buttock augmentation goal should be ‘just something more than what I have’. As that is the only assurity you can get from the procedure.
Many successful buttock augmentation results occur from the combination of reducing what lies around the buttocks and augmenting what lies within…more so than a real substantial buttock size increase. Such would be the case with your body type.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I did not know i could have cheekbone reduction in the U.S.. I had it done in Asia where my friend had that done too. I am of Asian descent and I have wide prominent cheekbones. I had the cheekbone reduction procedure without plates and screws and now I am afraid of non union of the bones, misalignment and dislocation of the fragments of the zygomatic arch. I hear a clicking sound. My surgeon in Korea says it’s normal and will disappear, but I wanted a second opinion from you.
if you don’t use fixation how you make sure the bones stay in place how you prevent sagging and scleral show after the cheekbone is collapsed. Once you push the zygoma arches in and there are gaps and dents, does new bone is created in years to fill in those gaps or do they remain depressed?
A: Cheek bone reduction surgery can be compared directly to have a facial fracture…albeit a surgically controlled one. The best way to ensure that the bones stay in the desired position and heal is to use some form of bone fixation. (plates and screws) The clicking you hear is the bone segments that are unstable and are moving with their edges rubbing together.
Since the zygomatic arches are not functionally loaded bones, like the lower jaw for example, one can argue that it is not critical that they are stabilized. They will eventually go on to heal even if it is by fibrous rather than bony union. When it comes to cheek bone reduction, however, the position of the bone is just as important as whether it heals. Sagging or dropping of the bone is associated with soft tissue sag and even potentially lower eyelid sag. This is why some form of bone fixation should be done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, After perusing your blog extensively (thank you for it, it has been a tremendous help!), I’ve finally decided to get cheek implants. My issue is that I had a sinus infection 2 weeks ago,and my doctor put me on antibiotics for a week. It has since cleared up and I don’t have any symptoms of sinusitis anymore. As I will be getting my cheek implants in two weeks, will enough time have passed for me to get the implants safely, or will I be an increased risk of infection due to the prior sinusitis?
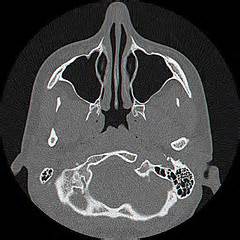 A: It would be logical to assume that there could be a correlation between cheek implants and maxillary sinusitis. And certainly one should not undergo any elective cosmetic procedure if any active head and neck infection is ongoing. While they are anatomically very close, the placement of cheek implants on top of the zygomatic bones and the sinuses located below and behind the front wall of the maxilla are distinctly separate areas that do not connect. Even an active maxillary sinus infection does not contaminate the tissues where a cheek implant would be placed.
A: It would be logical to assume that there could be a correlation between cheek implants and maxillary sinusitis. And certainly one should not undergo any elective cosmetic procedure if any active head and neck infection is ongoing. While they are anatomically very close, the placement of cheek implants on top of the zygomatic bones and the sinuses located below and behind the front wall of the maxilla are distinctly separate areas that do not connect. Even an active maxillary sinus infection does not contaminate the tissues where a cheek implant would be placed.
But having a two week period where the maxillary sinusitis is cleared would be prudent. But the typical antibiotics given for facial implants (usually Keflex) is not the type of antibiotics that should be prescribed for maxillary sinusitis since it does not provide adequate antimicrobial coverage.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am in search of a very skilled revision rhinoplasty surgeon and am impressed by your work.
I had my first septorhinoplasty with right inferior turbinectomy around 18 years ago. My nose looked wide and had bulbous tip and pinched nostrils on birth and I had breathing problems. During first surgery the doctor took too much of my bridge away. My breathing problems got a bit better but my nose looked totally deformed. I am of course very depressed due to that and am very much judged by people in life when they see me before I even open my mouth due to my appearance.
I long to have a normal nose, I would like to have my bridge built up. These pictures were taken in 2012 just before tip plasty. I am sending the same pics to you for evaluation as the doctor did not even touch the bridge, only the nasal tip (hook) noted on left profile was made smooth, but everything is the same no difference at all. I did not want my bridge touched at that time as I thought things will get worst but am prepared now to take the plunge with the right surgeon.
I was told that I did not have any septal cartilage left for grating but never had ear or other cartilage or implant used so far. What do you think could be done to improve my nose? I do not want any synthetic implants in my nose, thus the only option is my ear or rib cartilage?
I want to have an elegant nasal bridge, and have the pinched nostrils look better and start to live life better. I would be ever so grateful for your feedback.
A: In looking at your pictures, you do need a dorsal augmentation by a cartilage graft and a rib donor source would be the best and really only good choice in your revision rhinoplasty. This provides an adequate amount and shape of the dorsal augmentation that you need. You would also benefit by alar rim grafts to provide improved support to your nostril rims so they do not collapse downward. Slivers of rib cartilage graft would be an excellent source of the straight thin grafts that are needed here.
Dorsal augmentation would bring the upper two thirds of your nose in better balance/proportion to the tip.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if you have and do perform surgery on cutis verticis gyrata. If so I was wondering some of the details and and maybe some idea of the length and width of a post op scar.
A: I have performed surgery on this exact scalp condition in the past and can make the following comments about it.
Cutis verticis gyrate (CVG) is a most unusual although not rare scalp condition of which its cause is unknown. But how it presents with ridges and creases is well known and that the scalp tissue thickens to create it. Treatment options are very limited with the most common approach in limited scalp areas of excision. This may be satisfactory if the rolls are limited to the back of the scalp in a horizontal orientation. But for many cases of cutis verticis gyrata the scarring is likely prohibitive. A more innovative approach is the use of subcision (release) of the creases combined with fat injections. This ‘scarless’ approach has no real downside other than its effectiveness and would be the preferred approach in larger areas of scalp involvement in which excision is not an option.
I would need to see some pictures of your scalp CVG to see which, if any treatment options, may be worthwhile for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in lower eyelid bag removal surgery. I have dreadful eyebags that won’t go away. I have tried all the home treatments and nothing works. I’m a young female at age 28 and the bags last all day. There are two bags under each eye. The past two years everyone has been asking if I’m exhausted or sick. It’s really affecting my self esteem. Can you help me? I am getting married next year and and I don’t want him to lift the veil and see my tired baggy eyes. Thank you for your time.
A: Lower eye bags are the result of fat that is sticking out from under the eyes and pushing out on the eyelids. Because there is a ligament of sorts that normally holds back this fat, when it protrudes it is known as herniated infraorbital fat. Usually it occurs as a result of aging but there are younger people who have it naturally. Known as congenital herniated infraorbital fat, I have seen and treated it as young as 14 years of age. Because you would be normally too young to have this as a result of aging, we can assume this is the result of a congenital weakness in the lower eyelid tissues that can not contain the fat.
This is a very correctable problem. There are two lower blepharoplasty techniques that can be used to eliminate the lower eyelid bags. The first is a transconjunctival (inside the eyelid incision) to just remove the protruding fat. (transconjunctival lower blepharoplasty) This is usually the best approach for younger patients or those that have no excess lower eyelid skin. The other approach is to reposition rather than remove the excess lower eyelid fat done through either internal or external incisions. The decision between the two depends the patient’s anatomy, age and their facial type.
Dr. Barry Eppley
Indianapolis, Indiana